Download as pdf or txt
You might also like
- Diabetus Mellitus, LeoDocument11 pagesDiabetus Mellitus, LeoinnyNo ratings yet
- Type 2 Diabetes MellitusDocument19 pagesType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Microsoft Word Document جديدDocument3 pagesMicrosoft Word Document جديدHisham EssamNo ratings yet
- Discharge Summary PDFDocument2 pagesDischarge Summary PDFbalab2311No ratings yet
- Anesthesiology Case PresDocument26 pagesAnesthesiology Case PresNasrah N. MusaNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2MTs MIFDANo ratings yet
- Diabetes MellitusDocument43 pagesDiabetes MellitusRobi HSNo ratings yet
- Diabetes MellitusDocument6 pagesDiabetes MellitusChristian YuNo ratings yet
- Review of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksDocument51 pagesReview of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksBerlia NarayaniNo ratings yet
- DM2 StatPearlsDocument14 pagesDM2 StatPearlsغاز الشمالNo ratings yet
- Diabetic PatientDocument16 pagesDiabetic PatientGabii OrdoñezNo ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationQori AdawiyahNo ratings yet
- Diabetes Mellitus PresentationDocument178 pagesDiabetes Mellitus PresentationMelesNo ratings yet
- Diabetes MellitusDocument5 pagesDiabetes MellitussujithasNo ratings yet
- Bka Case FinalDocument26 pagesBka Case FinalJayson SorianoNo ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationSmeu MirelaNo ratings yet
- IntroductionDocument22 pagesIntroductionjayrana40No ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- DM Type IiDocument6 pagesDM Type Iifarhah ayunizar ramadhaniNo ratings yet
- 05.diagnosis and Classification of Diabetes Mellitus PDFDocument6 pages05.diagnosis and Classification of Diabetes Mellitus PDFEliuth ZamoraNo ratings yet
- Diabetes Mellitus Type 2Document10 pagesDiabetes Mellitus Type 2Exia QuinagonNo ratings yet
- Diagnosis and Classification of Diabetes 2013Document8 pagesDiagnosis and Classification of Diabetes 2013Armando ATNo ratings yet
- Dr. Pragasam Viswanathan Professor, SBSTDocument43 pagesDr. Pragasam Viswanathan Professor, SBSTMaru Mengesha Worku 18BBT0285No ratings yet
- Diabetes Mellitus, Often Simply Referred To As Diabetes, Is A Group of Metabolic Diseases inDocument3 pagesDiabetes Mellitus, Often Simply Referred To As Diabetes, Is A Group of Metabolic Diseases inGanesh BalaNo ratings yet
- Definition and Diagnostic Criteria For Diabetes Mellitus and Other Categories of Glucose IntoleranceDocument4 pagesDefinition and Diagnostic Criteria For Diabetes Mellitus and Other Categories of Glucose Intolerancevai2No ratings yet
- Diabetes MellitusDocument38 pagesDiabetes Mellitusمیاں منیب احمدNo ratings yet
- Dianosis Dan Klasifikasi DMDocument8 pagesDianosis Dan Klasifikasi DMFatkhul Ali ImronNo ratings yet
- Diabetes MelitusDocument8 pagesDiabetes MelituswahyunhyNo ratings yet
- Orthodontic Considerations in The Diabetic Patient: Luc Bensch, Marc Braem, and Guy WillemsDocument7 pagesOrthodontic Considerations in The Diabetic Patient: Luc Bensch, Marc Braem, and Guy WillemsRanda KamelNo ratings yet
- Diabetes MellitusDocument6 pagesDiabetes MellitusDr Mangesti Utami PKM Kebaman BanyuwangiNo ratings yet
- Diabetes Mellitus Is A Group of Metabolic Diseases Characterized byDocument67 pagesDiabetes Mellitus Is A Group of Metabolic Diseases Characterized byBivek TimalsinaNo ratings yet
- Pedoman Diet Diabetes MelitusDocument45 pagesPedoman Diet Diabetes Melitus51limasatuNo ratings yet
- Diabetes PPT FinalDocument86 pagesDiabetes PPT FinalMohammed IbraheemNo ratings yet
- DiabetesDocument14 pagesDiabetesAaditya MallikNo ratings yet
- VERNILLO Et Al PDFDocument8 pagesVERNILLO Et Al PDFJardelSantosNo ratings yet
