Professional Documents
Culture Documents
The Immune Response in
The Immune Response in
Uploaded by
Alexis Jesus GomezOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
The Immune Response in
The Immune Response in
Uploaded by
Alexis Jesus GomezCopyright:
Available Formats
Atherosclerosis is an inflammatory disease characterized
by intense immunological activity, which increasingly
threatens human health worldwide
1
. Atherosclerosis
involves the formation in the arteries of lesions that
are characterized by inflammation, lipid accumula-
tion, cell death and fibrosis. Over time, these lesions,
which are known as atherosclerotic plaques, mature and
gain new characteristics. Although clinical complica-
tions of atherosclerosis can arise from plaques causing
flow-limiting stenoses, the most severe clinical events
follow the rupture of a plaque, which exposes the pro-
thrombotic material in the plaque to the blood and
causes sudden thrombotic occlusion of the artery at
the site of disruption. In the heart, atherosclerosis can
lead to myocardial infarction and heart failure; whereas in
the arteries that perfuse the brain, it can cause ischaemic
stroke and transient ischaemic attacks. If atherosclero-
sis affects other arterial branches, it can result in renal
impairment, hypertension, abdominal aortic aneurysms
and critical limb ischaemia. As our knowledge of this
disease increases, we increasingly recognize that there is
no simple answer to the question of whether the immune
response promotes or retards atherogenesis. Indeed, the
two arms of the immune response can either promote
or attenuate aspects of atherosclerosis and its complica-
tions. This Review summarizes our current understand-
ing of the role of adaptive immunity in atherosclerosis
and, in particular, weighs the evidence regarding the
yin and yang of the immune response at various places
and times in the evolution of this lengthy and complex
disease. We do not discuss the arteriosclerosis of allo-
grafted transplants, which is a distinct disease with a
unique pathogenesis, although it might represent an
extreme case of immune-driven arteriopathy.
Immunological features of atherosclerosis
In humans, atherosclerotic plaques contain blood-borne
inflammatory and immune cells (mainly macrophages
and T cells), as well as vascular endothelial cells, smooth
muscle cells, extracellular matrix, lipids and acellular
lipid-rich debris
2
. These lesions typically present as
asymmetrical focal thickenings of the intima, which is
the innermost layer of the artery (FIG. 1). Accumulation
of immune cells and lipid droplets in the intima occurs
during the first stage of plaque formation. Lipid-laden
macrophages, known as foam cells, outnumber other
cells in early plaques (which are known as fatty streaks),
but these nascent plaques also contain T cells. Fatty
streaks are prevalent in young individuals, never cause
symptoms, and can progress into mature atherosclerotic
plaques or disappear with time.
Mature plaques (also known as atheromas) have a
more complex structure than fatty streaks (FIG. 1). In
the centre of a plaque, foam cells and extracellular lipid
droplets form a core region that is surrounded by a cap
of smooth muscle cells and a collagen-rich matrix
2
.
Other cell types present in plaques include dendritic cells
(DCs)
3
, mast cells
4
, a few B cells
2
and probably natural
killer T (NKT) cells. The shoulder region of the plaque,
which is where it grows, and the interface between the
cap and the core have particularly abundant accumu-
lations of T cells and macrophages
2
. Many of these
immune cells show signs of activation and produce pro-
inflammatory cytokines such as interferon- (IFN) and
*Center for Molecular
Medicine, Department
of Medicine, Karolinska
University Hospital,
Karolinska Institute,
Stockholm, SE-17176,
Sweden.
Leducq Transatlantic
Network of Excellence in
Cardiovascular Research,
Brigham and Womens
Hospital and Harvard
Medical School, Boston,
Massachusetts, USA.
Donald W. Reynolds
Cardiovascular Clinical
Research Center, Department
of Medicine, Brigham
and Womens Hospital and
Harvard Medical School,
Boston, Massachusetts
02115, USA.
Correspondence to P.L.
e-mail:
plibby@rics.bwh.harvard.edu
doi:10.1038/nri1882
Published online
16 June 2006
Plaque
An atherosclerotic lesion
consisting of a fibrotic cap
surrounding a lipid-rich core.
The lesion is the site of
inflammation, lipid
accumulation and cell death.
Also known as an atheroma.
The immune response in
atherosclerosis: a double-edged sword
Gran K. Hansson *
and Peter Libby
Abstract | Immune responses participate in every phase of atherosclerosis. There is
increasing evidence that both adaptive and innate immunity tightly regulate atherogenesis.
Although improved treatment of hyperlipidaemia reduces the risk for cardiac and cerebral
complications of atherosclerosis, these remain among the most prevalent of diseases
and will probably become the most common cause of death globally within 15 years.
This Review focuses on the role of immune mechanisms in the formation and activation of
atherosclerotic plaques, and also includes a discussion of the use of inflammatory markers
for predicting cardiovascular events. We also outline possible future targets for prevention,
diagnosis and treatment of atherosclerosis.
REVI EWS
508 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
Cellular debris
and cholesterol
Shoulder
Media
Blood-vessel lumen
Endothelial cell
Normal artery
Elastic lamina
Intima
Media
Foam cell T cell Macrophage Mast cell Monocyte Cholesterol Dendritic cell Dead cell
Smooth
muscle cell
Myocardial infarction
An episode of acute cardiac
ischaemia that leads to death
of heart muscle cells. It is
usually caused by a thrombotic
atherosclerotic plaque.
Ischaemic stroke
An episode of acute regional
ischaemia in the brain leading
to nerve-cell death. It is usually
caused by thrombi or emboli
from atherosclerotic plaques.
Aneurysm
The local dilatation of an artery
caused by weakening of the
artery wall. Some, but not all,
aneurysms are caused by
atherosclerosis.
Intima
The innermost layer of an
artery, which consists of loose
connective tissue and is
covered by a monolayer of
endothelium. Atherosclerotic
plaques form in the intima.
Fibrous cap
A structure composed of a
dense collagen-rich
extracellular matrix with
occasional smooth muscle
cells, macrophages and T cells
that typically overlies the
characteristic central lipid core
of plaques.
tumour-necrosis factor (TNF)
5
. With time, the plaque
can progress into an even more complex lesion, the
lipid core of which has become a paucicellular pool of
cholesterol deposits surrounded by a fibrous cap of vary-
ing thickness. The fibrous cap prevents contact between
the blood and the pro-thrombotic material in the lesion
(FIG. 1). Disruption of the cap can lead to thrombosis and
many of the adverse clinical outcomes associated with
atherosclerosis.
Models of atherogenesis in mutant mice
Direct analysis of the early phases of human athero sclerosis
presents obvious obstacles. Therefore, systematic inves-
tigation of the mechanisms that initiate athero sclerosis
relies on animal models of the disease. The available
observations indicate that there is substantial overlap
between disease development in these animal models and
the human disease. Two strains of genetically altered mice
have been particularly fruitful in this regard. Apoe
/
mice lack apolipoprotein E (APOE; which is a key
component in cholesterol metabolism), and develop
spontaneous hypercholesterolaemia and atherosclerotic
disease (which is exacerbated by an atherogenic diet)
that progresses to myocardial infarction and stroke
6,7
.
Low-density-lipoprotein receptor (LDLR)-deficient mice
respond to being fed with fat by developing hypercholes-
terolaemia and atherosclerotic plaques
8
. The crossbreed-
ing of these mice with mice that carry deletions in genes
encoding crucial components of the immune system
has provided important information on the role of the
immune system in the pathogenesis of atherosclerosis. In
addition, bone-marrow transplantation of, and spleen-cell
transfer to, Apoe
/
or Ldlr
/
mice has offered insights into
the role of specific populations of bone-marrow-derived
cells in disease development.
Immune-cell recruitment initiates atherosclerotic-
plaque formation. In experimental animals, endothelial
cells in the arteries express leukocyte adhesion mol-
ecules, in particular vascular cell-adhesion molecule 1
(VCAM1), as part of the initial vascular response to
cholesterol accumulation in the intima
9
(FIG. 2a). The
patchy distribution of adhesion-molecule expression
corresponds to the subsequent position at which fatty
streaks form
10
. This patchy pattern of expression prob-
ably reflects haemodynamic factors, because the shear
stresses and disturbed fluid flows vary over the arterial
bed in a similar way to the predilection sites for athero-
sclerosis. Interestingly, exposing cultured endothelial
cells to oscillatory shear stress that mimics arterial
blood flow increases the expression of several leukocyte
adhesion molecules
11
.
Shortly after VCAM1 induction, monocytes and
T cells enter the arterial intima (FIG. 2a). Under the influ-
ence of macrophage colony-stimulating factor (M-CSF)
produced by endothelial cells and smooth muscle cells
12
,
the monocytes differentiate into macrophages
13
(FIG. 2b)
and T cells can undergo antigen-dependent activation
(FIG. 2c; see later). Interestingly, VCAM1 expression by
the endothelium ceases after a few weeks, but smooth
muscle cells begin to express this adhesion molecule
14
.
Expression of VCAM1 and other adhesion molecules by
smooth muscle cells might promote the recruitment and
retention of mononuclear cells in the arterial intima.
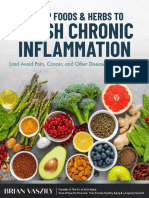
Figure 1 | Cellular composition of atherosclerotic plaques. The atherosclerotic plaque has a core containing lipids
(which include esterified cholesterol and cholesterol crystals) and debris from dead cells. Surrounding it, a fibrous cap
containing smooth muscle cells and collagen fibres stabilizes the plaque. Immune cells including macrophages, T cells
and mast cells populate the plaque, and are frequently in an activated state. They produce cytokines, proteases, pro-
thrombotic molecules and vasoactive substances, all of which can affect plaque inflammation and vascular function.
Until complications occur, an intact endothelium covers the plaque.
