
Atients Hospitalized After Initial Outpatient Treatment For Community-Acquired Pneumonia
Atients Hospitalized After Initial Outpatient Treatment For Community-Acquired Pneumonia
You might also like
- Ineffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive CoughDocument1 pageIneffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive Coughdana93% (30)
- Assessment and Management of Preoperative Anxiety: London, United KingdomDocument6 pagesAssessment and Management of Preoperative Anxiety: London, United KingdomrsudabadiNo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaEd BarajasNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Pratiwi AyuningtyasNo ratings yet
- Treatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsDocument5 pagesTreatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsSyairah Banu DjufriNo ratings yet
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDocument4 pagesThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNo ratings yet
- Long-Stay of PICU in SepsisDocument6 pagesLong-Stay of PICU in SepsisSanti IskandarNo ratings yet
- Coach 2023Document11 pagesCoach 2023Guilherme CarelliNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- High-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisDocument10 pagesHigh-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisSoleh SundawaNo ratings yet
- Chan 2004Document8 pagesChan 2004clinica cuelloNo ratings yet
- Selected Topics: Prehospital CareDocument9 pagesSelected Topics: Prehospital CareYo MeNo ratings yet
- Two-Year Survival Comparing Web-Based Symptom Monitoring Vs Routine Surveillance Following Treatment For Lung CancerDocument6 pagesTwo-Year Survival Comparing Web-Based Symptom Monitoring Vs Routine Surveillance Following Treatment For Lung CancerValerie LascauxNo ratings yet
- Huang 2018Document14 pagesHuang 2018amazeyragNo ratings yet
- PROCESSDocument11 pagesPROCESSandrea vargasNo ratings yet
- Oral AbstractsDocument210 pagesOral AbstractspascutaNo ratings yet
- Procalcitonin PneumoniaDocument14 pagesProcalcitonin PneumoniaMr. LNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- Low Dose Prednisolone in Community Acquired PneumoniaDocument15 pagesLow Dose Prednisolone in Community Acquired PneumoniaIsaac SalazarNo ratings yet
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDocument5 pagesAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaNo ratings yet
- Valacyclovir For Episodic Treatment of Genital Herpes: A Shorter 3-Day Treatment Course Compared With 5-Day TreatmentDocument5 pagesValacyclovir For Episodic Treatment of Genital Herpes: A Shorter 3-Day Treatment Course Compared With 5-Day TreatmentEpi PanjaitanNo ratings yet
- Journal Presentation: Presented By-Vidisha Adarsh MPT (Neurosciences) Evaluator - Dr. Kritika Sharma (PT)Document51 pagesJournal Presentation: Presented By-Vidisha Adarsh MPT (Neurosciences) Evaluator - Dr. Kritika Sharma (PT)Urvashi SilalNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Discharge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectDocument17 pagesDischarge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectMukhlis HasNo ratings yet
- Goal-Directed Resuscitation For Patients With Early Septic ShockDocument11 pagesGoal-Directed Resuscitation For Patients With Early Septic ShockmmsNo ratings yet
- P2.06-041 Telenursing: A Thoracic Surgery Nursing Initiative Aimed at Decreasing Hospital Readmissions and Increasing Patient SatisfactionDocument2 pagesP2.06-041 Telenursing: A Thoracic Surgery Nursing Initiative Aimed at Decreasing Hospital Readmissions and Increasing Patient Satisfactionervina wulandariNo ratings yet
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDocument6 pagesEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahNo ratings yet
- Case Study #3Document26 pagesCase Study #3Reshma MohabeirNo ratings yet
- Medication-Related Problems in Critical Care Survivors - A Systematic ReviewDocument7 pagesMedication-Related Problems in Critical Care Survivors - A Systematic ReviewenesNo ratings yet
- Randomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureDocument7 pagesRandomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureThyka MayasariNo ratings yet
- Daily Interruption of Sedation in Patients Treated With Mechanical VentilationDocument4 pagesDaily Interruption of Sedation in Patients Treated With Mechanical VentilationMark_LiGx_8269No ratings yet