- Type 1 Diabetes: Classification of DMDocument3 pagesType 1 Diabetes: Classification of DMSri Agustin Purwanti 1911124848No ratings yet
- Assessment & Treatment of Diabetic Emergencies: Paramedic LevelDocument12 pagesAssessment & Treatment of Diabetic Emergencies: Paramedic LevelSarah-kate PatersonNo ratings yet
- Dad ADocument107 pagesDad Abammu21No ratings yet
- Case Report GeriatricDocument29 pagesCase Report Geriatricjoanna fitzmorrisNo ratings yet
- Session 27 Diabetes M - 1Document47 pagesSession 27 Diabetes M - 1Kuchby MskudeNo ratings yet
- Dissertation Diabetes Mellitus Type 2Document5 pagesDissertation Diabetes Mellitus Type 2Syracuse100% (1)
- Diabetes Mellitus and HomeopathyDocument9 pagesDiabetes Mellitus and HomeopathyImran Shafqat100% (2)
- PharmacologyDocument16 pagesPharmacologyRakshita JainNo ratings yet
- Diabeties NewDocument54 pagesDiabeties NewDipti SharmaNo ratings yet
- DefinitionDocument6 pagesDefinitionChana 'eLecter' ChuLumNo ratings yet
- Diabetes Mellitus (WHO)Document6 pagesDiabetes Mellitus (WHO)Aggita CahyaniNo ratings yet
- By: Emad Qassim Khaleel Ghassan Mahmood Khalaf Firas Khalaf EidoDocument38 pagesBy: Emad Qassim Khaleel Ghassan Mahmood Khalaf Firas Khalaf EidoEmad Qasim KhaleelNo ratings yet
- Diabetes Mellitus An OverviewDocument4 pagesDiabetes Mellitus An OverviewALNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2Roland Jireh MarananNo ratings yet
- Diabetes Mellitus Type 2Document3 pagesDiabetes Mellitus Type 2Licio LentimoNo ratings yet
- FND Project FinalDocument18 pagesFND Project FinalVARSHA BHOJWANINo ratings yet
- Diabetes - StatPearls - NCBI BookshelfDocument16 pagesDiabetes - StatPearls - NCBI BookshelfWidad SalsabilaNo ratings yet
- The Two-Way Relationship Between Diabetes and Periodontal DiseaseDocument12 pagesThe Two-Way Relationship Between Diabetes and Periodontal DiseaseDevi AlfianiNo ratings yet
- Diabetes MellitusDocument79 pagesDiabetes Mellituskhalid saifur rahman khanNo ratings yet
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachFrom EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNo ratings yet
- Type 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]From EverandType 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]Rating: 5 out of 5 stars5/5 (8)
- A Guide to Diabetes: Symptoms; Causes; Treatment; PreventionFrom EverandA Guide to Diabetes: Symptoms; Causes; Treatment; PreventionNo ratings yet
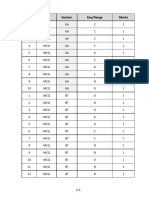
- Q.No. Type Section Key/Range MarksDocument3 pagesQ.No. Type Section Key/Range Marksbiotech_vidhyaNo ratings yet
- BT 2019Document13 pagesBT 2019biotech_vidhyaNo ratings yet
- Whole Cell ExtractDocument1 pageWhole Cell Extractbiotech_vidhyaNo ratings yet
- Buffer Preparation PDFDocument6 pagesBuffer Preparation PDFbiotech_vidhyaNo ratings yet
- Troubleshooting SDS-PAGE 1Document3 pagesTroubleshooting SDS-PAGE 1biotech_vidhyaNo ratings yet
- Polymerase Chain Reaction (PCR)Document3 pagesPolymerase Chain Reaction (PCR)biotech_vidhyaNo ratings yet
- Buffer Preparation PDFDocument6 pagesBuffer Preparation PDFbiotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Nuclear ExtractsDocument2 pagesNuclear Extractsbiotech_vidhyaNo ratings yet
- Ies 17 Set A Me Q ADocument67 pagesIes 17 Set A Me Q Abiotech_vidhyaNo ratings yet
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Document20 pagesMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaNo ratings yet
- 1 TolerancesDocument1 page1 Tolerancesbiotech_vidhyaNo ratings yet
- Befcv List PDFDocument22 pagesBefcv List PDFbiotech_vidhyaNo ratings yet
- Lec09 Three PhaseDocument84 pagesLec09 Three Phasebiotech_vidhyaNo ratings yet