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 509
2006 Nature Publishing Group
Endothelial
cell
MHC class II
TCR
APC
Scavenger
receptor
VLA4
VCAM1
Blood-vessel
lumen
LDL
oxLDL
Monocyte
Macrophage Monocyte
Foam cell
Chemokine
receptor
Chemokine
M-CSF
T cell
TLR T cell Endothelial cell
LPS, HSP60
or oxLDL
Pro-inammatory cytokines
Proteases
Procoagulants
Pro-apoptotic factors
Increased adhesion molecules
Increased permeability
Increased propensity for
thrombus formation
Decreased collagen production
Decreased proliferation
CD4
+
T cell
T
H
1 cell
IL-12
IL-15
IL-18
b
c
oxLDL
T
H
1 cell
Smooth
muscle cell
MHC class II TCR
IFN
TNF
CD40L CD40
Macrophage
Proteases
Pro-inammatory
mediators
Decreased
inammation
T
H
1 cell
T
H
2 cell or
regulatory
T cell
Smooth
muscle cell
TGF
TGF
IL-10
e
Macrophage
a d
T cell Endothelial cell
T cell Endothelial cell
T cell Endothelial cell
Figure 2 | Recruitment and activation of immune cells in atherosclerotic plaques. a | Low-density lipoprotein (LDL)
diffuses from the blood into the innermost layer of the artery, where LDL particles can associate with proteoglycans of the
extracellular matrix. The LDL of this extracellular pool is modified by enzymes and oxygen radicals to form molecules such
as oxidized LDL (oxLDL). Biologically active lipids are released and induce endothelial cells to express leukocyte adhesion
molecules, such as vascular cell-adhesion molecule 1 (VCAM1). Monocytes and T cells bind to VCAM1-expressing
endothelial cells through very late antigen 4 (VLA4) and respond to locally produced chemokines by migrating into the
arterial tissue. b | Monocytes differentiate into macrophages in response to local macrophage colony-stimulating factor
(M-CSF) and other stimuli. Expression of many pattern-recognition receptors increases, including scavenger receptors
and Toll-like receptors (TLRs). Scavenger receptors mediate macrophage uptake of oxLDL particles, which leads to
intracellular cholesterol accumulation and the formation of foam cells. TLRs bind lipopolysaccharide (LPS), heat-shock
protein 60 (HSP60), oxLDL and other ligands, which instigates the production of many pro-inflammatory molecules by
macrophages. c | T cells undergo activation after interacting with antigen-presenting cells (APCs), such as macrophages
or dendritic cells, both of which process and present local antigens including oxLDL, HSP60 and possibly components
of local microorganisms. A T helper 1 (T
H
1)-cell-dominated response ensues, possibly owing to the local production of
interleukin-12 (IL-12), IL-18 and other cytokines. Antigen presentation and T
H
1-cell differentiation might also occur in
regional lymph nodes. d | T
H
1 cells produce inflammatory cytokines including interferon- (IFN ) and tumour-necrosis
factor (TNF) and express CD40 ligand (CD40L). These messengers prompt macrophage activation, production of
proteases and other pro-inflammatory mediators, activate endothelial cells, increase adhesion-molecule expression
and the propensity for thrombus formation, and inhibit smooth-muscle-cell proliferation and collagen production.
e | Plaque inflammation might be attenuated in response to the anti-inflammatory cytokines IL-10 and transforming
growth factor- (TGF), which are produced by several cell types including regulatory T cells, macrophages, and for TGF,
also vascular cells and platelets. TCR, T-cell receptor.
REVI EWS
510 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
Scavenger receptors
Cell-membrane proteins that
take up oxidatively or
otherwise modified low-density
lipoproteins.
Experiments using genetically altered mice show
that leukocyte adhesion molecules participate in the
initiation of atherosclerosis. Apoe
/
mice that are also
deficient for both endothelial-cell selectin (E-selectin)
and platelet selectin (P-selectin) have reduced severity
of atherosclerosis
15
. Similarly, Ldlr
/
mice that express
a truncated form of VCAM1 with impaired func-
tion develop less severe disease than those expressing
wild-type VCAM1 (REF. 16). Such studies use truncated
VCAM1 because complete VCAM1 deficiency is lethal
at the embryonic stage.
In addition to the expression of adhesion molecules,
several chemokines produced by vascular cells guide
the recruitment of immune cells (FIG. 2a). Data obtained
using knockout mice show a key role for CC-chemokine
ligand 2 (CCL2; also known as MCP1) and its receptor,
CC-chemokine receptor 2 (CCR2), in the initiation of
atherosclerosis
17,18
. Indeed, absence of CCL2 or CCR2
limits the entry of monocytes and T cells into the arte-
rial intima and inhibits atherogenesis. Macrophages
and vascular cells of the forming plaque also produce
the T-cell attractants CCL5 (also known as RANTES),
CXC-chemokine ligand 10 (CXCL10; also known as
IP10) and CXCL11 (also known as ITAC)
19
, the mast-
cell attractant CCL11 (also known as eotaxin)
20
and also
the Janus molecule CXCL16, which can function as both
a scavenger receptor and a chemokine
21
. Administration
of a blocking form of CCL5 attenuates atherogenesis
in mice
22
.
Atherosclerotic plaques in humans and mice also
express another chemokine, the cell-surface anchored
CX
3
-chemokine ligand 1 (CX
3
CL1; also known as
fractalkine), which is a transmembrane protein pref-
erentially expressed by smooth muscle cells. CX
3
CL1
that is shed by proteolysis can engage CX
3
-chemokine
receptor 1 (CX
3
CR1), which is expressed by monocytes
and macrophages. Ligation of CX
3
CR1 on blood-borne
monocytes stimulates their migration to the artery wall
and contributes to atherogenesis, as indicated by stud-
ies using mice deficient for both APOE and CX
3
CR1
(REFS 23,24).
Innate immunity and lipid accumulation
Monocyte-derived macrophages abound in plaques and
are outnumbered only by vascular smooth muscle cells
in some plaques. Several phenotypes of macrophage are
found in plaques, including inflammatory macrophages
and also foam cells, which develop when cholesteryl
esters accumulate in the cytosol of intimal macrophages
(FIG. 2b). Cholesterol derives from lipoproteins that have
undergone oxidation or enzymatic modification in the
tissue. This renders the lipoprotein particle amenable
to uptake by macrophages that express scavenger recep-
tors
25
, a family of proteins that includes CD36, CD68,
CXCL16, lectin-type oxidized low-density lipoprotein
receptor 1 (LOX1), scavenger receptor A (SR-A) and
SR-B1 . Scavenger receptors are pattern-recognition
receptors (PRRs) that mediate internalization and
lysosomal degradation of modified lipoprotein parti-
cles, lipopolysaccharide, fragments of malaria parasites
and apoptotic bodies
26
. Uptake by scavenger receptors
does not lead directly to inflammation but can lead to
MHC-class-II-restricted antigen presentation of inter-
nalized material, thereby linking innate and adaptive
immunity
27
.
Considering their role in the formation of foam
cells, one would expect scavenger receptors to have an
important, if not crucial, role in atherogenesis. However,
recent results showing increased, rather than decreased,
atherosclerosis in mice lacking CD36, CXCL16 or SR-A
have cast doubt on this conclusion
28
. This might be
because receptor-mediated internalization of modified
lipoproteins by macrophages can facilitate the eventual
elimination of these particles from plaques through
high-density-lipoprotein-dependent mechanisms
29
.
If, as a result of the absence of foam cells, this clear-
ance of modified lipoprotein did not occur, removal of
such lipids from plaques would be less efficient and the
accumulation of extracellular cholesterol in the lipid
pool might be more detrimental than the presence of
foam cells.
Whereas scavenger receptors mediate internaliza-
tion, degradation and antigen presentation of ligands,
Toll-like receptors (TLRs) can elicit inflammatory
responses directly
30
. The many TLR-family members
that can be detected in plaques are expressed mainly by
macrophages and endothelial cells
31
. By contrast, in the
normal artery wall, only TLR2 and TLR4 are expressed
by endothelial cells and the underlying smooth muscle
cells do not express TLRs. Therefore, plaque forma-
tion causes a considerable increase in the repertoire
of PRRs expressed by the artery wall. A broad range of
pathogen-associated molecular patterns can ligate the
different TLRs
30
. Among them, microbial components,
heat-shock proteins (HSPs) and unmethylated CpG
DNA might be directly relevant to athero genesis because
several microorganisms are associated with atheroscle-
rosis. In addition, some data indicate that endogenous
HSP60 and oxidized LDL (oxLDL) bind TLR4CD14
complexes and elicit inflammatory responses
3234
.
Following ligation, TLRs activate nuclear factor-B
(NF-B) and mitogen-activated protein kinase
activator protein 1 signalling pathways
30,32
. Direct
immuno histochemical analysis has shown that a large
proportion of the TLR4-expressing cells in human
plaques have nuclear translocation of NF-B, which is
consistent with a role for TLR4 ligation in inflammatory
activation in the plaques
31
. The response downstream
of TLR ligation in the plaque probably involves the
secretion of pro-inflammatory cytokines and matrix
metalloproteinases (MMPs), as well as the production
of low-molecular-weight inflammatory mediators such
as nitric oxide and endothelin-1 (REF. 30). Genetic defi-
ciency of TLR4 or its signal-transducing adaptor mol-
ecule myeloid differentiation primary-response gene 88
(MyD88) reduces plaques in mice
35,36
.
T cells promote atherogenesis
Human atherosclerotic plaques contain numerous
T cells. In a plaque, ~40% of the cells express macro-
phage markers, ~10% are CD3
+
T cells and most of the
remainder have the characteristics of smooth muscle
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 511
2006 Nature Publishing Group
Vasa vasorum
Small nutrient vessels in the
normal adventitia and outer
media of the artery wall,
which can also give rise to
microvessels in the plaque.
cells
2
. Small populations of mast cells, B cells and DCs
occur in plaques and, together with T cells, monocytes
and macrophages, might traffic between the blood in
the arterial lumina, the lesioned artery wall, the vasa
vasorum microvessels that penetrate the artery and
the regional lymph nodes.
The ratio of CD4
+
to CD8
+
T cells in advanced
plaques resembles that found in peripheral blood
2
. Most
T cells are T cells, but there is also a small propor-
tion of T cells. Lesions of early stages of experimental
atherosclerosis contain oligoclonal expansions of CD4
+
cells expressing an T-cell receptor (TCR)
37
, indi-
cating activation in response to a limited set of local
antigens (FIG. 2c). The CD4
+
T cells that are isolated
from human plaques are mostly CD45RO-expressing
memory and/or effector T cells
38
. An initial round of
T-cell activation in response to athero-antigens might
occur in the regional lymph nodes, possibly after anti-
gen presentation by DCs trafficking from the plaque
to the lymph node
39
. After entering the blood, previ-
ously activated memory and/or effector T cells bind
cell-surface adhesion molecules that are expressed by
endothelial cells at the plaque surface and/or in the vasa
vasorum, and then enter the plaque. Macrophages in
the plaque expressing MHC class II molecules might
then present antigen to these T cells, leading to further
rounds of activation.