- G-4 Presentation DoneDocument24 pagesG-4 Presentation DoneAbdulrhman 123No ratings yet
- Search BMJ GroupDocument23 pagesSearch BMJ GroupCharles BrooksNo ratings yet
- Chlo Ramp He NicolDocument6 pagesChlo Ramp He NicolDivika ShilvanaNo ratings yet
- Breast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsDocument11 pagesBreast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsAn'umillah Arini ZidnaNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- THR RehabilitationDocument5 pagesTHR RehabilitationWei-Ting WuNo ratings yet
- Cisplatin-Based Adjuvant Chemotherapy in Patients With Completely Resected Non-Small-Cell Lung CancerDocument10 pagesCisplatin-Based Adjuvant Chemotherapy in Patients With Completely Resected Non-Small-Cell Lung CancerSouvik SahaNo ratings yet
- The Quality of Discharge Care Planning in Acute Stroke Care: Influencing Factors and Association With Postdischarge OutcomesDocument8 pagesThe Quality of Discharge Care Planning in Acute Stroke Care: Influencing Factors and Association With Postdischarge OutcomesnindyaNo ratings yet
- CRA 2010-Poster-PresentationsDocument236 pagesCRA 2010-Poster-PresentationsJoe GassNo ratings yet
- 2009hetrase CCMDocument12 pages2009hetrase CCMgiseladelarosa2006No ratings yet
- Out Come StudyDocument12 pagesOut Come StudyjaraNo ratings yet
- MeduloblastomaDocument7 pagesMeduloblastomasilvia erfanNo ratings yet
- Cannabis 10Document7 pagesCannabis 10CARLOS HERNAN FERNANDEZ CORDOBESNo ratings yet
- CMA AntibioticsDocument11 pagesCMA AntibioticsNovita Oktavianti DehiNo ratings yet
- Effect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDocument8 pagesEffect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDyla FaradhylaNo ratings yet
- ,adherence, 2008Document8 pages,adherence, 2008Abdurhman SeidNo ratings yet
- Journal Reading Etika MarcoDocument26 pagesJournal Reading Etika MarcoMarco GunawanNo ratings yet
- Pirfenidone and Nintedanib Compliance and Persistence in A Real World SettingDocument2 pagesPirfenidone and Nintedanib Compliance and Persistence in A Real World SettingmaleticjNo ratings yet
- Review 20 - 03 - 20 - 001Document18 pagesReview 20 - 03 - 20 - 001Ulices QuintanaNo ratings yet
- AddgfhgkklDocument10 pagesAddgfhgkklEza YusraNo ratings yet
- Farach 2014Document5 pagesFarach 2014mia widiastutiNo ratings yet
- IOI140094supp1 ProdDocument10 pagesIOI140094supp1 ProdArrizqi Ramadhani MuchtarNo ratings yet
- Which Patients Will Benefit From Psychosocial Intervention After Cystectomy For Bladder Cancer?Document8 pagesWhich Patients Will Benefit From Psychosocial Intervention After Cystectomy For Bladder Cancer?jedan185No ratings yet
- Pzad 183Document11 pagesPzad 183anvesh.jallapally.68No ratings yet
- Antibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.HDocument2 pagesAntibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.Hchebonk13No ratings yet
- Embedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyDocument17 pagesEmbedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyAnatha ChrisciliaNo ratings yet
- Early Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureDocument6 pagesEarly Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureTakashi NakamuraNo ratings yet
- Review of Acute Cancer Beds 1Document2 pagesReview of Acute Cancer Beds 1Cepi Ridwan FerdiansyahNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Hirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersDocument139 pagesHirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersJhoms Poja FeriaNo ratings yet
- Medical Bacteriology (460 MIC) : Bacterial - Host RelationshipsDocument11 pagesMedical Bacteriology (460 MIC) : Bacterial - Host RelationshipsMuna Moh'dNo ratings yet
- Human ORFeome Gateway Entry Vector PENTR223Document6 pagesHuman ORFeome Gateway Entry Vector PENTR223Dave RapaconNo ratings yet
- Puttur DetailDocument12 pagesPuttur DetailakileshNo ratings yet
- SAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaDocument25 pagesSAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaMark CheneyNo ratings yet
- New Jersey Health Department Report RE: Dr. John VecchioneDocument11 pagesNew Jersey Health Department Report RE: Dr. John VecchioneNews12NJWebNo ratings yet
