Download as pdf or txt
You might also like
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Psoriasis Excerpts From The Edgar Cayce ReadingsDocument26 pagesPsoriasis Excerpts From The Edgar Cayce ReadingsjunghiuNo ratings yet
- Sodium Chloride Injection and Intravenous Infusion-PiDocument4 pagesSodium Chloride Injection and Intravenous Infusion-PiNg Chee LunNo ratings yet
- 11 - Novel Decision Tree Algorithms For The Treatment Planning of Compromised TeethDocument10 pages11 - Novel Decision Tree Algorithms For The Treatment Planning of Compromised TeethkochikaghochiNo ratings yet
- Serum Oxidative Stress Markers Are Not Associated With Renal and Common Carotid Arteries Arteriosclerotic Vascular Changes in Patients With GoutDocument7 pagesSerum Oxidative Stress Markers Are Not Associated With Renal and Common Carotid Arteries Arteriosclerotic Vascular Changes in Patients With GoutTeodorNo ratings yet
- Preanalytical Variables and Their Influence On The Quality of Laboratory ResultsDocument4 pagesPreanalytical Variables and Their Influence On The Quality of Laboratory Resultsapi-165321926No ratings yet
- Jurnal RingerfundinDocument7 pagesJurnal RingerfundinRyan Arifin SuryantoNo ratings yet
- Acidosis Metabolica en UciDocument5 pagesAcidosis Metabolica en UciPedro Fernando GiraldoNo ratings yet
- Evaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryDocument7 pagesEvaluation of Factors Affecting Liver Function Test in Patients Underwent Coronary Artery Bypass Graft SurgeryajmrdNo ratings yet
- 012 Analysis of Reticulocyte Parameters On The Sysmex XEDocument8 pages012 Analysis of Reticulocyte Parameters On The Sysmex XEblanket_thNo ratings yet
- Potassium Level Changes - Arrhythmia Contributing Factor in Chronic Kidney Disease PatientsDocument4 pagesPotassium Level Changes - Arrhythmia Contributing Factor in Chronic Kidney Disease PatientssigitNo ratings yet
- (Doi 10.1007/978!1!4020-9646-4 - 41) Shirahata, Sanetaka Ikura, Koji Nagao, Masaya Ichikawa, Akira - Animal Cell Technology - Basic & Applied Aspects  - Nordenau Phenomenonâ -  - Application of NaDocument7 pages(Doi 10.1007/978!1!4020-9646-4 - 41) Shirahata, Sanetaka Ikura, Koji Nagao, Masaya Ichikawa, Akira - Animal Cell Technology - Basic & Applied Aspects  - Nordenau Phenomenonâ -  - Application of NaAndry SudhariandiNo ratings yet
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- bb5 ClassifsofttissueDocument5 pagesbb5 ClassifsofttissueMuhammad MaulanaNo ratings yet
- Jurnal Yang DipakeDocument8 pagesJurnal Yang DipakeEsy LNo ratings yet
- The Role of Organic Acid Analysis in The Diagnosis of Peroxisomal Biogenesis DisordersDocument4 pagesThe Role of Organic Acid Analysis in The Diagnosis of Peroxisomal Biogenesis DisorderssaranyaNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleAshlea HunterNo ratings yet
- Inorganic Phosphorus and Potassium Are Putative Indicators of Delayed Separation of Whole BloodDocument6 pagesInorganic Phosphorus and Potassium Are Putative Indicators of Delayed Separation of Whole Bloodanon_837143581No ratings yet
- Intensive Care 1Document6 pagesIntensive Care 1raitchuNo ratings yet
- 2010-Fasting For Haematological TestDocument6 pages2010-Fasting For Haematological Testpedro vargasNo ratings yet
- Clase 7 Articulo Ejemplo 11-03-15Document8 pagesClase 7 Articulo Ejemplo 11-03-15Betzi HannlyNo ratings yet
- Reduced Albumin Dosing During Large-Volume Paracentesis Is Not Associated With Adverse Clinical OutcomesDocument6 pagesReduced Albumin Dosing During Large-Volume Paracentesis Is Not Associated With Adverse Clinical OutcomesLuis Gerardo Alcalá GonzálezNo ratings yet
- 10.1007@s10157 020 01867 yDocument6 pages10.1007@s10157 020 01867 yGin RummyNo ratings yet