Very recently, Ath1, which is an atherosclerosis sus-
ceptibility locus on mouse chromosome 1, was mapped
to the gene encoding OX40 ligand (OX40L; also known
as TNFSF4), which is a co-stimulatory factor for T-cell
activation
40
. Reduced expression of this protein was asso-
ciated with reduced atherosclerosis in inbred strains that
differ in their Tnfsf4 alleles and also in mice carrying a
targeted deletion of this gene
40
. Polymorphisms in human
TNFSF4 were found to be associated with coronary
atherosclerosis and with an increased risk for myocar-
dial infarction in a human genetic epidemiology study
40
.
These data re-emphasize the importance of immune
activation in atherosclerosis and its complications
41
.
Plaque antigens activate local cellular adaptive immu-
nity. Cloning T cells from surgically removed human
plaques has identified several cell-mediated, local adap-
tive immune reactions. CD4
+
T-cell clones derived from
plaques recognize oxLDL, with other clones recognizing
HSP60 or other antigens derived from certain pathogenic
microorganisms, such as Chlamydia pneumoniae
42,43
(FIG. 2c). In all of these cases, antigen recognition was
restricted by HLA-DR and involved TCR
+
CD4
+
T cells
42,44,45
.
Antigen-presenting cells selectively internalize
oxLDL particles through the scavenger-receptor path-
way. After proteolytic processing, fragments of the
protein component of LDL, APOB, bind nascent MHC
class II molecules and traffic to the cell surface. Indeed,
APOB fragments are among the peptides displayed most
frequently by HLA-DR molecules in cultured human
lymphoblastoid cells
46
. Therefore, receptor-mediated
endocytosis and the antigen-presentation pathway facili-
tate MHC class II presentation of LDL-derived peptides
to CD4
+
T cells. As expected, no T cells react with native
LDL components. However, oxidative modification
of LDL breaks tolerance and oxLDL-reactive T cells local-
ize in plaques, lymph nodes, and in the blood of patients
with atherosclerosis and experimental animals
42,47
.
OxLDL-reactive CD4
+
T cells probably recognize
APOB-derived oligopeptides carrying adducts formed
during oxidation
48
; whereas oxLDL-specific antibodies
react with oxidized phospholipids such as phosphoryl-
choline
49,50
, as well as aldehyde-peptide epitopes including
malondialdehyde-lysine
42,44,45
.
Most oxLDL-reactive CD4
+
T cells have a T helper 1
(T
H
1)-cell phenotype
42,47
. Because T
H
1 cytokines (such as
IFN) generally stimulate pro-atherosclerotic processes
(see later), these T cells probably promote atherogenesis,
a conclusion supported by adoptive-transfer studies in
severe combined immunodeficient (SCID) mice lack-
ing APOE
51
. As expected, these mice show substantially
reduced atherosclerotic plaques compared with immuno-
competent Apoe
/
mice. Transfer of CD4
+
T cells from
immunocompetent Apoe
/
mice to SCID mice lacking
ApoE increases the atherogenesis found in immuno-
deficient mice, to almost the same level as that found
in fully immunocompetent Apoe
/
mice. Therefore, the
net effect of CD4
+
T cells is to increase atherogenesis in
mice susceptible to atherosclerotic disease. Obviously,
this finding does not preclude the existence of T-cell
subsets that might mitigate disease.
Recent studies have identified transcripts encoding
V14J281-containing TCR -chains in plaques of
hypercholesterolaemic mice, indicating the presence
of NKT cells
52
. The abundance of CD1 molecules in
plaques
53
indicates that CD1-mediated NKT-cell acti-
vation takes place, but the absence of specific markers
for NKT cells has hampered direct immunohistological
demonstration of NKT cells in plaques. However, admin-
istration of ligands that specifically activate NKT cells to
Apoe
/
mice shows that NKT-cell activation increases
early atherosclerotic plaque development concomitantly
with increased local expression of pro-inflammatory
cytokines, whereas abrogation of CD1-mediated antigen
presentation reduces disease
52,54
. Therefore, NKT cells
contribute to atherosclerosis, probably by antigen-
specific activation in response to lipid antigens present
in plaques.
A role for T
H
1/T
H
2-cytokine balance? Analyses of
cell-surface-marker expression and cytokine secretion
indicate activation of a remarkably large proportion
of T cells in plaques
38
. T
H
1-type cytokines dominate
in mouse models of atherosclerosis and in human
plaques. For example, human plaques contain cells
producing IFN, interleukin-12 (IL-12), IL-15, IL-18
and TNF, but few cells producing the T
H
2-type cytokine
IL-4 (REFS 42,55,56). Together with the histopatho-
logical features of accumulation of macrophages and
T cells, the predominance of T
H
1-type cytokines indi-
cates that atherosclerosis is a T
H
1-cell-driven disease
(FIG. 2d). This hypothesis is supported by studies in
genetically altered mice that show that there is reduced
atherosclerosis in hypercholesterolaemic mice lacking
REVI EWS
512 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
Tissue factor
A procoagulant that stimulates
thrombus formation, when in
contact with blood, by
accelerating the action of
factors VIIa and Xa.
IFN or its receptor
57,58
, IL-12 (REF. 59), IL-18 (REF. 60),
TNF
61
or the T
H
1-cell-inducing transcription factor
T-bet
62
. Administration of recombinant IFN
63
or
the T
H
1-cell-inhibiting drug pentoxifyllin
64
to hyper-
cholesterolaemic mice led to increased and decreased
atherosclerosis, respectively, lending further support
to this hypothesis
64
.
If T
H
1 cytokines stimulate plaque formation and
T
H
2 cytokines inhibit T
H
1-cell responses, can T
H
2-cell
responses protect against atherosclerosis? In support
of this proposition, C57BL/6 mice (which are prone
to T
H
1-type immune responses) develop fatty streaks
if fed a high-cholesterol diet, whereas BALB/c mice
(which are prone to T
H
2-type immune responses)
are resistant to atherogenesis
65,66
. Targeted deletion
of the gene encoding signal transducer and activa-
tor of transcription 6 (STAT6), a transcription factor
that is essential for the differentiation of T
H
2 cells,
renders BALB/c mice susceptible to atherogenesis and
this occurs in parallel with a switch from T
H
2-cell to
T
H
1-cell responses
66
.
Although these studies of the development of
fatty streaks indicate opposing roles for T
H
1 and T
H
2
cells in disease development, mice that develop more
advanced plaques show a more complicated picture.
Pharmacological inhibition of T
H
1 cells using pentoxi-
fyllin or IL-18-binding protein inhibits atherosclerosis
in Apoe
/
mice
64,67
, and administration of recombinant
T
H
1 cytokines (recombinant IL-18 and IFN) exacer-
bates disease
63,68
. However, data for IL-4, which is
the prototypic T
H
2 cytokine, are inconclusive. Some
studies have shown that IL-4 has a protective effect,
whereas others found reduced disease in the absence
of IL-4 (REFS 59,69). These divergent findings, under
different experimental conditions, might reflect the
complex range of biological activities found for IL-4,
including stimulation of scavenger-receptor expres-
sion and the induction of elastin degrading MMP12,
which can lead to aneurysm formation
70
. Defining the
role of T
H
2 cells in atherosclerosis, therefore, requires
further study.
Pro-atherosclerotic action of T
H
1 cells. How can T
H
1
cells promote disease development? IL-12 and IL-18,
which are produced by macrophages and smooth mus-
cle cells in plaques, can indirectly affect the develop-
ment of plaques by promoting T
H
1-cell differentiation.
By contrast, IFN and TNF directly accelerate disease
through their actions on macrophages and vascular
cells (FIG. 2c,d). IFN activates macrophages, thereby
increasing their production of nitric oxide, pro-inflam-
matory cytokines, and pro-thrombotic and vasoactive
mediators. Additionally, IFN inhibits endothelial-cell
proliferation
71
, the proliferation and differentiation
of vascular smooth muscle cells
72
, and also decreases
collagen production by these smooth muscle cells
73
.
Decreasing the cell and collagen content of the fibrous
cap might reduce the stability of the plaque. Therefore,
the combined effects of IFN on cells of the forming
plaque promote inflammation and extracellular-matrix
destabilization.
The pro-inflammatory cytokine TNF triggers vascu-
lar inflammation through the NF-B pathway, inducing
the production of reactive oxygen and nitrogen species,
proteolytic enzymes and pro-thrombotic tissue factor by
endothelial cells, and modulates the fibrinolytic capacity
of the cells
7476
. TNF also has profound metabolic effects
that include the suppression of lipoprotein lipase, which
leads to the accumulation of triglyceride-rich lipopro-
teins in the blood. Such lipoproteins, and the TNF levels,
have been associated with heart disease in clinical stud-
ies
7779
. Genetic loss-of-function studies also support the
idea that TNF has a pro-atherogenic role
61
.
CD40 and CD40L: a co-stimulatory dyad with pro-
atherogenic action. The cell-surface proteins CD40 and
CD40 ligand (CD40L; also known as CD154) have sev-
eral similarities to soluble pro-inflammatory cytokines.
CD40 ligation on cells found in plaques triggers an
inflammatory response similar to that elicited by TNF,
that is, secretion of other cytokines and MMPs, and
expression of adhesion molecules
80
. Importantly, CD40
ligation causes expression of the procoagulant tissue
factor by human macrophages, something that soluble
pro-inflammatory cytokines do not do. Macrophages and
T cells express CD40 and CD40L, as do vascular endothe-
lial cells, smooth muscle cells and platelets
81,82
. Therefore,
CD40 ligation propagates inflammatory activation in all
the main cell types involved in atherogenesis. Inhibition
of CD40 ligation and inactivation of the gene encoding
CD40L reduces atherosclerotic plaques in hypercholes-
terolaemic mice
83,84
. Unfortunately, CD40 blockade in
humans can promote platelet aggregation and thrombosis,
which is an obstacle to its clinical application.
Anti-atherogenic immunity
Anti-inflammatory cytokines. Although local cellular
immunity predominantly promotes atherosclerosis
through the action of cell-surface molecules (such as
CD40CD40L) and cytokines (such as IFN and TNF),
counterbalancing factors can function to dampen dis-
ease activity (FIG. 2e). Two anti-inflammatory cytokines,
IL-10 and transforming growth factor- (TGF), provide
particularly important atheroprotective signals.
Two groups have reported previously that IL-10-
deficient C57BL/6 mice that consume a fatty diet develop
an increased quantity of fatty streaks compared with
wild-type mice
85,86
. By contrast, Il10 transgenic C57BL/6
mice do not develop fatty streaks, thereby providing evi-
dence of a protective role for IL-10 in athero sclerosis
85,86
.
