Professional Documents
Culture Documents
Cancer Pancreatico
Cancer Pancreatico
Uploaded by
Jossue Espinoza FigueroaOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Cancer Pancreatico
Cancer Pancreatico
Uploaded by
Jossue Espinoza FigueroaCopyright:
Available Formats
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1605
review article
Medical Progress
Pancreatic Cancer
Manuel Hidalgo, M.D.
From the Centro Nacional de Investi-
gaciones Oncolgicas and Hospital de
Madrid, Madrid; and Johns Hopkins Uni-
versity School of Medicine, Baltimore.
Address reprint requests to Dr. Hidalgo
at 1650 Orleans St., Rm. 489, Baltimore,
MD 21230, or at mhidalgo@cnio.es.
This article (10.1056/NEJMra0901557) was
updated on July 14, 2010, at NEJM.org.
N Engl J Med 2010;362:1605-17.
Copyright 2010 Massachusetts Medical Society.
D
eaths from pancreatic ductal adenocarcinoma, also known as
pancreatic cancer, rank fourth among cancer-related deaths in the United
States. In 2008, the estimated incidence of pancreatic cancer in the United
States was 37,700 cases, and an estimated 34,300 patients died from the disease.
1
Pancreatic cancer is more common in elderly persons than in younger persons, and
less than 20% of patients present with localized, potentially curable tumors. The
overall 5-year survival rate among patients with pancreatic cancer is <5%.
1,2
The causes of pancreatic cancer remain unknown. Several environmental fac-
tors have been implicated, but evidence of a causative role exists only for tobacco
use. The risk of pancreatic cancer in smokers is 2.5 to 3.6 times that in nonsmok-
ers; the risk increases with greater tobacco use and longer exposure to smoke.
3
Data are limited on the possible roles of moderate intake of alcohol, intake of cof-
fee, and use of aspirin as contributing factors. Some studies have shown an in-
creased incidence of pancreatic cancer among patients with a history of diabetes
or chronic pancreatitis, and there is also evidence, although less conclusive, that
chronic cirrhosis, a high-fat, high-cholesterol diet, and previous cholecystectomy
are associated with an increased incidence.
4-7
More recently, an increased risk has
been observed among patients with blood type A, B, or AB as compared with
blood type O.
8
Approximately 5 to 10% of patients with pancreatic cancer have a family history
of the disease.
9
In some patients, pancreatic cancer develops as part of a well-
defined cancer-predisposing syndrome for which germ-line genetic alterations are
known (see Table 1 in the Supplementary Appendix, available with the full text of
this article at NEJM.org). In addition, in some families with an increased risk of
pancreatic cancer, a genetic rather than an environmental cause is suspected. The
risk of pancreatic cancer is 57 times as high in families with four or more affected
members as in families with no affected members.
10
The genetic bases for these
associations are not known, although a subgroup of such high-risk kindred carry
germ-line mutations of DNA repair genes such as BRCA2 and the partner and local-
izer of BRCA2 (PALB2).
11-13
In recent years, there have been important advances in the understanding of the
molecular biology of pancreatic cancer as well as in diagnosis, staging, and treat-
ment in patients with early-stage tumors. Minimal progress has been made, how-
ever, in prevention, early diagnosis, and treatment in patients with advanced disease.
This review summarizes recent progress in the understanding and management
of pancreatic cancer.
The Biology of Pancreatic Cancer
Data suggest that pancreatic cancer results from the successive accumulation of gene
mutations.
14
The cancer originates in the ductal epithelium and evolves from pre-
malignant lesions to fully invasive cancer. The lesion called pancreatic intraepithe-
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1606
lial neoplasia is the best-characterized histologic
precursor of pancreatic cancer.
15
The progres-
sion from minimally dysplastic epithelium (pan-
creatic intraepithelial neoplasia grades 1A and
1B) to more severe dysplasia (pancreatic intraepi-
thelial neoplasia grades 2 and 3) and finally to
invasive carcinoma is paralleled by the successive
accumulation of mutations that include activa-
tion of the KRAS2 oncogene, inactivation of the
tumor-suppressor gene CDKN2A (which encodes
the inhibitor of cyclin-dependent kinase 4 [INK4A]),
and, last, inactivation of the tumor-suppressor
genes TP53 and deleted in pancreatic cancer 4
(DPC4, also known as the SMAD family member
4 gene [SMAD4]).
16
This sequence of events in
pancreatic carcinogenesis is supported by studies
in genetically engineered mouse models in which
targeted activation of Kras2 with concomitant in-
activation of Trp53 or Cdkn2A/Ink4A results in the
development of pancreatic cancer that is identical
to the cognate human disease.
17-19
Other prema-
lignant lesions of the pancreas, which are less
well characterized, include intrapancreatic muci-
nous neoplasia and mucinous cystic neoplasia.
20
Almost all patients with fully established pan-
creatic cancer carry one or more of four genetic
defects.
21
Ninety percent of tumors have activat-
ing mutations in the KRAS2 oncogene. Transcrip-
tion of the mutant KRAS gene produces an abnor-
mal Ras protein that is locked in its activated
form, resulting in aberrant activation of prolifera-
tive and survival signaling pathways. Likewise,
95% of tumors have inactivation of the CDKN2A
gene, with the resultant loss of the p16 protein
(a regulator of the G1S transition of the cell
cycle) and a corresponding increase in cell pro-
liferation. TP53 is abnormal in 50 to 75% of tu-
mors, permitting cells to bypass DNA damage
control checkpoints and apoptotic signals and
contributing to genomic instability. DPC4 is lost
in approximately 50% of pancreatic cancers, re-
sulting in aberrant signaling by the transform-
ing growth factor (TGF-) cell-surface recep-
tor. A recent comprehensive genetic analysis of
24 pancreatic cancers showed that the genetic
basis of pancreatic cancer is extremely complex
and heterogeneous.
11
In that study, an average of
63 genetic abnormalities per tumor, mainly point
mutations, were classified as likely to be relevant.
These abnormalities can be organized in 12 func-
tional cancer-relevant pathways (Fig. 1). However,
not all tumors have alterations in all pathways,
and the key mutations in each pathway appear
to differ from one tumor to another.
A characteristic of pancreatic cancer is the
formation of a dense stroma termed a desmo-
plastic reaction (Fig. 1).
22,23
The pancreatic stel-
late cells (also known as myofibroblasts) play a
critical role in the formation and turnover of the
stroma. On activation by growth factors such as
TGF1, platelet-derived growth factor (PDGF),
and fibroblast growth factor, these cells secrete
Figure 1 (facing page). Components of Pancreatic Cancer.
Pancreatic cancers are composed of several distinct
elements, including pancreatic-cancer cells, pancreatic-
cancer stem cells, and the tumor stroma. A recent
analysis of 24 pancreatic cancers suggested that the
mature pancreatic-cancer cell carries on average 63
genetic alterations per cancer; these alterations can be
grouped in 12 core signaling pathways.
11
These results,
if confirmed in larger studies, would indicate that pan-
creatic cancer is genetically very complex and hetero-
geneous. Thus, effective treatments will probably need
to attack several targets (with combination regimens)
and may require individualized therapy. A small group
of cells (5%) appear to have cancer stem-cell features
that render them capable of asymmetric division, en-
abling them to generate mature cells as well as cancer
stem cells. These stem cells may be identified by the
expression of specific membrane markers and can re-
generate into full tumors on implantation in immuno-
deficient animals. Pancreatic-cancer stem cells are resis-
tant to conventional treatment, but they have alterations
in developmental pathways such as Notch, hedgehog,
and wingless in drosophila (Wnt)-catenin that may
result in new therapeutic targets. Pancreatic cancer is
characterized by a dense, poorly vascularized stroma;
this microenvironment contains a mixture of interact-
ing cellular and noncellular elements. Autocrine and
paracrine secretion of growth factors such as platelet-
derived growth factor (PDGF) and transforming growth
factor (TGF-) and cytokines results in continuous
interaction between the stromal and cancer cells. Pan-
creatic stellate cells are a key cellular element in the
stroma. They are characterized by the expression of
desmin, glial fibrillary acidic protein, and intracellular
fat droplets. On stimulation by growth factors, pancre-
atic stellate cells express smooth-muscle actin and
produce abundant collagen fibers that contribute to
tumor hypoxia. ALDH+ denotes aldehyde dehydroge-
nase, CTGF connective-tissue growth factor, CXCL-12
chemokine 12 ligand, EMSA electrophoretic mobility-
shift assay, EMT epithelial-to-mesenchymal transition,
FGF fibroblast growth factor, GTPase guanosine triphos-
phatase, HGF hepatocyte growth factor, HGF-met hepa-
tocyte growth factor mesenchymalepithelial transition
factor, JNK Jun N-terminal kinase, MMP matrix metallo-
proteinase, SPARC secreted protein, acidic, cysteine-rich,
TIMP tissue inhibitor of MMP, TNF- tumor necrosis
factor , and VEGF vascular endothelial growth factor.
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1607
collagen and other components of the extracel-
lular matrix; stellate cells also appear to be
responsible for the poor vascularization that is
characteristic of pancreatic cancer.
24,25
Further-
more, stellate cells regulate the reabsorption and
turnover of the stroma, mainly through the
production of matrix metalloproteinases.
26
The
stroma is not just a mechanical barrier; rather, it
constitutes a dynamic compartment that is criti-
cally involved in the process of tumor formation,
progression, invasion, and metastasis.
22,23
Stromal
cells express multiple proteins such as cyclooxy-
genase-2, PDGF receptor, vascular endothelial
growth factor, stromal cellderived factor, chemo-
kines, integrins, SPARC (secreted protein, acidic,
cysteine-rich), and hedgehog pathway elements,
among others, which have been associated with
a poor prognosis and resistance to treatment.
However, these proteins may also represent new
therapeutic targets.