- SORL DEP Workout Phase 1Document17 pagesSORL DEP Workout Phase 1Anonymous pOggsIhOMNo ratings yet
- Joint Commision RegulationsDocument12 pagesJoint Commision Regulationsapi-223525467No ratings yet
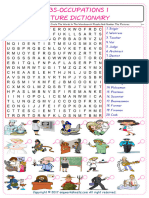
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- Chemical Constituents From The Stems Of: Celastrus OrbiculatusDocument5 pagesChemical Constituents From The Stems Of: Celastrus OrbiculatusTuan PhamquocNo ratings yet
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- Model AnalysisDocument7 pagesModel Analysissrishti jainNo ratings yet
- Aspartame Side EffectsDocument3 pagesAspartame Side Effectsnettie95No ratings yet
- Imogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSDocument3 pagesImogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSinfo7462100% (1)
- MDocument86 pagesMeheidariNo ratings yet
- PathologyDocument4 pagesPathologyVISHAKHANo ratings yet
- Critical Care EnvironmentDocument16 pagesCritical Care EnvironmentJeffrey KauvaNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Stephen's Story: A 19 Year Old'S Life Lessons OnDocument16 pagesStephen's Story: A 19 Year Old'S Life Lessons OnSylvia DobsonNo ratings yet
- Your Electro Vibratory Body 13MB Re OCRedDocument305 pagesYour Electro Vibratory Body 13MB Re OCRedDanilo TorresNo ratings yet
- Nursing TheoryDocument15 pagesNursing TheoryTherese CanapiNo ratings yet
- SimuDocument13 pagesSimuPrince Rener Velasco PeraNo ratings yet
- Laporan Home Visit (Revin)Document24 pagesLaporan Home Visit (Revin)marinNo ratings yet
- Discontinuing An Intravenous InfusionDocument2 pagesDiscontinuing An Intravenous InfusionAgustin TrinaNo ratings yet
- Levetiracetam in Refractory Pediatric EpilepsyDocument11 pagesLevetiracetam in Refractory Pediatric EpilepsyAdlinaNo ratings yet
- Closed Fracture of Middle ClaviculaDocument12 pagesClosed Fracture of Middle ClaviculachiciNo ratings yet
- Cystic Lung Disease2Document26 pagesCystic Lung Disease2Shoban RajNo ratings yet
- DR Prathap C ReddyDocument4 pagesDR Prathap C ReddyShakin ShaNo ratings yet

























































































Download as pdf or txt
You might also like
- Ineffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive CoughDocument1 pageIneffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive Coughdana93% (30)
- Assessment and Management of Preoperative Anxiety: London, United KingdomDocument6 pagesAssessment and Management of Preoperative Anxiety: London, United KingdomrsudabadiNo ratings yet
- Critical Care Goals and ObjectivesDocument28 pagesCritical Care Goals and ObjectivesjyothiNo ratings yet
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaEd BarajasNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Pratiwi AyuningtyasNo ratings yet
- Treatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsDocument5 pagesTreatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsSyairah Banu DjufriNo ratings yet
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDocument4 pagesThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNo ratings yet
- Long-Stay of PICU in SepsisDocument6 pagesLong-Stay of PICU in SepsisSanti IskandarNo ratings yet
- Coach 2023Document11 pagesCoach 2023Guilherme CarelliNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- High-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisDocument10 pagesHigh-Dose Rifapentine With Moxifloxacin For Pulmonary TuberculosisSoleh SundawaNo ratings yet
- Chan 2004Document8 pagesChan 2004clinica cuelloNo ratings yet
- Selected Topics: Prehospital CareDocument9 pagesSelected Topics: Prehospital CareYo MeNo ratings yet
- Two-Year Survival Comparing Web-Based Symptom Monitoring Vs Routine Surveillance Following Treatment For Lung CancerDocument6 pagesTwo-Year Survival Comparing Web-Based Symptom Monitoring Vs Routine Surveillance Following Treatment For Lung CancerValerie LascauxNo ratings yet
- Huang 2018Document14 pagesHuang 2018amazeyragNo ratings yet
- PROCESSDocument11 pagesPROCESSandrea vargasNo ratings yet
- Oral AbstractsDocument210 pagesOral AbstractspascutaNo ratings yet
- Procalcitonin PneumoniaDocument14 pagesProcalcitonin PneumoniaMr. LNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- Low Dose Prednisolone in Community Acquired PneumoniaDocument15 pagesLow Dose Prednisolone in Community Acquired PneumoniaIsaac SalazarNo ratings yet