The mouse model used in these early studies mimicked
the initial stage of atherogenesis, but the mice did
not develop lesions similar to human clinical disease.
However, subsequent experiments using Apoe
/
mice,
which develop atherosclerotic lesions that are more simi-
lar to those found in humans, also show an atheroprotec-
tive role for IL-10 (REF. 87). Interestingly, IL-10 promotes
arteriopathy in transplanted hearts, indicating a more
complex picture.
The pluripotent cytokine TGF has many effects on a
diverse range of cell types and can inhibit atherosclerosis
at least as well as IL-10. For example, TGF promotes
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 513
2006 Nature Publishing Group
collagen production, which could increase plaque
stability. Treatment with tamoxifen, which is a TGF-
stimulating oestrogen-receptor agonist, reduces the
formation of fatty streaks in C57BL/6 mice fed with
fat
88
, whereas administration of TGF-specific block-
ing antibodies or decoy receptors for TGF reduces
atherosclerotic plaque formation in Ldlr
/
mice
89,90
.
However, these studies did not identify the mechanism
of action of TGF.
Two more-recent studies show that TGF exerts its
atheroprotective effects by modulating T-cell activation.
In the first study, crossbreeding mice carrying dominant-
negative TGF receptors (that were expressed under
the control of the Cd4 promoter) with Apoe
/
mice
led to a fivefold increase in plaque size and advanced
plaques were found in the proximal aorta of 12-week-
old crossbred mice
91
. Notably, the plaques showed signs
of increased inflammation and had fewer interstitial
collagen fibres, a characteristic of human plaques that
cause thrombosis (see later). In the second study, bone
marrow from mice that expressed a dominant-negative
form of the type II TGF receptor (that was expressed
under the control of the Cd2 promoter) was transplanted
to irradiated Ldlr
/
mice
92
. Again, plaques showed signs
of substantial inflammation and a poorly developed
collagenous matrix. These studies show the important
atheroprotective effects of TGF that occur through the
dampening of T-cell activity.
Several cell types can produce TGF and IL-10,
including platelets, macrophages, endothelial cells,
smooth muscle cells and regulatory T cells. Activation
of regulatory T cells could therefore offer a means of
antigen-specific atheroprotection (FIG. 2e). A recent study
supports this idea by showing that the transfer of natural
CD4
+
CD25
+
regulatory T (T
Reg
) cells reduces athero-
sclerosis, whereas depletion of CD25
+
cells increases dis-
ease in Apoe
/
mice
93
. Depletion of CD25
+
cells in mice
lacking functional TGF receptors on T cells did not alter
plaque size, indicating that this cytokine mediates the
atheroprotective effect of regulatory T cells
93
.
Humoral immunity. In addition to innate immunity
and T cells, antibodies with different specificities can
participate in atherosclerosis. Humans and experimen-
tal animals with disease have antibodies specific for
oxLDL particles
44
. B-cell epitopes in oxLDL include
amino-acid residues of APOB that are modified by
lipid peroxidation products, such as malondialdehyde
and 4-hydroxynonenal. Although some clinical and epi-
demiological studies have found positive correlations
between the presence of antibodies specific for oxLDL
and the progression of atherosclerosis
94,95
, other studies
have not detected any correlation. Interestingly, anti-
bodies specific for oxLDL, mainly of the IgM isotype,
also circulate in asymptomatic humans
96
and cross react
with apoptotic bodies
49
. These antibodies bind the
oxidized phospholipids in oxLDL and also recognize
phosphorylcholine in the cell wall of Streptococcus
pneumoniae
49
. Phosphorylcholine-specific IgM con-
sists of germline-encoded antibodies of the T15 type
that are produced by B1 cells
49
. Therefore, expansion
of B-cell clones that produce T15-type antibodies, for
example during a pneumococcal infection, might affect
the development of plaques. Indeed, immunization of
Ldlr
/
mice with a pneumococcal vaccine reduced the
extent of atherosclerosis
50
.
Molecular mimicry could explain the crossreactiv-
ity between the humoral immune responses to oxLDL,
apoptotic bodies and pneumococci. This mechanism
might also apply to HSP60, another antigen associated
with atherosclerosis
97
. HSP60 is a chaperone molecule
that is involved in protein folding and can be detected
in plaques. Antibodies specific for HSP60 are found in
experimental animals that have atherosclerosis and have
been correlated with disease progression in a human
cohort study
98
. Present in prokaryotes and eukaryotes,
HSP60 has shown remarkable sequence conservation dur-
ing evolution. As antibodies specific for HSP60 crossreact
between microbial and eukaryotic HSP60, antibodies
that react to human HSP60 can be generated in response
to infection with microbes that express HSP60, such as
C. pneumoniae
99
.
Several further experimental, and some human, stud-
ies show that humoral immunity can protect against
atherosclerosis. Splenectomy increases atherosclerosis in
both Apoe
/
mice and humans
100
. In Apoe
/
mice, trans-
fer of splenic B cells from atherosclerotic animals into
splenectomized recipients protects against disease, pos-
sibly because of the production of protective antibodies
by B cells
100
.
Immunization experiments identify oxLDL and
HSP60 as important antigens that can induce protective,
as well as detrimental, immune responses (TABLE 1; see
also later). A tentative conclusion from these studies is that
T
H
1-type immune responses promote disease; whereas
humoral immunity has protective effects, possibly by
eliminating antigens before they reach plaques.
Adaptive immunity disrupts plaques
In general, the gravest clinical complications of athero-
sclerosis result from the sudden thrombotic occlusion of
an artery
101
. The sudden onset of myocardial infarction,
as well as many strokes and episodes of acute limb ischae-
mia, is caused by thrombi that arise from atherosclerotic
plaques that do not necessarily tightly narrow the artery.
Therefore, many episodes of damage to the heart muscle,
brain or lower extremities can occur without warning, all
too often with devastating consequences.
Physical disruption of a plaque is the most frequent
cause of thrombotic occlusions. Indeed, the most fre-
quent patho-anatomical substrate for sudden coronary
thrombosis is rupture of the fibrous cap that overlies the
lipid core of the plaque
101
(FIG. 3). Fibres of interstitial col-
lagens (types I and III) normally confer biomechanical
stability on the fibrous cap of the plaque. As discussed
earlier, the T
H
1-cytokine IFN strongly inhibits the
production of interstitial collagens by vascular smooth
muscle cells, which are the main source in the arterial
wall of this extracellular-matrix macromolecule
73
. IFN
can also inhibit the proliferation of smooth muscle
cells, thereby reducing the stabilizing and collagen-
synthesizing cellular component of the plaque
72
. Also,
REVI EWS
514 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
Angina pectoris
A reversible attack of chest
discomfort, usually caused by
an imbalance between the
oxygen demand of the working
heart muscle and the
insufficient supply through
narrow, atherosclerotic
coronary arteries.
Angioplasty
A percutaneous catheter
procedure that inflates a
balloon in areas of narrowing
(stenosis) in arteries.
Statins
A class of drugs that inhibit the
rate-limiting enzyme (3-
hydroxy-3-methylglutaryl
coenzyme A reductase) in the
pathway of cholesterol
biosynthesis.
proteases elaborated mainly from activated macrophages
in plaques can degrade collagen
102,103
. In addition, liga-
tion of CD40 expressed by macrophages increases the
production of matrix-degrading proteases that include
the interstitial collagenases of the MMP family, MMP1,
MMP8 and MMP13 (REF. 104). Therefore, T
H
1 cells
probably have an essential role in regulating the func-
tions of smooth muscle cells (collagen-fibre formation)
and macrophages (collagen degradation) that crucially
regulate the integrity of the fibrous cap of the plaque
and therefore its susceptibility to rupture and provoke
thrombosis.
Once coagulation factors in the blood gain access
to the lipid core of the plaque following rupture of the
fibrous cap, thrombosis commonly ensues. Tissue factor,
the potent procoagulant expressed by a subpopulation
of macrophages in the lipid core of the plaque, triggers
these thromboses
101
. As noted earlier, ligation of CD40
expressed by macrophages strongly induces expression
of tissue factor
80
. Indeed, T cells expressing CD40L local-
ize in the vicinity of macrophages that are expressing tis-
sue factor in the lipid core of human plaques
105
. Because
platelets can also express CD40L
82
when activated, positive
feedback can amplify the local inflammatory response,
once a thrombus begins to form, because of generation of
the protease thrombin induced by tissue factor and plate-
let activation induced by thrombin. Therefore, although
T cells could orchestrate the pathophysiology of plaque
disruption, dysregulated antigen-nonspecific pathways
probably amplify and sustain the formation of thrombi.
Modulation of immunity in atherosclerosis
Immunopharmacological intervention against sympto-
matic atherosclerosis. Although thrombi cause most of
the acute complications of atherosclerosis, the gradual
formation of stenoses that impede blood flow causes
many of the chronic symptoms of atherosclerotic disease,
such as angina pectoris (chest discomfort precipitated
typically by physical or emotional stress). Recent decades
have witnessed important advances in the ability of inter-
ventions, particularly percutaneous procedures, to relieve
stenoses and reduce ischaemia. Until recently, however,
the long-term success of mechanical procedures, such
as the deployment of arterial stents (metal scaffolds to
hold arteries open) and balloon angioplasty (inflation
of miniature balloons in blocked segments of arter-
ies to expand the arterial lumen), has been limited
by re-growth of intimal tissue which is known as
in-stent stenosis and restenosis, respectively. This
fibro-proliferative response of the injured artery can
re-occlude the lumen within months in a substantial
minority of patients.
Recently, the coating of stents with immunosup-
pressive agents, for example sirolimus (Rapamycin),
has shown striking effectiveness at reducing in-stent
stenosis
106
. This advance has markedly improved clinical
outcomes in patients undergoing percutaneous interven-
tion. Early preclinical studies provided the experimental
basis for this important therapeutic advance by show-
ing that another immunosuppressant, cyclosporin,
reduces intimal-cell proliferation in response to arterial
injury
107
.
The use of statins has shown striking clinical benefit
in preventing atherosclerotic complications during the
past decade. Numerous clinical trials have established
that 3-hydroxy-3-methylglutaryl coenzyme A (HMG-
CoA) reductase inhibitors (drugs of the statin family)
can reduce various atherosclerotic complications
108
.
The lowering of LDL cholesterol concentrations in the
blood doubtless accounts for much of this remarkable
clinical benefit. However, recent data indicate that part
of the clinical benefit of statins occurs because of an
anti-inflammatory effect that is apparently not related
to LDL reduction
109
. (See REF. 110 for a detailed discus-
sion of non-LDL-lowering effects of statins).