- Teachers Recruitment Board: 1. Important DatesDocument13 pagesTeachers Recruitment Board: 1. Important Datesbiotech_vidhyaNo ratings yet
- Isa BusDocument30 pagesIsa Busbiotech_vidhya100% (1)
- Diabetic Emergencies During Ramadan FastingDocument4 pagesDiabetic Emergencies During Ramadan FastingAmany SalamaNo ratings yet
- Dietary Treatment ObesityDocument52 pagesDietary Treatment Obesitymark pavlovicNo ratings yet
- 002 Pediatric Obesity An IntroductionDocument24 pages002 Pediatric Obesity An IntroductionAnurag BhatejaNo ratings yet
- Diabetic Retinopathy: Clinical Findings and Management: Review ArticleDocument4 pagesDiabetic Retinopathy: Clinical Findings and Management: Review ArticlewadejackNo ratings yet
- Insulin TherapyDocument62 pagesInsulin TherapyCharisma Bimara CozyNo ratings yet
- Practice QuestionsDocument10 pagesPractice Questionsdabervid230% (1)
- Met 2008 0065 PDFDocument10 pagesMet 2008 0065 PDFDeedee RenovaldiNo ratings yet
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocument20 pagesDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- The Other Diabetes - LADA, or Type 1Document3 pagesThe Other Diabetes - LADA, or Type 1rey_fremyNo ratings yet
- Carbohydrates SummaryDocument9 pagesCarbohydrates SummaryHarold NagunaNo ratings yet
- HypoglicemiaDocument4 pagesHypoglicemiayeniNo ratings yet
- HypertriglyceridemiaDocument8 pagesHypertriglyceridemiaNaila KhanNo ratings yet
- AACE-ACE - Practice Guidelines For Developing Diabete MellitusDocument87 pagesAACE-ACE - Practice Guidelines For Developing Diabete MellitusDottNo ratings yet
- Tugas Critical Appraisal Jurnal Bu AnnaDocument8 pagesTugas Critical Appraisal Jurnal Bu AnnaerlanggawidyaputriNo ratings yet
- Chapter 47 Diabetes Mellitus PDFDocument14 pagesChapter 47 Diabetes Mellitus PDFRLLT100% (1)
- DM AAFP ManagementDocument8 pagesDM AAFP ManagementphilsguNo ratings yet
- Algorithms For The Automated Detection of Diabetic Retinopathy Using Digital Fundus Images: A ReviewDocument13 pagesAlgorithms For The Automated Detection of Diabetic Retinopathy Using Digital Fundus Images: A ReviewAbderrahmane ElbaalaouiNo ratings yet
- 13Document203 pages13Carlos HernándezNo ratings yet
- Malnutrition in Older Adults: An Evidence-Based Review of Risk Factors, Assessment, and InterventionDocument8 pagesMalnutrition in Older Adults: An Evidence-Based Review of Risk Factors, Assessment, and InterventionDago DagoNo ratings yet
- Obesity Prevention and Education For School Nurses Community Health NursingDocument66 pagesObesity Prevention and Education For School Nurses Community Health NursingGabrielaNo ratings yet
- Pathophysiology of Carbohydrates MetabolismDocument54 pagesPathophysiology of Carbohydrates MetabolismMaui TingNo ratings yet
- MCQDocument6 pagesMCQدرالجمانNo ratings yet
- Obesity Case StudyDocument4 pagesObesity Case Studydsaitta108No ratings yet
- Soap Note PracticeDocument45 pagesSoap Note PracticeErica Conner MenendezNo ratings yet
- DIABETES ProjectDocument26 pagesDIABETES ProjectIshq KaurNo ratings yet
- Collins Cambridge IGCSE English As A Second Language Student WorkbookDocument16 pagesCollins Cambridge IGCSE English As A Second Language Student WorkbookQibthiyah SavitriNo ratings yet
- TeneligliptinDocument17 pagesTeneligliptintarun956519No ratings yet
- Diabetes Prevention and Control Program Chapter 5Document24 pagesDiabetes Prevention and Control Program Chapter 5Wendy EscalanteNo ratings yet


























































![Type 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]](https://imgv2-2-f.scribdassets.com/img/word_document/616633879/149x198/173640cf06/1710278044?v=1)