- Elevated Calcium After Acute Ischemic Stroke: Association With A Poor Short-Term Outcome and Long-Term MortalityDocument6 pagesElevated Calcium After Acute Ischemic Stroke: Association With A Poor Short-Term Outcome and Long-Term MortalityMuhammad Ilham FarizNo ratings yet
- Jurnal 6Document8 pagesJurnal 6OziNo ratings yet
- Sevelamer Attenuates The Progression of Coronary and Aortic Calcification in Hemodialysis PatientsDocument8 pagesSevelamer Attenuates The Progression of Coronary and Aortic Calcification in Hemodialysis Patientsdamien333No ratings yet
- Correlation of Serum Sodiumserum Potassium ConcentDocument16 pagesCorrelation of Serum Sodiumserum Potassium ConcentItsme AyNo ratings yet
- Ijcrbm 1Document8 pagesIjcrbm 1IndahNo ratings yet
- Ijcrbm 1Document8 pagesIjcrbm 1IndahNo ratings yet
- Babandi Et Al., (2017) BJMLS, 2 (1) :: Level Among Hypertensive Patients in Kano-Nigeria BJMLS. 2Document8 pagesBabandi Et Al., (2017) BJMLS, 2 (1) :: Level Among Hypertensive Patients in Kano-Nigeria BJMLS. 2idiNo ratings yet
- BloodDocument7 pagesBloodNicol RojasNo ratings yet
- Use of A Blood Gas Analyzer and A Laboratory Autoanalyzer in Routine Practice To Measure Electrolytes in Intensive Care Unit PatientsDocument7 pagesUse of A Blood Gas Analyzer and A Laboratory Autoanalyzer in Routine Practice To Measure Electrolytes in Intensive Care Unit PatientsZheng GuNo ratings yet
- 10.1515 - CCLM 2015 0591Document7 pages10.1515 - CCLM 2015 0591fsafNo ratings yet
- Albumin DissertationDocument6 pagesAlbumin DissertationPaperWriterServicesCanada100% (1)
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- Bicnat For CKDDocument8 pagesBicnat For CKDrahmat akbarNo ratings yet
- EduardoDocument12 pagesEduardomufti dewantaraNo ratings yet
- The Influence of Blood Storage Time On The Potassium Level of Patients Receiving Packed Red Cell (PRC) Transfusion in Adam Malik General Hospital, MedanDocument6 pagesThe Influence of Blood Storage Time On The Potassium Level of Patients Receiving Packed Red Cell (PRC) Transfusion in Adam Malik General Hospital, MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Plasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationDocument5 pagesPlasma Homocysteine and Total Thiol Content in Patients With Exudative Age-Related Macular DegenerationAnonymous 1jCVqQuNo ratings yet
- 3 Lesión de Almacenamiento de EritrocitosDocument13 pages3 Lesión de Almacenamiento de EritrocitosMacarenaNo ratings yet
- Outcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationDocument5 pagesOutcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationMuhammad RizqiNo ratings yet
- Comparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaDocument7 pagesComparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Jurnal Ginjal 1 PDFDocument5 pagesJurnal Ginjal 1 PDFEva HarionoNo ratings yet
- Articulo 2 YaDocument9 pagesArticulo 2 YaLaura EscobarNo ratings yet
- Evaluation Some Biochemical Levels in Patients Undergoing Hemodialysis in Baghdad GovernorateDocument8 pagesEvaluation Some Biochemical Levels in Patients Undergoing Hemodialysis in Baghdad GovernorateKanhiya MahourNo ratings yet
- Piis2468024919301822 PDFDocument15 pagesPiis2468024919301822 PDFThinh VinhNo ratings yet
- Article: Jason C. George, Waleed Zafar, Ion Dan Bucaloiu, and Alex R. ChangDocument9 pagesArticle: Jason C. George, Waleed Zafar, Ion Dan Bucaloiu, and Alex R. ChangDesi HutapeaNo ratings yet
- 2019 Article 1596Document9 pages2019 Article 1596Arina FitrianiNo ratings yet