By blocking HMG-CoA reductase, statins prevent
the formation of lipids that control the function of
several intracellular proteins
111
. By acting on the MHC
class II transactivator (CIITA), statins can interfere with
the transcriptional induction of MHC class II mol-
ecules, which would decrease immune activation in the
plaque
112
. Statins can also limit the accelerated arterio-
sclerosis (sclerosis of the arterial walls) that complicates
solid-organ transplantation, a disease that often occurs
in the absence of increased concentrations of LDL
113
.
They also seem to reduce disease activity in patients with
rheumatoid arthritis
114
and in mice with experimental
autoimmune encephalomyelitis
115
. All these results lend
Table 1 | Immunization against atherosclerosis in experimental models
Antigen Route Animal model Effect on atherosclerosis References
MDA-LDL Subcutaneous WHHL rabbits Reduced 124
oxLDL Subcutaneous Fat-fed NZW rabbits Reduced 125
MDA-LDL Subcutaneous Apoe
/
mice Reduced 47,126
MDA-LDL Subcutaneous Ldlr
/
mice Reduced 127
APOB-peptides Subcutaneous Apoe
/
mice Reduced 95,128
MDA-LDL Subcutaneous Cd4
/
Apoe
/
mice Reduced 129
HSP65 Subcutaneous Ldlr
/
mice Increased 130
HSP65 Peroral/nasal Ldlr
/
mice Reduced 131,132
2-GPI Subcutaneous Ldlr
/
mice Increased 133
APO, apolipoprotein; GPI, glycoprotein I; HSP65, heat-shock protein 65; LDL, low-density lipoprotein; LDLR, LDL receptor; MDA-LDL,
malondialdehyde-modified LDL; NZW, New Zealand white; oxLDL, oxidized LDL; WHHL, Watanabe hereditably hyperlipidaemic.
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 515
2006 Nature Publishing Group
Blood-vessel lumen
Endothelial cell
Elastic
lamina
Cellular debris
and cholesterol
Rupture
Thrombus
Platelet
Erythrocyte
Fibrin
Foam cell T cell Macrophage Mast cell Monocyte Cholesterol Dendritic cell Dead cell
Smooth
muscle cell
Peroxisome-proliferator-
activated receptors
Nuclear receptors that
participate in the regulation
of cellular metabolism and
differentiation.
Thiazolidinedione
A class of medication, used
to treat diabetes, that binds
peroxisome-proliferator-
activated receptor-.
support to the idea that the immunomodulatory actions
of statins also contribute to their effects in patients with
atherosclerosis.
Recent studies have established that another category
of anti-atherosclerotic drugs, the ligands for a group of
nuclear transcription factors known as peroxisome-
proliferator-activated receptors (PPARs), can inhibit T-cell
activation in vitro. Activators of both PPAR (members
of the fibrate class of drugs) and PPAR (members of
the thiazolidinedione family of drugs) can reduce T-cell
activation, as was shown by decreased production of
IFN, TNF and IL-2 (REF. 116). PPAR agonists also
inhibit inflammatory activation of vascular smooth
muscle cells
117
. Therefore, activation of PPAR or PPAR
might also affect atherosclerosis in a beneficial manner
by blunting the adaptive and innate immune responses.
Nonspecific anti-inflammatory therapies, such as
non-steroidal anti-inflammatory drugs (NSAIDs), have
not improved the cardiovascular outcome. Indeed, treat-
ment with NSAIDs selective for cyclooxygenase-2 seems
to increase the risk of thrombotic complications
118,119
.
Despite their marked anti-inflammatory properties,
gluco corticosteroids themselves probably increase,
rather than decrease, atherogenesis, as chronic admin-
istration of these agents adversely affects plasma lipopro-
teins, promotes insulin resistance and sodium retention,
Figure 3 | Plaque activation, rupture and thrombosis. When activated, immune cells including macrophages, T cells
and mast cells can release pro-inflammatory cytokines, which reduce collagen formation and induce the expression of
tissue factor. Proteases that attack the collagenous cap are also released by activated immune cells. The weakened plaque
might fissure when subjected to the forces of arterial blood pressure. Exposure of subendothelial structures and
procoagulants such as tissue factor promotes platelet aggregation and thrombosis. A thrombus forms and might occlude
the lumen of the artery, leading to acute ischaemia.
REVI EWS
516 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
C-reactive protein
An acute-phase reactant
protein, the plasma
concentration of which
increases in inflammatory
states.
and inhibits collagen and elastin formation. It therefore
does not offer a reasonable therapeutic alternative in the
chronic phases of atherosclerosis.
Vaccination against atherosclerosis? Parenteral immu-
nization with malondialdehyde-modified LDL (that
is, LDL with a defined oxidative modification) or
malondialdehyde-modified peptides derived from the
LDL protein apolipoprotein inhibits atherosclerosis and
this occurs in parallel with increased titres of antibody
specific for the immunogen (TABLE 1). Interestingly, pro-
tection through this route does not require CD4
+
T-cell
help
120
. Therefore, protection seems to depend mostly
on humoral immunity, at least in this model.
By contrast, the outcomes after immunization with
HSP60 or its mycobacterial homologue HSP65 are
complex (TABLE 1). Parenteral immunization in C57BL/6
mice fed with fat, as well as Ldlr
/
mice, aggravates
disease, whereas oral or nasal immunization elicits
protective immunity. Induction of mucosal immunity
involves activation of regulatory T cells that produce
anti-inflammatory cytokines and also high titres of
specific antibodies. Therefore, the precise mechanism
by which mucosal immunization leads to reduced
atherosclerosis remains to be clarified.
Although several questions remain, the immuniza-
tion experiments with malondialdehyde-modified LDL
and HSP60 indicate that it is possible that a vaccina-
tion strategy might protect against atherosclerosis and
its complications. Obviously, many obstacles remain,
rendering the success of this approach unpredictable,
particularly in humans.
Conclusion
The evidence reviewed in this article supports the
involvement of the immune response in atherosclerosis
from its initiation through to its thrombotic complica-
tions. The concept that adaptive immunity pivotally
regulates atherogenesis has already been clinically useful.
Markers of the acute-phase response, notably C-reactive
protein (CRP), predict the prognosis of patients who
have already sustained a cardiovascular event
121
. Lesser
elevations of CRP concentration, measured with a highly
sensitive assay and previously considered in the normal
range, can be used to predict cardiovascular events in
apparently well populations
109,122,123
. Markers of height-
ened innate immune responses, such as CRP, correlate
with worse outcomes in individuals with acute coronary
syndromes
121
.
Systemic administration of non-selective immuno-
suppressive drugs will probably not be useful for the
treatment of atherosclerosis, at least during its long
asymptomatic phase, because of the need for prolonged
therapy and the potential toxicities of such treatments.
However, the immune system in its full complexity offers
much more subtle targets for therapeutic manipulation.
As more details emerge of the specific pathways involved
in the immune response and the inflammation that
occur in atherosclerosis, more selective interventions
might prove appropriate for long-term anti-atheroscle-
rotic therapy. Also, as our ability to gauge the risk of
acute complications improves, we might be able to target
in a much more selective manner those therapies that
would otherwise impair host defences if administered
on a long-term basis.
1. Murray, C. J. & Lopez, A. D. Global mortality,
disability, and the contribution of risk factors: global
burden of disease study. Lancet 349, 14361442
(1997).
2. Jonasson, L., Holm, J., Skalli, O., Bondjers, G. &
Hansson, G. K. Regional accumulations of T cells,
macrophages, and smooth muscle cells in the human
atherosclerotic plaque. Arteriosclerosis 6, 131138
(1986).
3. Bobryshev, Y. V. & Lord, R. S. A. S-100 positive cells
in human arterial intima and in atherosclerotic lesions.
Cardiovas. Res. 29, 689696 (1995).
4. Kovanen, P. T., Kaartinen, M. & Paavonen, T.
Infiltrates of activated mast cells at the site of coronary
atheromatous erosion or rupture in myocardial
infarction. Circulation 92, 10841088 (1995).
5. Jonasson, L., Holm, J., Skalli, O., Gabbiani, G. &
Hansson, G. K. Expression of class II transplantation
antigen on vascular smooth muscle cells in human
atherosclerosis. J. Clin. Invest. 76, 125131 (1985).
6. Plump, A. S. et al. Severe hypercholesterolemia and
atherosclerosis in apolipoprotein E-deficient mice
created by homologous recombination in ES cells.
Cell 71, 343353 (1992).
7. Piedrahita, J. A., Zhang, S. H., Hagaman, J. R.,
Oliver, P. M. & Maeda, N. Generation of mice carrying
a mutant apolipoprotein E gene inactivated by gene
targeting in embryonic stem cells. Proc. Natl Acad.
Sci. USA 89, 44714475 (1992).
8. Ishibashi, S., Goldstein, J. L., Brown, M. S.,
Herz, J. & Burns, D. K. Massive xanthomatosis
and atherosclerosis in cholesterol-fed low density
lipoprotein receptor-negative mice. J. Clin. Invest.
93, 18851893 (1994).
9. Cybulsky, M. I. & Gimbrone, M. A. Endothelial
expression of a mononuclear leukocyte adhesion
molecule during atherosclerosis. Science 251,
788791 (1991).
10. Nakashima, Y., Raines, E. W., Plump, A. S.,
Breslow, J. L. & Ross, R. Upregulation of VCAM-1
and ICAM-1 at atherosclerosis-prone sites on the
endothelium in the apoE-deficient mouse.
Arterioscler. Thromb. Vasc. Biol. 18, 842851
(1998).
11. Dai, G. et al. Distinct endothelial phenotypes
evoked by arterial waveforms derived from
atherosclerosis-susceptible and-resistant regions
of human vasculature. Proc. Natl Acad. Sci. USA
101, 1487114876 (2004).
12. Rajavashisth, T. B. et al. Induction of endothelial
cell expression of granulocyte and macrophage
colony-stimulating factors by modified low-density
lipoproteins. Nature 344, 254257 (1990).
13. Smith, J. D. et al. Decreased atherosclerosis in mice
deficient in both macrophage colony-stimulating factor
(op) and apolipoprotein E. Proc. Natl Acad. Sci. USA
92, 82648268 (1995).
14. Li, H., Cybulsky, M. I., Gimbrone, M. A. &
Libby, P. Inducible expression of vascular cell
adhesion molecule-1 by vascular smooth muscle cells
in vitro and within rabbit atheroma. Am. J. Pathol.