27,28
The role of angiogenesis in pancreatic cancer
remains controversial. Although early data sug-
gested that pancreatic cancer is angiogenesis-
dependent, as are most solid tumors, treatment
Tumor
Tumor
Pancreatic-cancer cell
Pancreatic-cancer cell
Pancreatic-
cancer
stem cell
Tumor stroma
TGF-
MMPs
Integrins
Matriptase
Interleukin-1 and
interleukin-6
PDGF
TNF-
CXCL-12
Insulin-like growth
factor 1
HGF
Cancer pathways:
Apoptosis
DNA damage repair
Cell-cycle control
RAS
TGF-
Cell adhesion
Hedgehog
Integrin
JNK
Wnt-catenin
Invasion
Small GTPases
Pancreatic-cancer
stem cell:
Self-renewal
15% of cell population
Markers: CD24+, CD44+
EMSA, CD133+
ALDH+
Resistant to chemotherapy
and radiotherapy
Cancer stem-cell pathways:
CXCR4
Hedgehog
BMI-1
Wnt-catenin
EMT
Notch
Stromal cells:
Fibroblasts
Pancreatic stellate cells
Endothelial cells
Immune and inflammatory cells
Adipocytes
Extracellular matrix:
Collagen types I and III
Laminin
Fibronectin
MMP
TIMP
SPARC
CTGF
Selected altered genes:
CASP10, CAD,
TP53, ERCC4, BRCA2,
CDK2NA, APC2,
KRAS, MAP2K4,
BMPR2, SMAD4,
FAT, PCDH9,
GLI1, GLI3,
ILK, LAMA1,
MAP4K3, TNF,
MYC, TSC2,
ADAM11, ADAM19, PRSS23,
PLCB3, RP1
Stromal pathways:
Hedgehog
Nuclear factor
Cyclooxygenase-2
TGF-
Angiogenesis (VEGF and PDGF)
HGF-met
MMP
FGF
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1608
with angiogenesis inhibitors has failed in patients
with pancreatic cancer. A recent study in a mouse
model showed that targeting the stromal hedge-
hog pathway increases tumor vascularization,
resulting in increased delivery of chemothera-
peutic agents to pancreatic tumors and greater
efficacy.
29
In addition, a subgroup of cancer cells with
cancer stem-cell properties such as tumor initia-
tion have been identified within the tumor.
30,31
These cells, which compose just 1 to 5% of the
tumor, are capable of unlimited self-renewal,
and through asymmetric division, they give rise
to more-differentiated cells (Fig. 1). Pancreatic-
cancer stem cells are resistant to chemotherapy
and radiation therapy, which may explain why
these treatments do not cure the disease and
why there is much interest in targeting these
specific cells.
31,32
Clinical Presentation,
Diagnosis, and Staging
The presenting symptoms of pancreatic cancer
depend on the location of the tumor within the
gland, as well as on the stage of the disease.
The majority of tumors develop in the head of the
pancreas and cause obstructive cholestasis (Fig.
2A). Vague abdominal discomfort and nausea are
also common. More rarely, a pancreatic tumor
may also cause duodenal obstruction or gastroin-
testinal bleeding. Pancreatic cancer often causes
dull, deep upper abdominal pain that broadly lo-
calizes to the tumor area.
7 col
D E
A
C B
AUTHOR:
FIGURE:
RETAKE:
SIZE
4-C H/T Line Combo
Revised
AUTHOR, PLEASE NOTE:
Figure has been redrawn and type has been reset.
Please check carefully.
1st
2nd
3rd
Hidalgo
2 of 2
ARTIST:
TYPE:
ts
4-29-10 JOB: 36217 ISSUE:
ME: Authors combined Panel D (with arrows and type) is scaled vertically from unmarked
orginals. Currently, scaling is proportional to unmarked version.
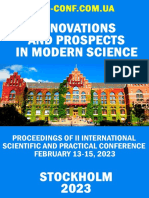
Figure 2. Pathological, Radiologic, and Histologic Features of Pancreatic Cancer.
Panel A shows a macroscopical view of a resected tumor affecting the head of the pancreas. Panel B shows a contrast- enhanced com-
puted tomographic scan from a patient with a T3 pancreatic mass. The tumor invades the splenic superior mesenteric veinportal vein
axis. Panel C shows endoscopic retrograde cholangiopancreatographic imaging of a plastic stent through the ampulla of Vater in a pa-
tient with a tumor in the head of the pancreas. Panel D (hematoxylin and eosin) shows microscopical adenocarcinoma of the pancreas
with abundant tumor stroma (black arrows). Smaller images show the tumor stroma at low, medium, and high magnification. Panel E
shows a peripancreatic lymph node involved with metastatic adenocarcinoma (hematoxylin and eosin, high magnification). (Courtesy
of Emilio de Vicente, M.D., and Elena Garcia, M.D.)
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1609
Obstruction of the pancreatic duct may lead to
pancreatitis. Patients with pancreatic cancer often
have dysglycemia. Indeed, pancreatic cancer should
be considered in the differential diagnoses of acute
pancreatitis and newly diagnosed diabetes.
At presentation, most patients also have sys-
temic manifestations of the disease such as asthe-
nia, anorexia, and weight loss. Other, less com-
mon manifestations include deep and superficial
venous thrombosis, panniculitis, liver-function
abnormalities, gastric-outlet obstruction, increased
abdominal girth, and depression.
Physical examination may reveal jaundice,
temporal wasting, peripheral lymphadenopathy,
hepatomegaly, and ascites. Results of routine
blood tests are generally nonspecific and may
include mild abnormalities in liver-function tests,
hyperglycemia, and anemia.
2,21
Evaluation of a patient in whom pancreatic
cancer is suspected should focus on diagnosis
and staging of the disease, assessment of resec-
tability, and palliation of symptoms. Multiphase,
multidetector helical computed tomography (CT)
with intravenous administration of contrast ma-
terial is the imaging procedure of choice for the
initial evaluation.
33
This technique allows visu-
alization of the primary tumor in relation to the
superior mesenteric artery, celiac axis, superior
mesenteric vein, and portal vein and also in
relation to distant organs (Fig. 2B). In general,
contrast-enhanced CT is sufficient to confirm a
suspected pancreatic mass and to frame an initial
management plan. Overall, contrast-enhanced CT
predicts surgical resectability with 80 to 90%
accuracy.
34
Positron-emission tomography can be
useful if the CT findings are equivocal.
Some patients require additional diagnostic
studies. Endoscopic ultrasonography is useful in
patients in whom pancreatic cancer is suspected
although there is no visible mass identifiable on
CT. It is the preferred method of obtaining tis-
sue for diagnostic purposes. Although a tissue
diagnosis is not needed in patients who are
scheduled for surgery, it is required before the
initiation of treatment with chemotherapy or
radiation therapy. Endoscopic retrograde cholan-
giopancreatography (ERCP) shows the pancreatic
and bile-duct anatomy and can be used to guide
ductal brushing and lavage, which provides tis-
sue for diagnosis. The ERCP technique is espe-
cially useful in patients with jaundice in whom
an endoscopic stent is required to relieve obstruc-
tion (Fig. 2C).
35
In patients who have large tu-
mors, especially in the body and tail of the pan-
creas, as well as other indications of advanced
disease such as weight loss, an elevated level of
carbohydrate antigen 19-9 (CA 19-9), ascites, or
equivocal CT findings, a staging laparoscopy can
accurately determine metastatic and vascular
involvement.
36
There are many potential serum biomarkers
for diagnosis, stratification of a prognosis, and
monitoring of therapy.
37
CA 19-9 is the only bio-
marker with demonstrated clinical usefulness and
is useful for therapeutic monitoring and early
detection of recurrent disease after treatment in
patients with known pancreatic cancer.
37-41
How-
ever, CA 19-9 has important limitations. It is not
a specific biomarker for pancreatic cancer; the
level of CA 19-9 may be elevated in other condi-
tions such as cholestasis. In addition, patients
who are negative for Lewis antigen a or b (ap-
proximately 10% of patients with pancreatic can-
cer) are unable to synthesize CA 19-9 and have
undetectable levels, even in advanced stages of
the disease. Although measurement of serum
CA 19-9 levels is useful in patients with known
pancreatic cancer, the use of this biomarker as a
screening tool has had disappointing results.
Universal primary screening for pancreatic
cancer is currently not recommended, given the
tools available and their performance.
42
Single-
institution studies focusing on surveillance of
patients at high risk, such as those with a strong
family history or cancer-predisposition syndromes,
have used serial endoscopic ultrasonography and
CT. Pancreatic lesions associated with benign
intrapancreatic mucinous neoplasia or pancreatic
intraepithelial neoplasia have been detected in
approximately 10% of these high-risk patients.
However, the cost-effectiveness of this approach
is unclear, and its use is investigational.
43
Staging of Pancreatic Cancer
Pancreatic cancer is staged according to the most
recent edition of the American Joint Committee
on Cancer tumornodemetastasis classification,
which is based on assessment of resectability by
means of helical CT.
44
T1, T2, and T3 tumors are
potentially resectable, whereas T4 tumors, which
involve the superior mesenteric artery or celiac
axis, are unresectable (Table 1). Tumors involv-
ing the superior mesenteric veins, portal veins, or
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1610
splenic veins are classified as T3, since these
veins can be resected and reconstructed, provid-
ed that they are patent.
Management of Early Disease
Patients with pancreatic cancer are best cared for
by multidisciplinary teams that include surgeons,
medical and radiation oncologists, radiologists,
gastroenterologists, nutritionists, and pain spe-
cialists, among others.
46,47
For patients with resec-
table disease, surgery remains the treatment of
choice.
48
Depending on the location of the tumor,
the operative procedures may involve cephalic
pancreatoduodenectomy (the Whipple procedure),
distal pancreatectomy, or total pancreatectomy.
A minimum of 12 to 15 lymph nodes should be
resected, and every attempt should be made to
obtain a tumor-free margin. Data from several
randomized clinical trials indicate that a more
extensive resection does not improve survival but
increases postoperative morbidity. Recent studies
show that the results of vein resection and vascu-
lar reconstruction in patients with limited in-
volvement of the superior mesenteric vein and
portal vein are similar to the results in patients
without vein involvement.
49
Poor prognostic fac-
tors include lymph-node metastases, a high tumor
grade, a large tumor, high levels of CA 19-9, per-
sistently elevated postoperative levels of CA 19-9,
and positive margins of resection.
38,40,50,51
Up to 70% of patients with pancreatic cancer
present with biliary obstruction, which can be
relieved by percutaneous or endoscopic stent
placement. Decompression is appropriate for pa-
tients in whom surgery is delayed, such as pa-
tients who are treated with neoadjuvant therapy
before resection or who are referred to other
centers for treatment.
52
Patients with symptoms
of cholangitis require decompression as well as
antibiotic treatment before surgery.