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDocument5 pagesAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaNo ratings yet
- Valacyclovir For Episodic Treatment of Genital Herpes: A Shorter 3-Day Treatment Course Compared With 5-Day TreatmentDocument5 pagesValacyclovir For Episodic Treatment of Genital Herpes: A Shorter 3-Day Treatment Course Compared With 5-Day TreatmentEpi PanjaitanNo ratings yet
- Journal Presentation: Presented By-Vidisha Adarsh MPT (Neurosciences) Evaluator - Dr. Kritika Sharma (PT)Document51 pagesJournal Presentation: Presented By-Vidisha Adarsh MPT (Neurosciences) Evaluator - Dr. Kritika Sharma (PT)Urvashi SilalNo ratings yet
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocument12 pagesOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNo ratings yet
- Discharge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectDocument17 pagesDischarge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectMukhlis HasNo ratings yet
- Goal-Directed Resuscitation For Patients With Early Septic ShockDocument11 pagesGoal-Directed Resuscitation For Patients With Early Septic ShockmmsNo ratings yet
- P2.06-041 Telenursing: A Thoracic Surgery Nursing Initiative Aimed at Decreasing Hospital Readmissions and Increasing Patient SatisfactionDocument2 pagesP2.06-041 Telenursing: A Thoracic Surgery Nursing Initiative Aimed at Decreasing Hospital Readmissions and Increasing Patient Satisfactionervina wulandariNo ratings yet
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDocument6 pagesEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahNo ratings yet
- Case Study #3Document26 pagesCase Study #3Reshma MohabeirNo ratings yet
- Medication-Related Problems in Critical Care Survivors - A Systematic ReviewDocument7 pagesMedication-Related Problems in Critical Care Survivors - A Systematic ReviewenesNo ratings yet
- Randomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureDocument7 pagesRandomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureThyka MayasariNo ratings yet
- Daily Interruption of Sedation in Patients Treated With Mechanical VentilationDocument4 pagesDaily Interruption of Sedation in Patients Treated With Mechanical VentilationMark_LiGx_8269No ratings yet
- G-4 Presentation DoneDocument24 pagesG-4 Presentation DoneAbdulrhman 123No ratings yet
- Search BMJ GroupDocument23 pagesSearch BMJ GroupCharles BrooksNo ratings yet
- Chlo Ramp He NicolDocument6 pagesChlo Ramp He NicolDivika ShilvanaNo ratings yet
- Breast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsDocument11 pagesBreast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsAn'umillah Arini ZidnaNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- THR RehabilitationDocument5 pagesTHR RehabilitationWei-Ting WuNo ratings yet
- Cisplatin-Based Adjuvant Chemotherapy in Patients With Completely Resected Non-Small-Cell Lung CancerDocument10 pagesCisplatin-Based Adjuvant Chemotherapy in Patients With Completely Resected Non-Small-Cell Lung CancerSouvik SahaNo ratings yet
- The Quality of Discharge Care Planning in Acute Stroke Care: Influencing Factors and Association With Postdischarge OutcomesDocument8 pagesThe Quality of Discharge Care Planning in Acute Stroke Care: Influencing Factors and Association With Postdischarge OutcomesnindyaNo ratings yet
- CRA 2010-Poster-PresentationsDocument236 pagesCRA 2010-Poster-PresentationsJoe GassNo ratings yet
- 2009hetrase CCMDocument12 pages2009hetrase CCMgiseladelarosa2006No ratings yet
- Out Come StudyDocument12 pagesOut Come StudyjaraNo ratings yet
- MeduloblastomaDocument7 pagesMeduloblastomasilvia erfanNo ratings yet
- Cannabis 10Document7 pagesCannabis 10CARLOS HERNAN FERNANDEZ CORDOBESNo ratings yet
- CMA AntibioticsDocument11 pagesCMA AntibioticsNovita Oktavianti DehiNo ratings yet
- Effect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDocument8 pagesEffect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDyla FaradhylaNo ratings yet
- ,adherence, 2008Document8 pages,adherence, 2008Abdurhman SeidNo ratings yet
- Journal Reading Etika MarcoDocument26 pagesJournal Reading Etika MarcoMarco GunawanNo ratings yet
- Pirfenidone and Nintedanib Compliance and Persistence in A Real World SettingDocument2 pagesPirfenidone and Nintedanib Compliance and Persistence in A Real World SettingmaleticjNo ratings yet