143, 15511559 (1993).
15. Dong, Z. M. et al. The combined role of P- and
E-selectins in atherosclerosis. J. Clin. Invest.
102, 145152 (1998).
16. Cybulsky, M. I. et al. A major role for VCAM-1,
but not ICAM-1, in early atherosclerosis.
J. Clin. Invest. 107, 12551262 (2001).
17. Boring, L., Gosling, J., Cleary, M. & Charo, I. F.
Decreased lesion formation in CCR2
/
mice reveals a
role for chemokines in the initiation of atherosclerosis.
Nature 394, 894897 (1998).
18. Gu, L. et al. Absence of monocyte chemoattractant
protein-1 reduces atherosclerosis in low density
lipoprotein receptor-deficient mice. Mol. Cell
2, 275281 (1998).
19. Mach, F. et al. Differential expression of three
T lymphocyte-activating CXC chemokines by
human atheroma-associated cells. J. Clin. Invest.
104, 10411050 (1999).
20. Haley, K. J. et al. Overexpression of eotaxin and
the CCR3 receptor in human atherosclerosis: using
genomic technology to identify a potential novel
pathway of vascular inflammation. Circulation
102, 21852189 (2000).
21. Minami, M. et al. Expression of SR-PSOX, a novel
cell-surface scavenger receptor for phosphatidylserine
and oxidized LDL in human atherosclerotic lesions.
Arterioscler. Thromb. Vasc. Biol. 21, 17961800
(2001).
22. Veillard, N. R. et al. Antagonism of RANTES receptors
reduces atherosclerotic plaque formation in mice.
Circ. Res. 94, 253261 (2004).
23. Combadiere, C. et al. Decreased atherosclerotic
lesion formation in CX3CR1/apolipoprotein E double
knockout mice. Circulation 107, 10091016
(2003).
24. Lesnik, P., Haskell, C. A. & Charo, I. F. Decreased
atherosclerosis in CX3CR1
/
mice reveals a role
for fractalkine in atherogenesis. J. Clin. Invest.
111, 333340 (2003).
25. Steinberg, D. Low density lipoprotein oxidation
and its pathobiological significance. J. Biol. Chem.
272, 2096320966 (1997).
26. Peiser, L., Mukhopadhyay, S. & Gordon, S. Scavenger
receptors in innate immunity. Curr. Opin. Immunol.
14, 123128 (2002).
27. Nicoletti, A. et al. The macrophage scavenger
receptor type A directs modified proteins to antigen
presentation. Eur. J. Immunol. 29, 512521 (1999).
28. Moore, K. J. et al. Loss of receptor-mediated lipid
uptake via scavenger receptor A or CD36 pathways
does not ameliorate atherosclerosis in hyperlipidemic
mice. J. Clin. Invest. 115, 21922201 (2005).
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 517
2006 Nature Publishing Group
29. Bodzioch, M. et al. The gene encoding ATP-binding
cassette transporter 1 is mutated in Tangier disease.
Nature Genet. 22, 347351 (1999).
30. Janeway, C. A. Jr & Medzhitov, R. Innate immune
recognition. Annu. Rev. Immunol. 20, 197216
(2002).
31. Edfeldt, K., Swedenborg, J., Hansson, G. K. &
Yan, Z. Q. Expression of toll-like receptors in human
atherosclerotic lesions: a possible pathway for plaque
activation. Circulation 105, 11581161 (2002).
32. Kol, A., Lichtman, A. H., Finberg, R. W., Libby, P. &
Kurt-Jones, E. A. Cutting edge: heat shock protein
(HSP) 60 activates the innate immune response:
CD14 is an essential receptor for HSP60 activation
of mononuclear cells. J. Immunol. 164, 1317
(2000).
33. Xu, X. H. et al. Toll-like receptor-4 is expressed
by macrophages in murine and human lipid-rich
atherosclerotic plaques and upregulated by oxidized
LDL. Circulation 104, 31033108 (2001).
34. Miller, Y. I. et al. Minimally modified LDL binds to
CD14, induces macrophage spreading via TLR4/
MD-2, and inhibits phagocytosis of apoptotic cells.
J. Biol. Chem. 278, 15611568 (2003).
35. Michelsen, K. S. et al. Lack of Toll-like receptor 4
or myeloid differentiation factor 88 reduces
atherosclerosis and alters plaque phenotype in mice
deficient in apolipoprotein E. Proc. Natl Acad. Sci.
USA 101, 1067910684 (2004).
36. Bjorkbacka, H. et al. Reduced atherosclerosis in
MyD88-null mice links elevated serum cholesterol
levels to activation of innate immunity signaling
pathways. Nature Med. 10, 416421 (2004).
37. Paulsson, G., Zhou, X., Trnquist, E. & Hansson, G. K.
Oligoclonal T cell expansions in atherosclerotic lesions
of apoE-deficient mice. Arterioscler. Thromb. Vasc.
Biol. 20, 1017 (2000).
38. Stemme, S., Holm, J. & Hansson, G. K. T lymphocytes
in human atherosclerotic plaques are memory cells
expressing CD45RO and the integrin VLA-1.
Arterioscler. Thromb. 12, 206211 (1992).
39. Angeli, V. et al. Dyslipidemia associated with
atherosclerotic disease systemically alters dendritic
cell mobilization. Immunity 21, 561574 (2004).
40. Wang, X. et al. Positional identification of TNFSF4,
encoding OX40 ligand, as a gene that influences
atherosclerosis susceptibility. Nature Genet.
37, 365372 (2005).
41. Swanberg, M. et al. MHC2TA is associated
with differential MHC molecule expression and
susceptibility to rheumatoid arthritis, multiple
sclerosis and myocardial infarction. Nature Genet.
37, 486494 (2005).
42. Stemme, S. et al. T lymphocytes from human
atherosclerotic plaques recognize oxidized low
density lipoprotein. Proc. Natl Acad. Sci. USA
92, 38933897 (1995).
43. de Boer, O. J. et al. Unstable atherosclerotic
plaques contain T-cells that respond to Chlamydia
pneumoniae. Cardiovasc. Res. 48, 402408 (2000).
44. Palinski, W. et al. Low density lipoprotein undergoes
oxidative modification in vivo. Proc. Natl Acad. Sci.
USA 86, 13721376 (1989).
45. Palinski, W. et al. Cloning of monoclonal
autoantibodies to epitopes of oxidized lipoproteins
from apolipoprotein E-deficient mice. Demonstration
of epitopes of oxidized low density lipoprotein in
human plasma. J. Clin. Invest. 98, 800814 (1996).
46. Chicz, R. M. et al. Specificity and promiscuity among
naturally processed peptides bound to HLA-DR alleles.
J. Exp. Med. 178, 2747 (1993).
47. Zhou, X., Caligiuri, G., Hamsten, A., Lefvert, A. K. &
Hansson, G. K. LDL immunization induces T-cell-
dependent antibody formation and protection against
atherosclerosis. Arterioscler. Thromb. Vasc. Biol.
21, 108114 (2001).
48. Stemme, S. et al. T lymphocytes from human
atherosclerotic plaques recognize oxidized LDL.
Proc. Natl Acad. Sci. USA 92, 38933897 (1995).
49. Shaw, P. X. et al. Natural antibodies with the T15
idiotype may act in atherosclerosis, apoptotic
clearance, and protective immunity. J. Clin. Invest.
105, 173117340 (2000).
50. Binder, C. J. et al. Pneumococcal vaccination
decreases atherosclerotic lesion formation: molecular
mimicry between Streptococcus pneumoniae and
oxidized LDL. Nature Med. 9, 736743 (2003).
51. Zhou, X., Nicoletti, A., Elhage, R. & Hansson, G. K.
Transfer of CD4
+
T cells aggravates atherosclerosis
in immunodeficient apolipoprotein E knockout mice.
Circulation 102, 29192922 (2000).
52. Tupin, E. et al. CD1d-dependent activation of NKT
cells aggravates atherosclerosis. J. Exp. Med.
199, 417422 (2004).
53. Melian, A., Geng, Y. J., Sukhova, G. K., Libby, P. &
Porcelli, S. A. CD1 expression in human atherosclerosis.
A potential mechanism for T cell activation by foam
cells. Am. J. Pathol. 155, 775786 (1999).
54. Nakai, Y. et al. Natural killer T cells accelerate
atherogenesis in mice. Blood 104, 20512059
(2004).
55. Uyemura, K. et al. Cross-regulatory roles of interleukin
(IL)-12 and IL-10 in atherosclerosis. J. Clin. Invest.
97, 21302138 (1996).
56. Frostegard, J. et al. Cytokine expression in advanced
human atherosclerotic plaques: dominance of
pro-inflammatory (Th1) and macrophage-stimulating
cytokines. Atherosclerosis 145, 3343. (1999).
57. Gupta, S. et al. IFN- potentiates atherosclerosis in
ApoE knock-out mice. J. Clin. Invest. 99, 27522761
(1997).
58. Buono, C. et al. Influence of interferon- on the extent
and phenotype of diet-induced atherosclerosis in the
LDLR-deficient mouse. Arterioscler. Thromb. Vasc.
Biol.23, 454460 (2003).
59. Davenport, P. & Tipping, P. G. The role of interleukin-4
and interleukin-12 in the progression of
atherosclerosis in apolipoprotein E-deficient mice.
Am. J. Pathol. 163, 11171125 (2003).
60. Elhage, R. et al. Reduced atherosclerosis in
interleukin-18 deficient apolipoprotein E-knockout
mice. Cardiovasc. Res. 59, 234240 (2003).
61. Branen, L. et al. Inhibition of tumor necrosis
factor- reduces atherosclerosis in apolipoprotein E
knockout mice. Arterioscler. Thromb. Vasc. Biol.
24, 21372142 (2004).
62. Buono, C. et al. T-bet deficiency reduces
atherosclerosis and alters plaque antigen-specific
immune responses. Proc. Natl Acad. Sci. USA
102, 15961601 (2005).
63. Whitman, S. C., Ravisankar, P., Elam, H. &
Daugherty, A. Exogenous interferon- enhances
atherosclerosis in apolipoprotein E
/
mice.
Am. J. Pathol. 157, 18191824 (2000).
64. Laurat, E. et al. In vivo downregulation of T helper
cell 1 immune responses reduces atherogenesis
in apolipoprotein E-knockout mice. Circulation
104, 197202 (2001).
65. Paigen, B., Morrow, A., Brandon, C., Mitchell, D. &
Holmes, P. Variation in susceptibility to atherosclerosis
among inbred strains of mice. Atherosclerosis 57,
6573 (1985).