Even if the tumor is fully resected, the out-
come in patients with early pancreatic cancer is
disappointing. The results of three large ran-
domized clinical trials, summarized in Table 2 in
the Supplementary Appendix, have established
the role of postoperative treatment in patients
with resected pancreatic cancer.
53-55
The results
of the European Study Group for Pancreatic Can-
cer Trial 1 and Charit Onkologie 1 trial show that
postoperative administration of chemotherapy
with either fluorouracil and leucovorin or gem-
citabine, a nucleotide analogue commonly used
to treat advanced pancreatic cancer, improves
progression-free and overall survival. In addi-
tion, the Radiation Therapy Oncology Group
trial 97-04 showed that the combination of gem-
citabine with fluorouracil administered as a
continuous infusion and radiation therapy re-
sulted in a trend toward increased overall survival,
although the increase was not significant, among
patients with tumors in the head of the pancreas.
These results are similar to those of large single-
institution series that incorporated radiation
therapy.
56
Notwithstanding differences in patient popu-
lations and therapies, the outcome in patients
treated in these trials was similar, with a median
survival of 20 to 22 months. Large tumor size,
high differentiation grade, and involvement of the
lymph nodes are risk factors for recurrent disease.
The effect of positive resection margins, however,
Table 1. Staging of Pancreatic Cancer.*
Stage
Tumor
Grade
Nodal
Status
Distant
Metastases
Median
Survival Characteristics
mo
IA T1 N0 M0 24.1 Tumor limited to the pancreas, 2 cm in longest dimension
IB T2 N0 M0 20.6 Tumor limited to the pancreas, >2 cm in longest dimension
IIA T3 N0 M0 15.4 Tumor extends beyond the pancreas but does not involve the celiac
axis or superior mesenteric artery
IIB T1, T2, or T3 N1 M0 12.7 Regional lymph-node metastasis
III T4 N0 or N1 M0 10.6 Tumor involves the celiac axis or the superior mesenteric artery
(unresectable disease)
IV T1, T2, T3, or T4 N0 or N1 M1 4.5 Distant metastasis
* N denotes regional lymph nodes, M distant metastases, and T primary tumor.
Data are from Bilimoria et al.
45
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1611
is more controversial.
57
Thus, gemcita bine alone
or gemcitabine in combination with fluorouracil-
based chemoradiation can be considered the stan-
dard of care in this setting. The unequivocal dem-
onstration that postoperative treatment improves
the outcome in these patients is one of the most
important advances that has been made in the
management of pancreatic cancer.
An emerging strategy in patients with resect-
able pancreatic cancer is the use of preoperative
(neoadjuvant) treatment. Nonrandomized, phase
2 studies suggest that this approach is at least as
effective as postoperative treatment and may de-
crease the rate of local failures and positive resec-
tion margins after surgery.
58
These findings are
particularly relevant for patients who have so-
called borderline-resectable tumors with limited
vascular involvement; in these patients, preopera-
tive treatment may result in tumor-free resection
margins.
59
Management of Locally
Advanced and Systemically
Advanced Disease
Approximately 30% of patients with pancreatic
cancer receive a diagnosis of advanced loco-
regional disease, and an additional 30% of pa-
tients will have local recurrence of tumors after
treatment for early disease. The treatment of pa-
tients with advanced locoregional disease is palli-
ative; with current treatments, the median over-
all survival ranges only from 9 to 10 months.
Management options range from systemic chemo-
therapy alone to combined forms of treatment
with chemoradiation therapy and chemotherapy.
A series of randomized trials conducted over the
past two decades established that chemoradia-
tion therapy was superior to radiation therapy
alone in these patients.
60,61
The results of more
recent studies, summarized in Table 3 in the
Supplementary Appendix, suggest that chemo-
therapy is indeed the critical component in the
treatment approach and that combined treatment
with chemotherapy and chemoradiation therapy
is an effective, though more toxic, approach. How-
ever, randomized clinical trials of such combined
treatments have had low enrollment, precluding
a firm conclusion.
60,62,63
The majority of patients with pancreatic can-
cer either present with metastatic disease or
metastatic disease develops in them, mainly in
the liver and peritoneal cavity. The treatment of
patients with advanced disease remains palliative,
although these patients should be offered the
opportunity to participate in clinical trials evalu-
ating new treatments when available. A meta-
analysis of published findings from clinical trials
showed an improvement in survival among pa-
tients who received chemotherapy; these findings
suggest that active treatment is beneficial.
61
For
more than a decade, gemcitabine has been the
treatment of choice on the basis of the results of
the randomized trial of gemcitabine versus fluo-
rouracil, summarized in Table 3 in the Supplemen-
tary Appendix.
64
Multiple new agents with diverse
mechanisms of action in combination with gem-
citabine have been tested in randomized clinical
trials, with no improvement in outcome.
2,65,66
The only agent that, in combination with
gemcitabine, has shown a small, but statistically
significant improvement in survival among pa-
tients with advanced pancreatic cancer is erloti-
nib, a small-molecule inhibitor of the epidermal
growth factor receptor (EGFR) (Table 3 in the
Supplementary Appendix).
67
As shown in other
studies of agents targeting the EGFR, patients in
whom drug-induced rashes developed had a better
outcome. However, the high frequency of KRAS2
mutations in pancreatic cancer probably limits
the benefits of an EGFR inhibitor; this limita-
tion is similar to that observed in other cancers
such as colon cancer. As compared with erlotinib
alone, the combination of gemcitabine and erlo-
tinib has more toxicity, particularly gastrointes-
tinal symptoms. Together with the rather mod-
est improvement in survival, the toxicity of this
combination has limited its wide acceptance as
the standard of care. A recent meta-analysis of
randomized trials showed that patients with
minimal disease-related symptoms and otherwise
good health may benefit from combination che-
motherapy with gemcitabine and either a plati-
num agent or a fluoropyrimidine.
66,68
Thus, at the
present time, the accepted treatment approach
for patients with advanced disease is either gem-
citabine given alone or gemcitabine combined
with a platinum agent, erlotinib, or a fluoropy-
ri midine.
Once the disease progresses, there is no ac-
cepted standard of care; most patients at that
point are too sick to receive any other treatment.
In a highly selected group of patients with mini-
mally symptomatic disease, second-line chemo-
therapy has modest efficacy, and it can be offered
to patients with good functional reserve (i.e., pa-
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1612
T
a
b
l
e
2
.
C
o
m
m
o
n
l
y
U
s
e
d
T
r
e
a
t
m
e
n
t
R
e
g
i
m
e
n
s
i
n
P
a
n
c
r
e
a
t
i
c
C
a
n
c
e
r
.
*
D
r
u
g
M
e
c
h
a
n
i
s
m
o
f
A
c
t
i
o
n
D
o
s
e
S
e
r
i
o
u
s
T
o
x
i
c
E
f
f
e
c
t
s
O
c
c
u
r
r
i
n
g
i
n
>
1
0
%
o
f
P
a
t
i
e
n
t
s
R
e
f
e
r
e
n
c
e
F
i
r
s
t
-
l
i
n
e
t
h
e
r
a
p
y
G
e
m
c
i
t
a
b
i
n
e
(
2
'
,
2
'
-
d
F
d
C
)
N
u
c
l
e
o
s
i
d
e
a
n
a
l
o
g
u
e
m
e
t
a
b
o
l
i
z
e
d
t
o
t
r
i
p
h
o
s
p
h
a
t
e
m
o
i
e
t
y
(
d
F
d
C
t
r
i
p
h
o
s
-
p
h
a
t
e
)
b
y
d
e
o
x
y
c
y
t
i
d
i
n
e
k
i
n
a
s
e
i
s
i
n
c
o
r
p
o
r
a
t
e
d
i
n
t
o
t
h
e
n
a
s
c
e
n
t
D
N
A
a
n
d
b
l
o
c
k
s
D
N
A
r
e
p
l
i
c
a
t
i
o
n
1
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
3
0
-
m
i
n
I
V
i
n
f
u
-
s
i
o
n
e
i
t
h
e
r
w
e
e
k
l
y
f
o
r
7
w
k
,
f
o
l
l
o
w
e
d
b
y
1
w
k
r
e
s
t
,
t
h
e
n
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
;
o
r
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
N
e
u
t
r
o
p
e
n
i
a
(
2
6
%
)
,
e
l
e
v
a
t
e
d
a
l
k
a
l
i
n
e
p
h
o
s
p
h
a
t
a
s
e
l
e
v
e
l
(
1
6
%
)
,
t
h
r
o
m
b
o
-
c
y
t
o
p
e
n
i
a
(
1
0
%
)
,
e
l
e
v
a
t
e
d
A
S
T
l
e
v
e
l
(
1
0
%
)
B
u
r
r
i
s
e
t
a
l
.
6
4
F
i
x
e
d
-
d
o
s
e
i
n
f
u
s
i
o
n
o
f
g
e
m
c
i
t
a
b
i
n
e
P
r
o
l
o
n
g
e
d
e
x
p
o
s
u
r
e
t
o
g
e
m
c
i
t
a
b
i
n
e
i
n
c
r
e
a
s
e
s
a
c
c
u
m
u
l
a
t
i
o
n
o
f
d
F
d
C
t
r
i
p
h
o
s
p
h
a
t
e
1
5
0
0
m
g
/
m
2
g
i
v
e
n
a
s
1
0
m
g
/
m
2
/
m
i
n
I
V
i
n
f
u
s
i
o
n
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
N
e
u
t
r
o
p
e
n
i
a
(
4
9
%
)
,
t
h
r
o
m
b
o
c
y
t
o
p
e
n
i
a
(
3
7
%
)
,
a
n
e
m
i
a
(
2
3
%
)
,
n
a
u
s
e
a
a
n
d
v
o
m
i
t
i
n
g
(
2
1
%
)
T
e
m
p
e
r
o
e
t
a
l
.