- Review 20 - 03 - 20 - 001Document18 pagesReview 20 - 03 - 20 - 001Ulices QuintanaNo ratings yet
- AddgfhgkklDocument10 pagesAddgfhgkklEza YusraNo ratings yet
- Farach 2014Document5 pagesFarach 2014mia widiastutiNo ratings yet
- IOI140094supp1 ProdDocument10 pagesIOI140094supp1 ProdArrizqi Ramadhani MuchtarNo ratings yet
- Which Patients Will Benefit From Psychosocial Intervention After Cystectomy For Bladder Cancer?Document8 pagesWhich Patients Will Benefit From Psychosocial Intervention After Cystectomy For Bladder Cancer?jedan185No ratings yet
- Pzad 183Document11 pagesPzad 183anvesh.jallapally.68No ratings yet
- Antibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.HDocument2 pagesAntibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.Hchebonk13No ratings yet
- Embedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyDocument17 pagesEmbedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyAnatha ChrisciliaNo ratings yet
- Early Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureDocument6 pagesEarly Intensive Care Unit Mobility Therapy in The Treatment of Acute Respiratory FailureTakashi NakamuraNo ratings yet
- Review of Acute Cancer Beds 1Document2 pagesReview of Acute Cancer Beds 1Cepi Ridwan FerdiansyahNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Hirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersDocument139 pagesHirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersJhoms Poja FeriaNo ratings yet
- Medical Bacteriology (460 MIC) : Bacterial - Host RelationshipsDocument11 pagesMedical Bacteriology (460 MIC) : Bacterial - Host RelationshipsMuna Moh'dNo ratings yet
- Human ORFeome Gateway Entry Vector PENTR223Document6 pagesHuman ORFeome Gateway Entry Vector PENTR223Dave RapaconNo ratings yet
- Puttur DetailDocument12 pagesPuttur DetailakileshNo ratings yet
- SAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaDocument25 pagesSAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaMark CheneyNo ratings yet
- New Jersey Health Department Report RE: Dr. John VecchioneDocument11 pagesNew Jersey Health Department Report RE: Dr. John VecchioneNews12NJWebNo ratings yet
- SORL DEP Workout Phase 1Document17 pagesSORL DEP Workout Phase 1Anonymous pOggsIhOMNo ratings yet
- Joint Commision RegulationsDocument12 pagesJoint Commision Regulationsapi-223525467No ratings yet
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- Chemical Constituents From The Stems Of: Celastrus OrbiculatusDocument5 pagesChemical Constituents From The Stems Of: Celastrus OrbiculatusTuan PhamquocNo ratings yet
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- Model AnalysisDocument7 pagesModel Analysissrishti jainNo ratings yet
- Aspartame Side EffectsDocument3 pagesAspartame Side Effectsnettie95No ratings yet
- Imogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSDocument3 pagesImogen Edwards-Jones, The Woman Behind Hotel Babylon, Is Training Her Sights On The Unlikeliest of Targets: The NHSinfo7462100% (1)
- MDocument86 pagesMeheidariNo ratings yet
- PathologyDocument4 pagesPathologyVISHAKHANo ratings yet
- Critical Care EnvironmentDocument16 pagesCritical Care EnvironmentJeffrey KauvaNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Stephen's Story: A 19 Year Old'S Life Lessons OnDocument16 pagesStephen's Story: A 19 Year Old'S Life Lessons OnSylvia DobsonNo ratings yet
- Your Electro Vibratory Body 13MB Re OCRedDocument305 pagesYour Electro Vibratory Body 13MB Re OCRedDanilo TorresNo ratings yet
- Nursing TheoryDocument15 pagesNursing TheoryTherese CanapiNo ratings yet
- SimuDocument13 pagesSimuPrince Rener Velasco PeraNo ratings yet
- Laporan Home Visit (Revin)Document24 pagesLaporan Home Visit (Revin)marinNo ratings yet
- Discontinuing An Intravenous InfusionDocument2 pagesDiscontinuing An Intravenous InfusionAgustin TrinaNo ratings yet
- Levetiracetam in Refractory Pediatric EpilepsyDocument11 pagesLevetiracetam in Refractory Pediatric EpilepsyAdlinaNo ratings yet
- Closed Fracture of Middle ClaviculaDocument12 pagesClosed Fracture of Middle ClaviculachiciNo ratings yet
- Cystic Lung Disease2Document26 pagesCystic Lung Disease2Shoban RajNo ratings yet
- DR Prathap C ReddyDocument4 pagesDR Prathap C ReddyShakin ShaNo ratings yet