66. Huber, S. A., Sakkinen, P., David, C., Newell, M. K. &
Tracy, R. P. T helper-cell phenotype regulates
atherosclerosis in mice under conditions of mild
hypercholesterolemia. Circulation 103, 26102616
(2001).
67. Mallat, Z. et al. Interleukin-18/interleukin-18 binding
protein signaling modulates atherosclerotic lesion
development and stability. Circ. Res. 89, E41E45
(2001).
68. Whitman, S. C., Ravisankar, P. & Daugherty, A.
Interleukin-18 enhances atherosclerosis in
apolipoprotein E
/
mice through release of
interferon-. Circ. Res. 90, e34e38 (2002).
69. King, V. L., Szilvassy, S. J. & Daugherty, A.
Interleukin-4 deficiency decreases atherosclerotic
lesion formation in a site-specific manner in female
LDL receptor
/
mice. Arterioscler. Thromb. Vasc. Biol.
22, 456461 (2002).
70. Shimizu, K., Shichiri, M., Libby, P., Lee, R. T. & Mitchell,
R. N. Th2-predominant inflammation and blockade of
IFN- signaling induce aneurysms in allografted aortas.
J. Clin. Invest. 114, 300308 (2004).
71. Friesel, R., Komoriya, A. & Maciag, T. Inhibition of
endothelial cell proliferation by -interferon. J. Cell
Biol. 104, 689696 (1987).
72. Hansson, G. K., Hellstrand, M., Rymo, L., Rubbia, L. &
Gabbiani, G. Interferon inhibits both proliferation
and expression of differentiation-specific -smooth
muscle actin in arterial smooth muscle cells.
J. Exp. Med. 170, 15951608 (1989).
73. Amento, E. P., Ehsani, N., Palmer, H. & Libby, P.
Cytokines and growth factors positively and negatively
regulate interstitial collagen gene expression in
human vascular smooth muscle cells. Arterioscler.
Thromb. 11, 12231230 (1991).
74. van Hinsbergh, V. W. M., van den Berg, E. A., Fiers, W.
& Dooijewaard, G. Tumor necrosis factor induces the
production of urokinase-type plasminogen activator
by human endothelial cells. Blood 75, 19911998
(1990).
75. Lee, E. et al. Regulation of matrix metalloproteinases
and plasminogen activator inhibitor-1 synthesis by
plasminogen in cultured human vascular smooth
muscle cells. Circ. Res. 78, 4449 (1996).
76. Saren, P., Welgus, H. G. & Kovanen, P. T. TNF-
and IL-1 selectively induce expression of 92-kDa
gelatinase by human macrophages. J. Immunol.
157, 41594165 (1996).
77. Jovinge, S. et al. Evidence for a role of tumor necrosis
factor in disturbances of triglyceride and glucose
metabolism predisposing to coronary heart disease.
Metabolism 47, 113118 (1998).
78. Boquist, S. et al. Alimentary lipemia, postprandial
triglyceride-rich lipoproteins, and common carotid
intima-media thickness in healthy, middle-aged men.
Circulation 100, 723728 (1999).
79. Beutler, B. & Cerami, A. Cachectin and tumour
necrosis factor as two sided of the same biological
coin. Nature 320, 584588 (1986).
80. Mach, F., Schoenbeck, U., Bonnefoy, J.-Y., Pober, J. &
Libby, P. Activation of monocyte/macrophage functions
related to acute atheroma complication by ligation
of CD40. Induction of collagenase, stromelysin, and
tissue factor. Circulation 96, 396399 (1997).
81. Mach, F. et al. Functional CD40 ligand is expressed on
human vascular endothelial cells, smooth muscle cells,
and macrophages- implications for CD40CD40
ligand signaling in atherosclerosis. Proc. Natl Acad.
Sci. USA 94, 19311936 (1997).
82. Henn, V. et al. CD40 ligand on activated platelets
triggers an inflammatory reaction of endothelial cells.
Nature 391, 591594 (1998).
83. Mach, F., Schnbeck, U., Sukhova, G. K., Atkinson, E.
& Libby, P. Reduction of atherosclerosis in mice by
inhibition of CD40 signalling. Nature 394, 200203
(1998).
84. Lutgens, E. et al. Requirement for CD154 in
the progression of atherosclerosis. Nature Med.
5, 13131316 (1999).
85. Mallat, Z. et al. Protective role of interleukin-10
in atherosclerosis. Circ. Res. 85, e17e24 (1999).
86. Pinderski Oslund, L. J. et al. Interleukin-10 blocks
atherosclerotic events in vitro and in vivo. Arterioscler.
Thromb. Vasc. Biol.19, 284753 (1999).
87. Caligiuri, G. et al. Interleukin-10 deficiency increases
atherosclerosis, thrombosis, and low-density
lipoproteins in apolipoprotein E knockout mice.
Mol. Med. 9, 1017 (2003).
88. Grainger, D. J. et al. The serum concentration of active
transforming growth factor- is severely depressed in
advanced atherosclerosis. Nature Med. 1, 7479
(1995).
89. Mallat, Z. et al. Inhibition of transforming growth
factor- signaling accelerates atherosclerosis and
induces an unstable plaque phenotype in mice.
Circ. Res. 89, 930934 (2001).
90. Lutgens, E. et al. Transforming growth factor-
mediates balance between inflammation and fibrosis
during plaque progression. Arterioscler. Thromb. Vasc.
Biol. 22, 975982 (2002).
91. Robertson, A. K. et al. Disruption of TGF- signaling
in T cells accelerates atherosclerosis. J. Clin. Invest.
112, 13421350 (2003).
92. Gojova, A. et al. Specific abrogation of transforming
growth factor- signaling in T cells alters
atherosclerotic lesion size and composition in mice.
Blood 102, 40524058 (2003).
93. Ait-Oufella, H. et al., Natural regulatory T cells control
the development of atherosclerosis in mice. Nature
Med. 12, 178180 (2006).
94. Salonen, J. T. et al. Autoantibody against oxidised
LDL and progression of carotid atherosclerosis.
Lancet 339, 883887 (1992).
95. Fredrikson, G. N. et al. Identification of immune
responses against aldehyde-modified peptide
sequences in apoB associated with cardiovascular
disease. Arterioscler. Thromb. Vasc. Biol. 23, 872878
(2003).
96. Shaw, P. X. et al. Human-derived anti-oxidized LDL
autoantibody blocks uptake of oxidized LDL
by macrophages and localizes to atherosclerotic
lesions in vivo. Arterioscler. Thromb. Vasc. Biol.
21, 13331339 (2001).
97. Kol, A., Sukhova, G. K., Lichtman, A. H. & Libby, P.
Chlamydial heat shock protein 60 localizes in human
atheroma and regulates macrophage tumor necrosis
factor- and matrix metalloproteinase expression.
Circulation 98, 300307 (1998).
98. Xu, Q. et al. Association of serum antibodies to
heat-shock protein 65 with carotid atherosclerosis.
Lancet 341, 255259 (1993).
REVI EWS
518 | JULY 2006 | VOLUME 6 www.nature.com/reviews/immunol
2006 Nature Publishing Group
99. Perschinka, H. et al. Cross-reactive B-cell epitopes
of microbial and human heat shock protein 60/65
in atherosclerosis. Arterioscler. Thromb. Vasc. Biol.
23, 10601065 (2003).
100. Caligiuri, G., Nicoletti, A., Poirier, B. & Hansson, G. K.
Protective immunity against atherosclerosis carried
by B cells of hypercholesterolemic mice. J. Clin. Invest.
109, 745753 (2002).
101. Libby, P. & Aikawa, M. Stabilization of atherosclerotic
plaques: new mechanisms and clinical targets.
Nature Med. 8, 12571262 (2002).
102. Henney, A. M. et al. Localization of stromelysin
gene expression in atherosclerotic plaques by
in situ hybridization. Proc. Natl Acad. Sci. USA
88, 81548158 (1991).
103. Galis, Z. S., Sukhova, G. K., Lark, M. W. & Libby, P.
Increased expression of matrix metalloproteinases
and matrix degrading activity in vulnarable regions
of human atherosclerotic plaques. J. Clin. Invest.
94, 24932503 (1994).
104. Dollery, C. & Libby, P. Atherosclerosis and
proteinase activation. Cardiovasc. Res. 69, 625635
(2006).
105. Buchner, K. et al. CD40 ligand is selectively expressed
on CD4
+
T cells and platelets: implications for
CD40CD40L signalling in atherosclerosis. J. Pathol.
201, 288295 (2003).
106. Poon, M., Badimon, J. J. & Fuster, V. Overcoming
restenosis with sirolimus: from alphabet soup
to clinical reality. Lancet 359, 619622 (2002).
107. Jonasson, L., Holm, J. & Hansson, G. K. Cyclosporin A
inhibits smooth muscle proliferation in the vascular
response to injury. Proc. Natl Acad. Sci. USA
85, 23032306 (1988).
108. Randomised trial of cholesterol lowering in
4444 patients with coronary heart disease:
the Scandinavian Simvastatin Survival Study (4S).
Lancet 344, 13831389 (1994).
109. Ridker, P. M. et al. C-reactive protein levels and
outcomes after statin therapy. N. Engl. J. Med.
352, 2028 (2005).
110. Greenwood, J., Steinman, L. & Zamvil, S.S. Statin
therapy and autoimmune disease: from protein
prenylation to immunomodulation. Nature Rev.
Immunol. 6, 358370
111. Takemoto, M. & Liao, J. K. Pleiotropic effects of
3-hydroxy-3-methylglutaryl coenzyme a reductase
inhibitors. Arterioscler. Thromb. Vasc. Biol.
21, 17121719 (2001).
112. Kwak, B., Mulhaupt, F., Myit, S. & Mach, F. Statins
as a newly recognized type of immunomodulator.
Nature Med. 6, 13991402 (2000).
113. Mehra, M. R. & Raval, N. Y. Metaanalysis of statins
and survival in de novo cardiac transplantation.
Transplant. Proc. 36, 15391541 (2004).
114. McCarey, D. W. et al. Trial of atorvastatin in rheumatoid
arthritis (TARA): double-blind, randomised placebo-
controlled trial. Lancet 363, 20152021 (2004).
115. Youssef, S. et al. The HMG-CoA reductase inhibitor,
atorvastatin, promotes a Th2 bias and reverses
paralysis in central nervous system autoimmune
disease. Nature 420, 7884 (2002).