7
1
G
e
m
c
i
t
a
b
i
n
e
p
l
u
s
o
x
a
l
i
p
l
a
t
i
n
O
x
a
l
i
p
l
a
t
i
n
i
s
a
d
i
a
m
i
n
o
c
y
c
l
o
h
e
x
a
n
o
p
l
a
t
i
n
u
m
a
n
a
l
o
g
u
e
t
h
a
t
b
i
n
d
s
a
n
d
a
l
k
y
l
a
t
e
s
D
N
A
G
e
m
c
i
t
a
b
i
n
e
:
1
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
1
0
m
g
/
m
2
/
m
i
n
I
V
i
n
f
u
s
i
o
n
o
n
d
a
y
1
e
v
e
r
y
o
t
h
e
r
w
k
;
p
l
u
s
o
x
a
l
i
p
l
a
t
i
n
:
1
0
0
m
g
/
m
2
g
i
v
e
n
a
s
1
2
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
o
n
d
a
y
2
,
e
v
e
r
y
o
t
h
e
r
w
k
N
e
u
t
r
o
p
e
n
i
a
(
2
0
%
)
,
p
e
r
i
p
h
e
r
a
l
s
e
n
s
o
r
y
n
e
u
r
o
p
a
t
h
y
(
1
9
%
)
,
t
h
r
o
m
b
o
c
y
t
o
p
e
-
n
i
a
(
1
4
%
)
,
n
a
u
s
e
a
(
1
0
%
)
L
o
u
v
e
t
e
t
a
l
.
7
2
G
e
m
c
i
t
a
b
i
n
e
p
l
u
s
c
i
s
p
l
a
t
i
n
C
i
s
p
l
a
t
i
n
i
s
a
D
N
A
-
b
i
n
d
i
n
g
a
l
k
y
l
a
t
i
n
g
a
g
e
n
t
G
e
m
c
i
t
a
b
i
n
e
:
1
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
3
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
e
v
e
r
y
o
t
h
e
r
w
k
;
c
i
s
-
p
l
a
t
i
n
:
5
0
m
g
/
m
2
g
i
v
e
n
a
s
I
V
i
n
f
u
-
s
i
o
n
e
v
e
r
y
o
t
h
e
r
w
k
N
a
u
s
e
a
a
n
d
v
o
m
i
t
i
n
g
(
2
2
%
)
,
a
n
e
m
i
a
(
1
3
%
)
,
p
a
i
n
(
1
2
%
)
,
l
e
u
k
o
p
e
n
i
a
(
1
0
%
)
H
e
i
n
e
m
a
n
n
e
t
a
l
.
7
3
G
e
m
c
i
t
a
b
i
n
e
p
l
u
s
c
a
p
e
c
i
t
a
b
i
n
e
C
a
p
e
c
i
t
a
b
i
n
e
i
s
c
o
n
v
e
r
t
e
d
i
n
t
h
e
t
u
m
o
r
t
o
f
l
u
o
r
o
u
r
a
c
i
l
a
n
d
i
n
h
i
b
i
t
s
t
h
y
m
i
d
i
-
l
a
t
e
s
y
n
t
h
e
t
a
s
e
G
e
m
c
i
t
a
b
i
n
e
:
1
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
3
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
;
p
l
u
s
c
a
p
e
c
i
t
a
b
i
n
e
:
1
3
0
0
m
g
/
m
2
d
a
i
l
y
,
o
r
a
l
l
y
f
o
r
1
4
d
a
y
s
e
v
e
r
y
3
4
w
k
,
d
i
v
i
d
e
d
i
n
t
w
o
d
a
i
l
y
d
o
s
e
s
N
e
u
t
r
o
p
e
n
i
a
(
2
3
%
)
B
e
r
n
h
a
r
d
e
t
a
l
.
7
4
G
e
m
c
i
t
a
b
i
n
e
p
l
u
s
e
r
l
o
t
i
n
i
b
E
r
l
o
t
i
n
i
b
i
s
a
s
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
o
f
t
h
e
e
p
i
d
e
r
m
a
l
g
r
o
w
t
h
f
a
c
t
o
r
r
e
c
e
p
t
o
r
G
e
m
c
i
t
a
b
i
n
e
:
1
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
3
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
,
e
i
t
h
e
r
w
e
e
k
l
y
f
o
r
7
w
k
f
o
l
l
o
w
e
d
b
y
1
w
k
r
e
s
t
,
t
h
e
n
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
,
o
r
w
e
e
k
l
y
f
o
r
3
o
f
e
v
e
r
y
4
w
k
;
p
l
u
s
e
r
l
o
t
i
n
i
b
:
1
0
0
m
g
/
d
a
y
o
r
a
l
l
y
d
a
i
l
y
N
e
u
t
r
o
p
e
n
i
a
(
2
4
%
)
,
i
n
f
e
c
t
i
o
n
(
1
7
%
)
,
f
a
t
i
g
u
e
(
1
5
%
)
,
e
l
e
v
a
t
e
d
A
S
T
l
e
v
e
l
(
1
1
%
)
,
t
h
r
o
m
b
o
c
y
t
o
p
e
n
i
a
(
1
0
%
)
M
o
o
r
e
e
t
a
l
.
6
7
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1613
S
e
c
o
n
d
-
l
i
n
e
t
h
e
r
a
p
y
M
o
d
i
f
i
e
d
F
O
L
F
O
X
(
c
o
m
b
i
n
a
t
i
o
n
r
e
g
i
m
e
n
i
n
c
l
u
d
i
n
g
o
x
a
l
i
p
l
a
t
i
n
,
f
l
u
o
r
o
u
r
a
c
i
l
,
a
n
d
l
e
u
c
o
v
o
r
i
n
)
F
l
u
o
r
o
u
r
a
c
i
l
i
s
a
n
i
n
h
i
b
i
t
o
r
o
f
t
h
y
m
i
d
i
l
a
t
e
s
y
n
t
h
e
t
a
s
e
,
a
n
d
l
e
u
c
o
v
o
r
i
n
p
o
t
e
n
t
i
-
a
t
e
s
t
h
e
i
n
h
i
b
i
t
i
o
n
o
f
t
h
y
m
i
d
i
l
a
t
e
s
y
n
t
h
e
t
a
s
e
b
y
f
l
u
o
r
o
u
r
a
c
i
l
O
x
a
l
i
p
l
a
t
i
n
:
8
5
m
g
/
m
2
g
i
v
e
n
a
s
1
2
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
e
v
e
r
y
o
t
h
e
r
w
k
;
l
e
u
c
o
v
o
r
-
i
n
:
4
0
0
m
g
/
m
2
o
n
d
a
y
1
,
e
v
e
r
y
o
t
h
e
r
w
k
;
a
n
d
f
l
u
o
r
o
u
r
a
c
i
l
:
2
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
4
6
-
h
r
i
n
f
u
s
i
o
n
e
v
e
r
y
o
t
h
e
r
w
k
N
e
u
t
r
o
p
e
n
i
a
(
2
0
%
)
,
a
s
t
h
e
n
i
a
(
1
3
%
)
,
v
o
m
i
t
i
n
g
(
1
0
%
)
L
i
a
n
d
S
a
i
f
7
5
M
o
d
i
f
i
e
d
F
O
L
F
I
R
I
.
3
(
c
o
m
b
i
n
a
t
i
o
n
r
e
g
i
m
e
n
o
f
i
r
i
n
o
t
e
c
a
n
w
i
t
h
f
l
u
o
r
o
u
r
a
c
i
l
a
n
d
l
e
u
c
o
v
o
r
i
n
)
F
l
u
o
r
o
u
r
a
c
i
l
i
s
a
n
i
n
h
i
b
i
t
o
r
o
f
t
h
y
m
i
d
i
l
a
t
e
s
y
n
t
h
e
t
a
s
e
,
a
n
d
i
r
i
n
o
t
e
c
a
n
i
s
a
t
o
p
o
-
i
s
o
m
e
r
a
s
e
I
i
n
h
i
b
i
t
o
r
;
l
e
u
c
o
v
o
r
i
n
p
o
-
t
e
n
t
i
a
t
e
s
t
h
e
i
n
h
i
b
i
t
i
o
n
o
f
t
h
y
m
i
d
i
l
a
t
e
s
y
n
t
h
e
t
a
s
e
b
y
f
l
u
o
r
o
u
r
a
c
i
l
I
r
i
n
o
t
e
c
a
n
:
7
0
m
g
/
m
2
g
i
v
e
n
a
s
6
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
o
n
d
a
y
1
;
l
e
u
c
o
v
o
r
i
n
:
4
0
0
m
g
/
m
2
g
i
v
e
n
a
s
g
i
v
e
n
a
s
1
2
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
o
n
d
a
y
1
;
a
n
d
f
l
u
o
r
o
u
r
a
c
i
l
:
2
0
0
0
m
g
/
m
2
g
i
v
e
n
a
s
4
6
-
h
r
I
V
i
n
f
u
-
s
i
o
n
o
n
d
a
y
1
;
a
n
d
i
r
i
n
o
t
e
c
a
n
:
7
0
m
g
/
m
g
2
g
i
v
e
n
a
s
6
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
a
t
t
h
e
e
n
d
o
f
t
h
e
i
n
f
u
s
i
o
n
o
f
f
l
u
o
r
o
u
r
a
-
c
i
l
,
e
v
e
r
y
2
w
k
N
e
u
t
r
o
p
e
n
i
a
(
2
2
%
)
,
v
o
m
i
t
i
n
g
(
1
0
%
)
L
i
a
n
d
S
a
i
f
7
5
O
x
a
l
i
p
l
a
t
i
n
p
l
u
s
c
a
p
e
c
i
t
a
b
i
n
e
O
x
a
l
i
p
l
a
t
i
n
i
s
a
d
i
a
m
i
n
o
c
y
c
l
o
h
e
x
a
n
o
p
l
a
t
i
n
u
m
a
n
a
l
o
g
u
e
t
h
a
t
b
i
n
d
s
a
n
d
a
l
-
k
y
l
a
t
e
s
D
N
A
;
c
a
p
e
c
i
t
a
b
i
n
e
i
s
c
o
n
v
e
r
t
-
e
d
i
n
t
h
e
t
u
m
o
r
t
o
f
l
u
o
r
o
u
r
a
c
i
l
a
n
d
i
n
h
i
b
i
t
s
t
h
y
m
i
d
i
l
a
t
e
s
y
n
t
h
e
t
a
s
e
O
x
a
l
i
p
l
a
t
i
n
:
1
3
0
m
g
/
m
2
g
i
v
e
n
a
s
1
2
0
-
m
i
n
I
V
i
n
f
u
s
i
o
n
e
v
e
r
y
3
w
k
;
a
n
d
c
a
p
e
c
i
t
a
b
i
n
e
:
2
0
0
0
m
g
/
m
2
d
a
i
l
y
,
o
r
a
l
l
y
f
o
r
1
4
d
a
y
s
e
v
e
r
y
3
4
w
k
,
d
i
v
i
d
e
d
i
n
t
w
o
d
a
i
l
y
d
o
s
e
s
O
x
a
l
i
p
l
a
t
i
n
:
f
a
t
i
g
u
e
(
1
3
%
)
,
d
i
a
r
r
h
e
a
(
5
%
)
,
v
o
m
i
t
i
n
g
(
3
%
)
;
c
a
p
e
c
i
t
a
b
i
n
e
:
h
a
n
d
f
o
o
t
s
y
n
d
r
o
m
e
(
3
%
)
,
a
b
d
o
m
i
-
n
a
l
p
a
i
n
(
3
%
)
X
i
o
n
g
e
t
a
l
.