- Clinical Outcomes, Histopathological Patterns, and Chemical Analysis of Ayurveda and Herbal Medicine Associated With Severe Liver Injury-A Single-Center Experience From Southern IndiaDocument9 pagesClinical Outcomes, Histopathological Patterns, and Chemical Analysis of Ayurveda and Herbal Medicine Associated With Severe Liver Injury-A Single-Center Experience From Southern IndiaabbyphilipsNo ratings yet
- Blunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooDocument5 pagesBlunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooTareeqanwar MohammedNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author Manuscriptrianseptian93No ratings yet
- RLEFandECS Garlitos RoanneDocument4 pagesRLEFandECS Garlitos RoannePaul JacksonNo ratings yet
- Hiperpotasemia KDIGODocument20 pagesHiperpotasemia KDIGOAndy MaciasNo ratings yet
- Effects of Potassium Bicarbonate On Endothelial Function CV Risk Factors and Bone Turnover in Mild HypertensivesDocument9 pagesEffects of Potassium Bicarbonate On Endothelial Function CV Risk Factors and Bone Turnover in Mild HypertensivesdobrevNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument10 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaReuben JosephNo ratings yet
- Sulodexide For Kidney Protection in Type 2 Diabetes PatientsDocument8 pagesSulodexide For Kidney Protection in Type 2 Diabetes PatientsFerdinand YuzonNo ratings yet
- Dileep N. LOBO, Zeno STANGA, J. Alastair D. SIMPSON, John A. ANDERSON, Brian J. ROWLANDS and Simon P. ALLISONDocument7 pagesDileep N. LOBO, Zeno STANGA, J. Alastair D. SIMPSON, John A. ANDERSON, Brian J. ROWLANDS and Simon P. ALLISONMaria De Los AngelesNo ratings yet
- Electron Spin Resonance SpectrosDocument6 pagesElectron Spin Resonance SpectrossakuraleeshaoranNo ratings yet
- CoQ10 in Hypertension&DIABETESDocument6 pagesCoQ10 in Hypertension&DIABETESHendri YantoNo ratings yet
- As N 2015010022 Supplementary DataDocument20 pagesAs N 2015010022 Supplementary DataAndrie GunawanNo ratings yet
- Protein Damage and Antioxidant Status Alterations Caused by Oxidative Injury in Chronic Myeloid LeukemiaDocument4 pagesProtein Damage and Antioxidant Status Alterations Caused by Oxidative Injury in Chronic Myeloid LeukemiaMuhammad ArifinNo ratings yet
- Monitoring and Intervention for the Critically Ill Small Animal: The Rule of 20From EverandMonitoring and Intervention for the Critically Ill Small Animal: The Rule of 20No ratings yet
- Will Any Future Increase in Cigarette Price Reduce Smoking in Saudi Arabia?Document4 pagesWill Any Future Increase in Cigarette Price Reduce Smoking in Saudi Arabia?Mihaela-Alexandra PopNo ratings yet
- CMJ 55 3 Kit 24891284Document6 pagesCMJ 55 3 Kit 24891284Mihaela-Alexandra PopNo ratings yet
- AMP PublishingGuidelines WebDocument7 pagesAMP PublishingGuidelines WebMihaela-Alexandra PopNo ratings yet
- AnnThoracMed93134-4810599 132145Document4 pagesAnnThoracMed93134-4810599 132145Mihaela-Alexandra PopNo ratings yet
- Original Papers: Assessment of Growth Dynamics of Human Cranium Middle Fossa in Foetal PeriodDocument16 pagesOriginal Papers: Assessment of Growth Dynamics of Human Cranium Middle Fossa in Foetal PeriodMihaela-Alexandra PopNo ratings yet
- The Main Symptoms in Dorsal Sleep Apnea - Hypopnea SyndromeDocument10 pagesThe Main Symptoms in Dorsal Sleep Apnea - Hypopnea SyndromeMihaela-Alexandra PopNo ratings yet
- 27 ThangarajDocument7 pages27 ThangarajMihaela-Alexandra PopNo ratings yet
- Increased Upper Airway Cytokines and Oxidative Stress in Severe Obstructive Sleep ApnoeaDocument9 pagesIncreased Upper Airway Cytokines and Oxidative Stress in Severe Obstructive Sleep ApnoeaMihaela-Alexandra PopNo ratings yet
- Has My Patient Responded?Document5 pagesHas My Patient Responded?Mihaela-Alexandra PopNo ratings yet