116. Marx, N. et al. PPAR activators as antiinflammatory
mediators in human T lymphocytes: implications
for atherosclerosis and transplantation-associated
arteriosclerosis. Circ. Res. 90, 703710 (2002).
117. Staels, B. et al. Activation of human aortic smooth-
muscle cells is inhibited by PPAR but not by PPAR
activators. Nature 393, 790793 (1998).
118. Fitzgerald, G. A. Coxibs and cardiovascular disease.
N. Engl. J. Med. 351, 17091711 (2004).
119. Solomon, S. D. et al. Cardiovascular risk associated
with celecoxib in a clinical trial for colorectal adenoma
prevention. N. Engl. J. Med. 352, 10711080 (2005).
120. Mattner, J. et al. Exogenous and endogenous
glycolipid antigens activate NKT cells during microbial
infections. Nature 434, 525529 (2005).
121. Liuzzo, G. et al. The prognostic value of C-reactive
protein and serum amyloid A protein in severe unstable
angina. N. Engl. J. Med. 331, 417424 (1994).
122. Ridker, P. M., Hennekens, C. H., Buring, J. E. &
Rifai, N. C-reactive protein and other markers of
inflammation in the prediction of cardiovascular
disease in women. N. Engl. J. Med. 342, 836843
(2000).
123. Danesh, J. et al. C-reactive protein and other circulating
markers of inflammation in the prediction of coronary
heart disease. N. Engl. J. Med. 350, 13871397
(2004).
124. Palinski, W., Miller, E. & Witztum, J. L. Immunization
of low density lipoprotein (LDL) receptor-deficient
rabbits with homologous malondialdehyde-modified
LDL reduces atherogenesis. Proc. Natl Acad. Sci. USA
92, 821825 (1995).
125. Ameli, S. et al. Effect of immunization with
homologous LDL and oxidized LDL on early
atherosclerosis in hypercholesterolemic rabbits.
Arterioscler. Thromb. Vasc. Biol. 16, 10741079
(1996).
126. George, J. et al. Hyperimmunization of apo-E-deficient
mice with homologous malondialdehyde low-density
lipoprotein suppresses early atherogenesis.
Atherosclerosis 138, 147152 (1998).
127. Freigang, S., Hrkk, S., Miller, E., Witztum, J. L. &
Palinski, W. Immunization of LDL receptor-deficient
mice with homologous malondialdehyde-modified
and native LDL reduces progression of atherosclerosis
by mechanisms other than induction of high titers of
antibodies to oxidative neoepitopes. Arterioscler.
Thromb. Vasc. Biol.18, 19721982 (1998).
128. Fredrikson, G. N. et al. Inhibition of atherosclerosis
in apoE-null mice by immunization with apoB-100
peptide sequences. Arterioscler. Thromb. Vasc.
Biol.23, 879884 (2003).
129. Zhou, X., Robertson, A. K., Hjerpe, C. &
Hansson, G. K. Adoptive transfer of CD4
+
T cells
reactive to modified low-density lipoprotein
aggravates atherosclerosis. Arterioscler. Thromb.
Vasc. Biol. 26, 864870 (2006).
130. Afek, A. et al. Immunization of low-density
lipoprotein receptor deficient (LDL-RD) mice with
heat shock protein 65 (HSP-65) promotes early
atherosclerosis. J. Autoimmun. 14, 115121
(2000).
131. Harats, D., Yacov, N., Gilburd, B., Shoenfeld, Y. &
George, J. Oral tolerance with heat shock protein 65
attenuates Mycobacterium tuberculosis-induced and
high-fat-diet-driven atherosclerotic lesions. J. Am. Coll.
Cardiol. 40, 13331338 (2002).
132. Maron, R. et al. Mucosal administration of heat shock
protein-65 decreases atherosclerosis and
inflammation in aortic arch of low-density lipoprotein
receptor-deficient mice. Circulation 106, 17081715
(2002).
133. George, J. et al. Induction of early atherosclerosis
in LDL-receptor-deficient mice immunized with
2-glycoprotein I. Circulation 98, 11081115
(1998).
Acknowledgements
We regret that we have not been able to cite many important
papers owing to space limitations. Our research is supported
by grants from the Swedish Research Council, Heart-Lung
Foundation, European Community, US National Institutes of
Health and Leducq Foundation.
Competing interests statement
The authors declare no competing financial interests.
DATABASES
The following terms in this article are linked online to:
Entrez Gene:
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=gene
APOE | CCL2 | CD14 | CD40 | CD40L | CD68 | CX
3
CR1 |
HSP60 | IFN | IL-4 | LDLR | MMP1 | PPAR | PPAR | TLR4 | TNF |
VCAM1
FURTHER INFORMATION
Peter Libbys homepage:
http://reynolds.brighamandwomens.org/faculty/libby.asp
Gran K. Hanssons homepage:
http://www.ki.se/medicin/medicine_ks/experimental_
cardiovascular_research_unit/index_en.html
Access to this links box is available online.
REVI EWS
NATURE REVIEWS | IMMUNOLOGY VOLUME 6 | JULY 2006 | 519
2006 Nature Publishing Group
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Nbme Recopilation FlashcardsDocument17 pagesNbme Recopilation FlashcardsIlse Pol TRuiz100% (1)
- The Evolving Tumor Microenvironment From Cancer Initiation To Metastatic OutgrowthDocument30 pagesThe Evolving Tumor Microenvironment From Cancer Initiation To Metastatic OutgrowthJose EdgarNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Asthma Lancet 23febDocument18 pagesAsthma Lancet 23febMr. LNo ratings yet
- UWorld Notes 2Document49 pagesUWorld Notes 2Dinesh Kumar ReddyNo ratings yet
- Vitamin B12 Boots Energy and Cures FatigueDocument9 pagesVitamin B12 Boots Energy and Cures FatiguecantodelcisneNo ratings yet
- Scavenger ReceptorsDocument9 pagesScavenger ReceptorsAlexis Jesus GomezNo ratings yet
- Rol de CaMKII en AritmiaDocument5 pagesRol de CaMKII en AritmiaAlexis Jesus GomezNo ratings yet
- Estres Oxidativo en Enf CardioDocument11 pagesEstres Oxidativo en Enf CardioAlexis Jesus GomezNo ratings yet
- Silenciamiento CCR2 PDFDocument17 pagesSilenciamiento CCR2 PDFAlexis Jesus GomezNo ratings yet
- Atherosclerosis en DiabetesDocument11 pagesAtherosclerosis en DiabetesAlexis Jesus GomezNo ratings yet
- 2021 - NEJM - The Evolving Challenge of Infections in CirrhosisDocument14 pages2021 - NEJM - The Evolving Challenge of Infections in CirrhosisHồ Huy HoàngNo ratings yet
- Drug Acting On Immune SystemDocument7 pagesDrug Acting On Immune SystemAnne Giselle PatocNo ratings yet
- HTMLE SEMINAR NOTES DOC. ORTEGA - CompressedDocument35 pagesHTMLE SEMINAR NOTES DOC. ORTEGA - CompressedNISSI JUNE T. UNGABNo ratings yet
- S.I.R.S & M.O.DDocument36 pagesS.I.R.S & M.O.Dshrikanth007No ratings yet
- Impaired Skin IntegrityDocument2 pagesImpaired Skin IntegrityVINCE ONATONo ratings yet
- Ch2 IS3 TestDocument12 pagesCh2 IS3 TestJohn Smith100% (1)
- How Vaccines Can Damage Your Brain, Russell BlaylockDocument9 pagesHow Vaccines Can Damage Your Brain, Russell BlaylockCherie RaymondNo ratings yet
- Inflammatory Responses in The Placenta Upon SARS-CoV-2 Infection Late in PregnancyDocument28 pagesInflammatory Responses in The Placenta Upon SARS-CoV-2 Infection Late in Pregnancyn9vthqdn4kNo ratings yet
- Vaccines 08 00764Document19 pagesVaccines 08 00764Mai Chi PhạmNo ratings yet
- 25 Top Foods Herbs To Slash Chronic InflammationDocument39 pages25 Top Foods Herbs To Slash Chronic InflammationEisha KarolNo ratings yet
- PIIS1748681520303417Document6 pagesPIIS1748681520303417Lavinia CristianNo ratings yet
- 445 CMED 222 Pathology of The Pancreas PDFDocument12 pages445 CMED 222 Pathology of The Pancreas PDFGepher CanoyNo ratings yet
- MMC 8Document27 pagesMMC 8Neil Patrick AngelesNo ratings yet
- 1992 Final Report On The Safety Assessment of Polyvinyl AcetateDocument9 pages1992 Final Report On The Safety Assessment of Polyvinyl Acetaterajesh kothariNo ratings yet
- Mechanisms, Pathophysiology, and Therapy of Arterial StiffnessDocument12 pagesMechanisms, Pathophysiology, and Therapy of Arterial StiffnessDididi WekaNo ratings yet
- Serrapeptase Book Edition 4 WebDocument358 pagesSerrapeptase Book Edition 4 WebIvan Curcio100% (2)
- Forbidden Secrets From Nature's Pharmacy To Reverse Diabetes and Blood Sugar ProblemsDocument54 pagesForbidden Secrets From Nature's Pharmacy To Reverse Diabetes and Blood Sugar Problemsa1khanNo ratings yet
- 22 - Atypical Squamous Cells in Liquid-Based CervicalDocument6 pages22 - Atypical Squamous Cells in Liquid-Based CervicalRenan RodriguesNo ratings yet
- Path NotesDocument111 pagesPath NotesNirav Patel100% (1)
- Association Between Oral Contraceptive Use and Interleukin-6 Levels and Periodontal HealthDocument8 pagesAssociation Between Oral Contraceptive Use and Interleukin-6 Levels and Periodontal Healthmy srNo ratings yet
- 6 A-Hot ToothDocument14 pages6 A-Hot ToothYadnesh DondulkarNo ratings yet
- Faecal Calprotectin Indicates Intestinal InflammatDocument2 pagesFaecal Calprotectin Indicates Intestinal Inflammatakbar011512No ratings yet
- Dr. Harish Thesis PlanDocument20 pagesDr. Harish Thesis PlanAyush JainNo ratings yet
- PHILIPPINES Asthma Consensus Guidelines 2009Document134 pagesPHILIPPINES Asthma Consensus Guidelines 2009Sirias_black50% (2)
- MFG E8介导的骨免疫在牙周炎中的作用研究进展 向群Document5 pagesMFG E8介导的骨免疫在牙周炎中的作用研究进展 向群颜加龙No ratings yet