6
9
C
a
p
e
c
i
t
a
b
i
n
e
p
l
u
s
e
r
l
o
t
i
n
i
b
C
a
p
e
c
i
t
a
b
i
n
e
i
s
c
o
n
v
e
r
t
e
d
i
n
t
h
e
t
u
m
o
r
t
o
f
l
u
o
r
o
u
r
a
c
i
l
a
n
d
i
n
h
i
b
i
t
s
t
h
y
m
i
d
i
-
l
a
t
e
s
y
n
t
h
e
t
a
s
e
;
e
r
l
o
t
i
n
i
b
i
s
a
s
m
a
l
l
-
m
o
l
e
c
u
l
a
r
i
n
h
i
b
i
t
o
r
o
f
t
h
e
e
p
i
d
e
r
m
a
l
g
r
o
w
t
h
f
a
c
t
o
r
r
e
c
e
p
t
o
r
C
a
p
e
c
i
t
a
b
i
n
e
:
2
0
0
0
m
g
/
m
2
d
a
i
l
y
,
o
r
a
l
l
y
f
o
r
1
4
d
a
y
s
e
v
e
r
y
3
4
w
k
,
d
i
v
i
d
e
d
i
n
t
w
o
d
a
i
l
y
d
o
s
e
s
;
a
n
d
e
r
l
o
t
i
n
i
b
:
1
5
0
m
g
o
r
a
l
l
y
d
a
i
l
y
C
a
p
e
c
i
t
a
b
i
n
e
:
d
i
a
r
r
h
e
a
(
1
7
%
)
,
r
a
s
h
(
1
3
%
)
,
h
a
n
d
f
o
o
t
s
y
n
d
r
o
m
e
(
1
3
%
)
,
m
u
c
o
s
i
-
t
i
s
(
1
0
%
)
;
e
r
l
o
t
i
n
i
b
:
f
a
t
i
g
u
e
(
3
%
)
,
e
l
e
-
v
a
t
e
d
b
i
l
i
r
u
b
i
n
l
e
v
e
l
(
3
%
)
,
e
l
e
v
a
t
e
d
a
l
k
a
l
i
n
e
p
h
o
s
p
h
a
t
a
s
e
l
e
v
e
l
(
3
%
)
K
u
l
k
e
e
t
a
l
.
7
0
*
A
S
T
d
e
n
o
t
e
s
a
s
p
a
r
t
a
t
e
a
m
i
n
o
t
r
a
n
s
f
e
r
a
s
e
;
d
F
d
C
d
i
f
l
u
o
r
o
d
e
o
x
y
c
y
t
i
d
i
n
e
;
F
O
L
F
I
R
I
.
3
r
e
g
i
m
e
n
o
f
f
l
u
o
r
o
u
r
a
c
i
l
,
l
e
u
c
o
v
o
r
i
n
,
a
n
d
i
r
i
n
o
t
e
c
a
n
;
F
O
L
F
O
X
r
e
g
i
m
e
n
o
f
f
o
l
i
n
i
c
a
c
i
d
,
f
l
u
o
r
o
u
r
a
c
i
l
,
a
n
d
o
x
a
l
i
p
l
a
t
i
n
;
a
n
d
I
V
i
n
t
r
a
v
e
n
o
u
s
.
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1614
T
a
b
l
e
3
.
S
e
l
e
c
t
e
d
S
t
r
a
t
e
g
i
c
T
a
r
g
e
t
s
i
n
P
a
n
c
r
e
a
t
i
c
C
a
n
c
e
r
.
*
T
a
r
g
e
t
A
g
e
n
t
D
r
u
g
C
l
a
s
s
M
e
c
h
a
n
i
s
m
o
f
A
c
t
i
o
n
T
r
i
a
l
P
h
a
s
e
R
e
f
e
r
e
n
c
e
S
P
A
R
C
N
a
n
o
p
a
r
t
i
c
l
e
a
l
b
u
m
i
n
-
b
o
u
n
d
p
a
c
l
i
t
a
x
e
l
C
y
t
o
t
o
x
i
c
a
g
e
n
t
S
P
A
R
C
,
e
x
p
r
e
s
s
e
d
i
n
c
a
n
c
e
r
c
e
l
l
s
a
n
d
s
t
r
o
m
a
i
n
t
h
e
p
a
n
c
r
e
a
s
,
b
i
n
d
s
n
a
n
o
p
a
r
t
i
c
l
e
a
l
b
u
m
i
n
-
b
o
u
n
d
p
a
c
l
i
t
a
x
e
l
,
i
n
c
r
e
a
s
i
n
g
l
o
c
a
l
d
r
u
g
d
e
l
i
v
e
r
y
3
L
i
a
n
d
S
a
i
f
7
5
I
G
F
-
I
R
M
K
0
6
4
6
,
A
M
G
4
7
9
,
R
1
5
0
7
M
o
n
o
c
l
o
n
a
l
a
n
t
i
b
o
d
y
I
n
h
i
b
i
t
s
l
i
g
a
n
d
b
i
n
d
i
n
g
a
c
t
i
v
a
t
i
o
n
o
f
t
h
e
I
G
F
-
I
R
a
n
d
c
e
l
l
p
r
o
l
i
f
e
r
a
t
i
o
n
3
H
e
w
i
s
h
e
t
a
l
.
7
8
D
e
a
t
h
r
e
c
e
p
t
o
r
A
M
G
6
5
5
,
C
S
1
0
0
8
M
o
n
o
c
l
o
n
a
l
a
n
t
i
b
o
d
y
A
g
o
n
i
s
t
a
n
t
i
b
o
d
i
e
s
t
o
m
e
m
b
r
a
n
e
d
e
a
t
h
r
e
c
e
p
t
o
r
s
i
n
d
u
c
e
a
p
o
p
t
o
s
i
s
2
L
i
a
n
d
S
a
i
f
,
7
5
D
e
r
o
s
i
e
r
e
t
a
l
.
7
9
M
u
c
i
n
-
1
9
0
Y
-
h
P
A
M
4
R
a
d
i
o
i
m
m
u
n
o
c
o
n
j
u
g
a
t
e
T
a
r
g
e
t
s
m
u
c
i
n
-
1
e
x
p
r
e
s
s
e
d
i
n
p
a
n
c
r
e
a
t
i
c
-
c
a
n
c
e
r
c
e
l
l
s
a
n
d
d
e
l
i
v
e
r
s
r
a
d
i
a
t
i
o
n
l
o
a
d
1
2
G
o
l
d
e
t
a
l
.
8
0
H
e
d
g
e
h
o
g
p
a
t
h
w
a
y
G
D
C
-
0
4
4
9
,
I
P
I
-
9
2
6
S
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
I
n
h
i
b
i
t
s
s
m
o
o
t
h
e
n
e
d
r
e
c
e
p
t
o
r
,
r
e
s
u
l
t
i
n
g
i
n
i
n
h
i
b
i
t
i
o
n
o
f
c
e
l
l
p
r
o
l
i
f
e
r
a
t
i
o
n
;
t
a
r
g
e
t
s
c
a
n
c
e
r
s
t
r
o
m
a
a
n
d
c
a
n
c
e
r
s
t
e
m
c
e
l
l
s
i
n
t
h
e
p
a
n
c
r
e
a
s
1
O
l
i
v
e
e
t
a
l
.
,
2
9
J
i
m
e
n
o
e
t
a
l
.
3
2
c
-
k
i
t
,
P
D
G
F
R
,
F
G
F
R
M
a
s
i
t
i
n
i
b
S
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
M
u
l
t
i
k
i
n
a
s
e
i
n
h
i
b
i
t
o
r
t
a
r
g
e
t
s
c
-
k
i
t
,
P
D
G
F
R
,
a
n
d
F
G
F
R
3
a
n
d
a
f
f
e
c
t
s
t
h
e
F
A
K
p
a
t
h
w
a
y
;
m
a
s
i
t
i
n
i
b
w
a
s
s
h
o
w
n
t
o
e
n
h
a
n
c
e
t
h
e
a
n
t
i
p
r
o
l
i
f
e
r
a
t
i
v
e
e
f
f
e
c
t
s
o
f
g
e
m
c
i
t
a
b
i
n
e
i
n
p
r
e
c
l
i
n
i
c
a
l
s
t
u
d
i
e
s
3
L
i
a
n
d
S
a
i
f
7
5
M
E
K
A
Z
D
6
2
4
4
S
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
T
a
r
g
e
t
s
a
n
d
i
n
h
i
b
i
t
s
M
E
K
,
d
e
c
r
e
a
s
i
n
g
c
e
l
l
p
r
o
l
i
f
e
r
a
t
i
o
n
2
C
h
u
n
g
e
t
a
l
.
8
1
S
r
c
A
Z
D
0
5
3
0
,
d
a
s
a
t
i
n
i
b
S
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
T
a
r
g
e
t
s
a
n
d
i
n
h
i
b
i
t
s
S
r
c
k
i
n
a
s
e
,
r
e
s
u
l
t
i
n
g
i
n
i
n
h
i
b
i
t
i
o
n
o
f
c
e
l
l
p
r
o
l
i
f
e
r
a
t
i
o
n
a
n
d
i
n
v
a
s
i
o
n
2
R
a
j
e
s
h
k
u
m
a
r
e
t
a
l
.
7
7
R
A
S
S
a
r
i
l
a
s
i
b
S
m
a
l
l
-
m
o
l
e
c
u
l
e
i
n
h
i
b
i
t
o
r
D
i
s
l
o
d
g
e
s
a
l
l
f
o
r
m
s
o
f
R
A
S
f
r
o
m
t
h
e
p
l
a
s
m
a
m
e
m
b
r
a
n
e
,
i
n
h
i
b
i
t
i
n
g
R
A
S
s
i
g
n
a
l
i
n
g
2
H
a
k
l
a
i
e
t
a
l
.