- Spirometric Reference Values From A Sample of The General U.S. PopulationDocument9 pagesSpirometric Reference Values From A Sample of The General U.S. PopulationMihaela-Alexandra PopNo ratings yet
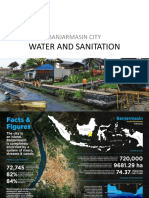
- Water and Sanitation: Banjarmasin CityDocument13 pagesWater and Sanitation: Banjarmasin CityAmelia MajidNo ratings yet
- 41 Management of Obstetric HaemorrhageDocument5 pages41 Management of Obstetric HaemorrhageParvathy R NairNo ratings yet
- Robotic-Assisted Laparoscopic Radical Prostatectomy: An Objective Assessment and Review of The LiteratureDocument12 pagesRobotic-Assisted Laparoscopic Radical Prostatectomy: An Objective Assessment and Review of The LiteratureMarwa MedNo ratings yet
- Child Psychologist Jerome Kagan On Overprescibing Drugs To Children - SPIEGEL ONLINEDocument3 pagesChild Psychologist Jerome Kagan On Overprescibing Drugs To Children - SPIEGEL ONLINEAnonymous V60yC9WNo ratings yet
- Fitzpatrick SLEDocument41 pagesFitzpatrick SLEIrene DjuardiNo ratings yet
- Prosthetics & Orthotics Clinic Procedures: Laaraib Nawaz Orthotist & ProsthetistDocument22 pagesProsthetics & Orthotics Clinic Procedures: Laaraib Nawaz Orthotist & ProsthetistGulzar AhmadNo ratings yet
- Basic First Aid For KidsDocument40 pagesBasic First Aid For KidsArceo AbiGail0% (1)
- JIAP April 2021 - Immediate Implant Placement in Periodontally Infected Sites - A Systematic Review and Meta-Analysis.Document23 pagesJIAP April 2021 - Immediate Implant Placement in Periodontally Infected Sites - A Systematic Review and Meta-Analysis.isaura sangerNo ratings yet
- Fundamentals of Edema ManagementDocument4 pagesFundamentals of Edema ManagementMoze Physio100% (1)
- What Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyDocument1 pageWhat Is Acrophobia?: Computer-Simulated Phobia PTSD Zoophobia Acrophobia U.S. NavyE. LópezNo ratings yet
- High Risk NeonatesDocument58 pagesHigh Risk Neonatesskybluedugs100% (1)
- Vesicovaginal FistulaDocument50 pagesVesicovaginal FistulaeslyNo ratings yet
- 4 F Guevara Muñoz B3 U2Document15 pages4 F Guevara Muñoz B3 U2CHRISTIAN GUEVARANo ratings yet
- Are We Ready For CannabisDocument15 pagesAre We Ready For CannabisBeatta RamirezNo ratings yet
- v7 Chronic Pain Relief TemplateDocument11 pagesv7 Chronic Pain Relief Templateravi_numl100% (1)
- Human-To-Human Relationship Model: Joyce Travelbee (1926-1973)Document17 pagesHuman-To-Human Relationship Model: Joyce Travelbee (1926-1973)Leah Abdul KabibNo ratings yet
- Basic Mulligan, Indikasi Dan Kontrakindikasi: Fitri Yani, M.FisDocument10 pagesBasic Mulligan, Indikasi Dan Kontrakindikasi: Fitri Yani, M.Fisrisa tifaNo ratings yet
- Schemas EmotionalDocument11 pagesSchemas EmotionalAnderson GaldinoNo ratings yet
- Pharmacology and The Nursing Process Lilley 6th Edition Test BankDocument5 pagesPharmacology and The Nursing Process Lilley 6th Edition Test BankStephen Breedon100% (33)
- Transient Ischemic AttackDocument5 pagesTransient Ischemic AttackVijayabala JeevaganNo ratings yet
- Renal Cortical CystDocument2 pagesRenal Cortical Cystra222j239No ratings yet
- 882 Epos PDFDocument137 pages882 Epos PDFDinar Sandi AjiNo ratings yet
- Analysis and Design of Sewage Treatment Plant: A Case Study On Vizianagaram MunicipalityDocument5 pagesAnalysis and Design of Sewage Treatment Plant: A Case Study On Vizianagaram MunicipalityPARVAIZ AHMAD KOKANo ratings yet
- Curetas Vs UltrasonicosDocument10 pagesCuretas Vs Ultrasonicosandres gabrielNo ratings yet
- Pterygium After Surgery JDocument6 pagesPterygium After Surgery JRayhan AlatasNo ratings yet
- ResumeDocument3 pagesResumeapi-284104372No ratings yet
- Anxiolytic Effect of Myristica FragransDocument7 pagesAnxiolytic Effect of Myristica FragransLiviliaMiftaNo ratings yet