8
2
P
S
C
A
A
G
S
-
1
C
4
D
4
M
o
n
o
c
l
o
n
a
l
a
n
t
i
b
o
d
y
B
i
n
d
s
m
e
m
b
r
a
n
e
P
S
C
A
;
s
p
e
c
i
f
i
c
m
e
c
h
a
n
i
s
m
s
o
f
c
e
l
l
k
i
l
l
i
n
g
u
n
d
e
t
e
r
m
i
n
e
d
2
W
e
n
t
e
e
t
a
l
.
8
3
M
e
s
o
t
h
e
l
i
n
M
O
R
A
b
-
0
0
9
M
o
n
o
c
l
o
n
a
l
a
n
t
i
b
o
d
y
B
i
n
d
s
m
e
m
b
r
a
n
e
m
e
s
o
t
h
e
l
i
n
;
s
p
e
c
i
f
i
c
m
e
c
h
a
n
i
s
m
s
o
f
c
e
l
l
k
i
l
l
i
n
g
u
n
d
e
t
e
r
m
i
n
e
d
2
H
a
s
s
a
n
e
t
a
l
.
8
4
T
N
F
-
T
N
F
e
r
a
d
e
G
e
n
e
t
h
e
r
a
p
y
A
d
e
n
o
v
i
r
a
l
g
e
n
e
t
h
e
r
a
p
y
i
n
c
r
e
a
s
e
s
i
n
t
r
a
t
u
m
o
r
a
l
c
o
n
c
e
n
t
r
a
t
i
o
n
o
f
T
N
F
-
3
M
u
r
u
g
e
s
a
n
e
t
a
l
.
8
5
*
T
h
e
a
b
b
r
e
v
i
a
t
i
o
n
c
-
k
i
t
d
e
n
o
t
e
s
s
t
e
m
-
c
e
l
l
f
a
c
t
o
r
r
e
c
e
p
t
o
r
;
F
A
K
f
o
c
a
l
a
d
h
e
s
i
o
n
k
i
n
a
s
e
;
F
G
F
R
f
i
b
r
o
b
l
a
s
t
g
r
o
w
t
h
f
a
c
t
o
r
r
e
c
e
p
t
o
r
;
I
G
F
-
I
R
t
y
p
e
I
i
n
s
u
l
i
n
-
l
i
k
e
g
r
o
w
t
h
f
a
c
t
o
r
r
e
c
e
p
t
o
r
;
M
E
K
m
i
t
o
g
e
n
-
a
c
t
i
v
a
t
e
d
p
r
o
t
e
i
n
k
i
n
a
s
e
e
x
t
r
a
c
e
l
l
u
l
a
r
-
s
i
g
n
a
l
r
e
g
u
l
a
t
e
d
k
i
n
a
s
e
,
P
D
G
F
R
p
l
a
t
e
l
e
t
-
d
e
r
i
v
e
d
g
r
o
w
t
h
f
a
c
t
o
r
;
P
S
C
A
p
r
o
s
t
a
t
e
s
t
e
m
-
c
e
l
l
a
n
t
i
g
e
n
;
S
P
A
R
C
s
e
c
r
e
t
e
d
p
r
o
t
e
i
n
,
a
c
i
d
i
c
,
c
y
s
t
e
i
n
e
-
r
i
c
h
;
a
n
d
T
N
F
-
t
u
m
o
r
n
e
c
r
o
s
i
s
f
a
c
t
o
r
.
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1615
tients who are ambulatory and minimally symp-
tomatic).
69,70
Table 2 lists commonly used first-line
and second-line therapeutic regimens.
Future Directions
There is much room for improvement in all as-
pects of treatment for pancreatic cancer. Screen-
ing of high-risk persons by means of either in-
novative imaging methods or measurements of
serum biomarkers for early diagnosis is criti-
cal.
42,43,76
A better understanding of the biology
of pancreatic cancer is opening new avenues for
treatment, and an increasing number of new tar-
geted agents are in clinical development (Table 3).
These agents include small-molecule inhibitors of
oncogenes and signaling pathways such as RAS,
Src, and MEK, monoclonal antibodies targeting
cell-membrane proteins such as mesothelin and
the so-called death receptors, and new nanotech-
nology and adenoviral agents. The recognition
that the tumor microenvironment and cancer
stem cells are critical components of pancreatic
cancer has led to the development of agents, such
as the hedgehog inhibitors, that target these
components.
23,29,31,32
The availability of preclini-
cal models that recapitulate the complexity of
this disease will probably help in establishing
priorities and strategies for the development of
new treatments.
77,86
The complexity of the genome
of pancreatic cancer indicates that it is a hetero-
geneous cancer and that methods to individual-
ize therapy will be required.
11,87
Dr. Hidalgo reports receiving grant support from Roche and
Daichi; being the principal investigator and receiving grant sup-
port for clinical studies of nanoparticle albumin-bound paclitaxel
from American Biosciences, of erlotinib from Roche, of AGS-
1C4D4 from Agensys, and of MORAb-009 from Eisai; and receiv-
ing consulting fees from American Biosciences, OSIGenentech,
Merck, and Agensys. No other potential conflict of interest rele-
vant to this article was reported.
I thank Wells Messersmith and Anirban Maitra for critical
comments on an earlier version of the manuscript and Sofia
Perea for editorial assistance.
References
Jemal A, Siegel R, Ward E, et al. Can- 1.
cer statistics, 2008. CA Cancer J Clin
2008;58:71-96.
Li D, Xie K, Wolff R, Abbruzzese JL. 2.
Pancreatic cancer. Lancet 2004;363:1049-
57.
Hassan MM, Bondy ML, Wolff RA, et al. 3.
Risk factors for pancreatic cancer: case-
control study. Am J Gastroenterol 2007;
102:2696-707.
Batty GD, Kivimaki M, Morrison D, 4.
et al. Risk factors for pancreatic cancer
mortality: extended follow-up of the orig-
inal Whitehall Study. Cancer Epidemiol
Biomarkers Prev 2009;18:673-5.
Landi S. Genetic predisposition and 5.
environmental risk factors to pancreatic
cancer: a review of the literature. Mutat
Res 2009;681:299-307.
Lowenfels AB, Maisonneuve P. Epide- 6.
miology and risk factors for pancreatic
cancer. Best Pract Res Clin Gastroenterol
2006;20:197-209.
Genkinger JM, Spiegelman D, Ander- 7.
son KE, et al. Alcohol intake and pancre-
atic cancer risk: a pooled analysis of four-
teen cohort studies. Cancer Epidemiol
Biomarkers Prev 2009;18:765-76.
Wolpin BM, Chan AT, Hartge P, et al. 8.
ABO blood group and the risk of pancre-
atic cancer. J Natl Cancer Inst 2009;101:
424-31.
Shi C, Hruban RH, Klein AP. Familial 9.
pancreatic cancer. Arch Pathol Lab Med
2009;133:365-74.
Tersmette AC, Petersen GM, Offer- 10.
haus GJ, et al. Increased risk of incident
pancreatic cancer among first-degree rel-
atives of patients with familial pancreatic
cancer. Clin Cancer Res 2001;7:738-44.
Jones S, Zhang X, Parsons DW, et al. 11.
Core signaling pathways in human pan-
creatic cancers revealed by global genom-
ic analyses. Science 2008;321:1801-6.
Couch FJ, Johnson MR, Rabe KG, et al. 12.
The prevalence of BRCA2 mutations in
familial pancreatic cancer. Cancer Epide-
miol Biomarkers Prev 2007;16:342-6.
Jones S, Hruban RH, Kamiyama M, et 13.
al. Exomic sequencing identifies PALB2
as a pancreatic cancer susceptibility gene.
Science 2009;324:217.
Vogelstein B, Kinzler KW. Cancer 14.
genes and the pathways they control. Nat
Med 2004;10:789-99.
Hruban RH, Maitra A, Goggins M. 15.
Update on pancreatic intraepithelial neo-
plasia. Int J Clin Exp Pathol 2008;1:306-
16.
Feldmann G, Beaty R, Hruban RH, 16.
Maitra A. Molecular genetics of pancre-
atic intraepithelial neoplasia. J Hepatobil-
iary Pancreat Surg 2007;14:224-32.
Hingorani SR, Wang L, Multani AS, et 17.
al. Trp53R172H and KrasG12D cooperate
to promote chromosomal instability and
widely metastatic pancreatic ductal ade-
nocarcinoma in mice. Cancer Cell 2005;
7:469-83.
Guerra C, Schuhmacher AJ, Caamero 18.
M, et al. Chronic pancreatitis is essential
for induction of pancreatic ductal adeno-
carcinoma by K-Ras oncogenes in adult
mice. Cancer Cell 2007;11:291-302.
Bardeesy N, Aguirre AJ, Chu GC, et al. 19.
Both p16(Ink4a) and the p19(Arf )-p53
pathway constrain progression of pancre-
atic adenocarcinoma in the mouse. Proc
Natl Acad Sci U S A 2006;103:5947-52.
Takaori K. Current understanding of 20.
precursors to pancreatic cancer. J Hepato-
biliary Pancreat Surg 2007;14:217-23.
Maitra A, Hruban RH. Pancreatic can- 21.
cer. Annu Rev Pathol 2008;3:157-88.
Chu GC, Kimmelman AC, Hezel AF, 22.
DePinho RA. Stromal biology of pancre-
atic cancer. J Cell Biochem 2007;101:887-
907.
Mahadevan D, Von Hoff DD. Tumor- 23.
stroma interactions in pancreatic ductal
adenocarcinoma. Mol Cancer Ther 2007;
6:1186-97.
Masamune A, Shimosegawa T. Signal 24.
transduction in pancreatic stellate cells.
J Gastroenterol 2009;44:249-60.
Erkan M, Reiser-Erkan C, Michalski 25.
CW, et al. Cancer-stellate cell interactions
perpetuate the hypoxia-fibrosis cycle in
pancreatic ductal adenocarcinoma. Neo-
plasia 2009;11:497-508.
Zhang W, Erkan M, Abiatari I, et al. 26.
Expression of extracellular matrix metal-
loproteinase inducer (EMMPRIN/CD147)
in pancreatic neoplasm and pancreatic
stellate cells. Cancer Biol Ther 2007;6:218-
27.
Mukherjee P, Basu GD, Tinder TL, et al. 27.
Progression of pancreatic adenocarcino-
ma is significantly impeded with a com-
bination of vaccine and COX-2 inhibition.
J Immunol 2009;182:216-24.
Infante JR, Matsubayashi H, Sato N, et 28.
al. Peritumoral fibroblast SPARC expres-
sion and patient outcome with resectable
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
The new engl and journal o f medicine
n engl j med 362;17 nejm.org april 29, 2010
1616
pancreatic adenocarcinoma. J Clin Oncol
2007;25:319-25.
Olive KP, Jacobetz MA, Davidson CJ, 29.
et al. Inhibition of Hedgehog signaling
enhances delivery of chemotherapy in a
mouse model of pancreatic cancer. Science
2009;324:1457-61.
Li C, Heidt DG, Dalerba P, et al. Iden- 30.
tification of pancreatic cancer stem cells.
Cancer Res 2007;67:1030-7.
Hermann PC, Huber SL, Herrler T, 31.
et al. Distinct populations of cancer stem
cells determine tumor growth and meta-
static activity in human pancreatic cancer.
Cell Stem Cell 2007;1:313-23.
Jimeno A, Feldmann G, Surez-Gau- 32.
thier A, et al. A direct pancreatic cancer
xenograft model as a platform for cancer
stem cell therapeutic development. Mol
Cancer Ther 2009;8:310-4.
Miura F, Takada T, Amano H, Yoshida 33.
M, Furui S, Takeshita K. Diagnosis of pan-
creatic cancer. HPB (Oxford) 2006;8:337-
42.
Karmazanovsky G, Fedorov V, Kubysh- 34.
kin V, Kotchatkov A. Pancreatic head can-
cer: accuracy of CT in determination of
resectability. Abdom Imaging 2005;30:
488-500.
Dumonceau JM, Vonlaufen A. Pancre- 35.
atic endoscopic retrograde cholangiopan-
creatography (ERCP). Endoscopy 2007;39:
124-30.
Mayo SC, Austin DF, Sheppard BC, 36.
Mori M, Shipley DK, Billingsley KG. Evolv-
ing preoperative evaluation of patients
with pancreatic cancer: does laparoscopy
have a role in the current era? J Am Coll
Surg 2009;208:87-95.
Harsha HC, Kandasamy K, Rangana- 37.
than P, et al. A compendium of potential
biomarkers of pancreatic cancer. PLoS
Med 2009;6(4):e1000046.
Berger AC, Garcia M Jr, Hoffman JP, 38.
et al. Postresection CA 19-9 predicts over-
all survival in patients with pancreatic
cancer treated with adjuvant chemoradia-
tion: a prospective validation by RTOG
9704. J Clin Oncol 2008;26:5918-22.
Hess V, Glimelius B, Grawe P, et al. 39.
CA 19-9 tumour-marker response to che-
motherapy in patients with advanced pan-
creatic cancer enrolled in a randomised
controlled trial. Lancet Oncol 2008;9:
132-8.
Ferrone CR, Finkelstein DM, Thayer 40.
SP, Muzikansky A, Fernandez-del Castillo
C, Warshaw AL. Perioperative CA19-9 levels
can predict stage and survival in patients
with resectable pancreatic adenocarcino-
ma. J Clin Oncol 2006;24:2897-902.
Ko AH, Hwang J, Venook AP, Abbruz- 41.
zese JL, Bergsland EK, Tempero MA. Se-
rum CA19-9 response as a surrogate for
clinical outcome in patients receiving
fixed-dose rate gemcitabine for advanced
pancreatic cancer. Br J Cancer 2005;93:
195-9.
Greenhalf W, Grocock C, Harcus M, 42.
Neoptolemos J. Screening of high-risk
families for pancreatic cancer. Pancrea-
tology 2009;9:215-22.
Larghi A, Verna EC, Lecca PG, Costa- 43.
magna G. Screening for pancreatic cancer
in high-risk individuals: a call for endo-
scopic ultrasound. Clin Cancer Res 2009;
15:1907-14.
Edge SB, Byrd DR, Compton CC, Fritz 44.
AG, Greene FL, Trotti A, eds. AJCC can-
cer staging manual. 7th ed. New York:
Springer, 2010.
Bilimoria KY, Bentrem DJ, Ko CY, et al. 45.
Validation of the 6th edition AJCC Pancre-
atic Cancer Staging System: report from
the National Cancer Database. Cancer
2007;110:738-44.
Pawlik TM, Laheru D, Hruban RH, et 46.
al. Evaluating the impact of a single-day
multidisciplinary clinic on the manage-
ment of pancreatic cancer. Ann Surg On-
col 2008;15:2081-8.
Katz MH, Wang H, Fleming JB, et al. 47.
Long-term survival after multidisciplinary
management of resected pancreatic adeno-
carcinoma. Ann Surg Oncol 2009;16:836-
47.
Shaib Y, Davila J, Naumann C, El-Serag 48.
H. The impact of curative intent surgery
on the survival of pancreatic cancer pa-
tients: a U.S. population-based study. Am
J Gastroenterol 2007;102:1377-82.
Tseng JF, Tamm EP, Lee JE, Pisters PW, 49.
Evans DB. Venous resection in pancreatic
cancer surgery. Best Pract Res Clin Gas-
troenterol 2006;20:349-64.
Hernandez JM, Cowgill SM, Al-Saadi 50.
S, et al. CA 19-9 velocity predicts disease-
free survival and overall survival after
pancreatectomy of curative intent. J Gas-
trointest Surg 2009;13:349-53.
Slidell MB, Chang DC, Cameron JL, et 51.
al. Impact of total lymph node count and
lymph node ratio on staging and survival
after pancreatectomy for pancreatic ade-
nocarcinoma: a large, population-based
analysis. Ann Surg Oncol 2008;15:165-74.
Pausawasdi N, Scheiman J. Endoscop- 52.
ic evaluation and palliation of pancreatic
adenocarcinoma: current and future op-
tions. Curr Opin Gastroenterol 2007;23:
515-21.
Neoptolemos JP, Stocken DD, Friess H, 53.
et al. A randomized trial of chemoradio-
therapy and chemotherapy after resection
of pancreatic cancer. N Engl J Med 2004;
350:1200-10. [Erratum, N Engl J Med
2004;351:726.]
Oettle H, Post S, Neuhaus P, et al. Ad- 54.
juvant chemotherapy with gemcitabine vs
observation in patients undergoing cura-
tive-intent resection of pancreatic cancer:
a randomized controlled trial. JAMA 2007;
297:267-77.
Regine WF, Winter KA, Abrams RA, 55.
et al. Fluorouracil vs gemcitabine chemo-
therapy before and after fluorouracil-
based chemoradiation following resection
of pancreatic adenocarcinoma: a random-
ized controlled trial. JAMA 2008;299:1019-
26. [Erratum, JAMA 2008;299:1902.]
Herman JM, Swartz MJ, Hsu CC, et al. 56.
Analysis of f luorouracil-based adjuvant
chemotherapy and radiation after pancrea-
ticoduodenectomy for ductal adenocarci-
noma of the pancreas: results of a large,
prospectively collected database at the
Johns Hopkins Hospital. J Clin Oncol
2008;26:3503-10.
Raut CP, Tseng JF, Sun CC, et al. Im- 57.
pact of resection status on pattern of fail-
ure and survival after pancreaticoduo-
denectomy for pancreatic adenocarcinoma.
Ann Surg 2007;246:52-60.
Evans DB, Varadhachary GR, Crane 58.
CH, et al. Preoperative gemcitabine-based
chemoradiation for patients with resect-
able adenocarcinoma of the pancreatic
head. J Clin Oncol 2008;26:3496-502.
Katz MH, Pisters PW, Evans DB, et al. 59.
Borderline resectable pancreatic cancer:
the importance of this emerging stage of
disease. J Am Coll Surg 2008;206:833-46.
Huguet F, Andr T, Hammel P, et al. 60.
Impact of chemoradiotherapy after dis-
ease control with chemotherapy in locally
advanced pancreatic adenocarcinoma in
GERCOR phase II and III studies. J Clin
Oncol 2007;25:326-31.
Sultana A, Tudur Smith C, Cunning- 61.
ham D, et al. Systematic review, including
meta-analyses, on the management of
locally advanced pancreatic cancer using
radiation/combined modality therapy. Br J
Cancer 2007;96:1183-90.
Loehrer PJ, Powell ME, Cardenes HR, 62.
et al. A randomized phase III study of
gemcitabine in combination with radia-
tion therapy versus gemcitabine alone in
patients with localized, unresectable pan-
creatic cancer: E4201. J Clin Oncol 2008;
26:Suppl:4506. abstract.
Chauffert B, Mornex F, Bonnetain F, 63.
et al. Phase III trial comparing intensive
induction chemoradiotherapy (60 Gy, in-
fusional 5-FU and intermittent cisplatin)
followed by maintenance gemcitabine with
gemcitabine alone for locally advanced
unresectable pancreatic cancer: definitive
results of the 2000-01 FFCD/SFRO study.
Ann Oncol 2008;19:1592-9.
Burris HA III, Moore MJ, Andersen J, 64.
et al. Improvements in survival and clini-
cal benefit with gemcitabine as first-line
therapy for patients with advanced pan-
creas cancer: a randomized trial. J Clin
Oncol 1997;15:2403-13.
Sultana A, Smith CT, Cunningham D, 65.
Starling N, Neoptolemos JP, Ghaneh P.
Meta-analyses of chemotherapy for locally
advanced and metastatic pancreatic can-
cer. J Clin Oncol 2007;25:2607-15.
Heinemann V, Boeck S, Hinke A, La- 66.
bianca R, Louvet C. Meta-analysis of ran-
domized trials: evaluation of benefit from
gemcitabine-based combination chemo-
therapy applied in advanced pancreatic
cancer. BMC Cancer 2008;8:82.
Moore MJ, Goldstein D, Hamm J, et al. 67.
Erlotinib plus gemcitabine compared with
gemcitabine alone in patients with ad-
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
Medical Progress
n engl j med 362;17 nejm.org april 29, 2010
1617
vanced pancreatic cancer: a phase III trial
of the National Cancer Institute of Canada
Clinical Trials Group. J Clin Oncol 2007;
25:1960-6.
Cunningham D, Chau I, Stocken DD, 68.
et al. Phase III randomized comparison
of gemcitabine versus gemcitabine plus
capecitabine in patients with advanced
pancreatic cancer. J Clin Oncol 2009;27:
5513-8.
Xiong HQ, Varadhachary GR, Blais JC, 69.
Hess KR, Abbruzzese JL, Wolff RA. Phase
2 trial of oxaliplatin plus capecitabine
(XELOX) as second-line therapy for pa-
tients with advanced pancreatic cancer.
Cancer 2008;113:2046-52.
Kulke MH, Blaszkowsky LS, Ryan DP, 70.
et al. Capecitabine plus erlotinib in gem-
citabine-refractory advanced pancreatic
cancer. J Clin Oncol 2007;25:4787-92.
Tempero M, Plunkett W, Ruiz Van Ha- 71.
peren V, et al. Randomized phase II com-
parison of dose-intense gemcitabine:
thirty-minute infusion and fixed dose
rate infusion in patients with pancreatic
adenocarcinoma. J Clin Oncol 2003;21:
3402-8.
Louvet C, Labianca R, Hammel P, et al. 72.
Gemcitabine in combination with oxali-
platin compared with gemcitabine alone in
locally advanced or metastatic pancreatic
cancer: results of a GERCOR and GISCAD
phase III trial. J Clin Oncol 2005;23:3509-
16.
Heinemann V, Quietzsch D, Gieseler F, 73.
et al. Randomized phase III trial of gem-
citabine plus cisplatin compared with
gemcitabine alone in advanced pancreatic
cancer. J Clin Oncol 2006;24:3946-52.
Bernhard J, Dietrich D, Scheithauer W, 74.
et al. Clinical benefit and quality of life in
patients with advanced pancreatic cancer
receiving gemcitabine plus capecitabine
versus gemcitabine alone: a randomized
multicenter phase III clinical trial
SAKK 44/00-CECOG/PAN.1.3.001. J Clin
Oncol 2008;26:3695-701.
Li J, Saif MW. Any progress in the 75.
management of advanced pancreatic can-
cer? Highlights from the 45th ASCO an-
nual meeting, Orlando, FL, USA, May 29-
June 2, 2009. JOP 2009;10:361-5.
Faca VM, Song KS, Wang H, et al. 76.
A mouse to human search for plasma pro-
teome changes associated with pancreatic
tumor development. PLoS Med 2008;5(6):
e123.
Rajeshkumar NV, Tan AC, De Oliveira 77.
E, et al. Antitumor effects and biomarkers
of activity of AZD0530, a Src inhibitor, in
pancreatic cancer. Clin Cancer Res 2009;
15:4138-46.
Hewish M, Chau I, Cunningham D. 78.
Insulin-like growth factor 1 receptor tar-
geted therapeutics: novel compounds and
novel treatment strategies for cancer medi-
cine. Recent Pat Anticancer Drug Discov
2009;4:54-72.
Derosier LC, Vickers SM, Zinn KR, et al. 79.
TRA-8 anti-DR5 monoclonal antibody and
gemcitabine induce apoptosis and inhibit
radiologically validated orthotopic pan-
creatic tumor growth. Mol Cancer Ther
2007;6:3198-207.
Gold DV, Schutsky K, Modrak D, Car- 80.
dillo TM. Low-dose radioimmunotherapy
((90)Y-PAM4) combined with gemcitabine
for the treatment of experimental pancre-
atic cancer. Clin Cancer Res 2003;9:3929S-
3937S.
Chung EJ, Brown AP, Asano H, et al. 81.
In vitro and in vivo radiosensitization with
AZD6244 (ARRY-142886), an inhibitor of
mitogen-activated protein kinase/extracel-
lular signal-regulated kinase 1/2 kinase.
Clin Cancer Res 2009;15:3050-7.
Haklai R, Elad-Sfadia G, Egozi Y, 82.
Kloog Y. Orally administered FTS (salira-
sib) inhibits human pancreatic tumor
growth in nude mice. Cancer Chemother
Pharmacol 2008;61:89-96.
Wente MN, Jain A, Kono E, et al. Pros- 83.
tate stem cell antigen is a putative target
for immunotherapy in pancreatic cancer.
Pancreas 2005;31:119-25.
Hassan R, Ebel W, Routhier EL, et al. 84.
Preclinical evaluation of MORAb-009, a
chimeric antibody targeting tumor-asso-
ciated mesothelin. Cancer Immun 2007;
7:20.
Murugesan SR, King CR, Osborn R, et 85.
al. Combination of human tumor necro-
sis factor-alpha (hTNF-alpha) gene deliv-
ery with gemcitabine is effective in mod-
els of pancreatic cancer. Cancer Gene Ther
2009;16:841-7.
Rubio-Viqueira B, Hidalgo M. Direct in 86.
vivo xenograft tumor model for predicting
chemotherapeutic drug response in can-
cer patients. Clin Pharmacol Ther 2009;85:
217-21.
Farrell JJ, Elsaleh H, Garcia M, et al. 87.
Human equilibrative nucleoside trans-
porter 1 levels predict response to gemcit-
abine in patients with pancreatic cancer.
Gastroenterology 2009;136:187-95.
Copyright 2010 Massachusetts Medical Society.
IMAGES IN CLINICAL MEDICINE
The Journal welcomes consideration of new submissions for Images in Clinical
Medicine. Instructions for authors and procedures for submissions can be found
on the Journals Web site at NEJM.org. At the discretion of the editor, images that
are accepted for publication may appear in the print version of the Journal,
the electronic version, or both.
The New England Journal of Medicine
Downloaded from nejm.org on July 3, 2014. For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights reserved.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Third International Consensus Definition For Sepsis and Septic ShockDocument13 pagesThe Third International Consensus Definition For Sepsis and Septic ShockdrhendyjuniorNo ratings yet
- Anatomy & Physiology of Female Reproductive System Lecturer .Mahabad.M.koyiDocument36 pagesAnatomy & Physiology of Female Reproductive System Lecturer .Mahabad.M.koyiKarwan DilmanyNo ratings yet
- Stamets Statement Oil SpillDocument4 pagesStamets Statement Oil SpillCarlos Rafael PitirreNo ratings yet
- Innovations and Prospects in Modern Science 13 15.02.23Document481 pagesInnovations and Prospects in Modern Science 13 15.02.23Miroslav Ekman-KremenetskyNo ratings yet
- EcholocationDocument14 pagesEcholocationapi-238216496No ratings yet
- Ascent of Sap by IDS PDFDocument27 pagesAscent of Sap by IDS PDFkingNo ratings yet
- Sexual Propagation - Advantages and DisadvantagesDocument2 pagesSexual Propagation - Advantages and DisadvantagesKlint VanNo ratings yet
- Cell - 28 March 2013Document270 pagesCell - 28 March 2013Ian De La CruzNo ratings yet
- TOXONOMYDocument42 pagesTOXONOMYNanami MumuzunoNo ratings yet
- (PDF) bài tập về từ đồng nghĩaDocument98 pages(PDF) bài tập về từ đồng nghĩaminhducvn2004No ratings yet
- Lec 1 Introduction To The Course and History of PharmacyDocument4 pagesLec 1 Introduction To The Course and History of PharmacyahusainNo ratings yet
- 8-Reticuloendothelial System and Function of The SpleenDocument18 pages8-Reticuloendothelial System and Function of The SpleenHassan AhmedNo ratings yet
- XI - UNIT-10 Training and Doping in SportsDocument58 pagesXI - UNIT-10 Training and Doping in Sportspriya2kalyanNo ratings yet
- Hypnosis Progressive Muscle Relaxation Induction ScriptDocument5 pagesHypnosis Progressive Muscle Relaxation Induction Scriptlezzo sudicioNo ratings yet
- D-1-10 Horticultural Oils.198104904Document3 pagesD-1-10 Horticultural Oils.198104904ReilpeterNo ratings yet
- pGLO Bacterial Transformation Laboratory - Creating Bioluminescent Escherichia Coli By: ABADILLA, Marlo Gabriel O. BackgroundDocument3 pagespGLO Bacterial Transformation Laboratory - Creating Bioluminescent Escherichia Coli By: ABADILLA, Marlo Gabriel O. BackgroundMarloAbadillaNo ratings yet
- Response of Common Bean (Phaseolus Vulgaris L.) Cultivars To Nitrogen Fertilizer Application at Nedjo, Western EthiopiaDocument13 pagesResponse of Common Bean (Phaseolus Vulgaris L.) Cultivars To Nitrogen Fertilizer Application at Nedjo, Western EthiopiaPremier PublishersNo ratings yet
- Guidance On Registration of Similar Biological Products in SingaporeDocument13 pagesGuidance On Registration of Similar Biological Products in SingaporeWilliam ChandraNo ratings yet
- Fruit Fly Reference ManualDocument18 pagesFruit Fly Reference Manualgermain figueroaNo ratings yet
- Estimation of HeterosisDocument3 pagesEstimation of HeterosisAnkita MisalNo ratings yet
- The Importance of Developing The Whole of Oneself Focused On The Five Areas of Personal DevelopmentDocument1 pageThe Importance of Developing The Whole of Oneself Focused On The Five Areas of Personal DevelopmentEduardo BernalesNo ratings yet
- 7th Grade Scope and Sequence 15 16Document4 pages7th Grade Scope and Sequence 15 16api-292474936No ratings yet
- Neural Networks: Chapter 20, Section 5Document21 pagesNeural Networks: Chapter 20, Section 5api-19801502No ratings yet
- Handout For Week 4Document4 pagesHandout For Week 4Cheena Francesca LucianoNo ratings yet
- QIAamp DNA Mini and Blood Mini HandbookDocument72 pagesQIAamp DNA Mini and Blood Mini HandbookMaribel GatitoNo ratings yet
- 1.8 InvestigationsDocument4 pages1.8 InvestigationsJessie QianNo ratings yet
- Second Quarter Grade4fl Performance TaskDocument10 pagesSecond Quarter Grade4fl Performance TaskMark angelo BrionesNo ratings yet
- PRACTICAL 1 PharmaceuticsDocument6 pagesPRACTICAL 1 PharmaceuticsNaresh100% (1)
- Stopwatch 1 Students Book Accelerated EditionDocument12 pagesStopwatch 1 Students Book Accelerated EditioncinemaNo ratings yet
- Anthem Biosciences - OverviewDocument29 pagesAnthem Biosciences - OverviewNitish JondhaleNo ratings yet