Download as xlsx, pdf, or txt
You might also like
- MandalaDocument80 pagesMandalavanag99152100% (1)
- Saving My Knee Guide by The Stone Clinic Copy (New)Document11 pagesSaving My Knee Guide by The Stone Clinic Copy (New)Aleksandra LSNo ratings yet
- Pharmacology Notes (Chapter 20 and 21)Document2 pagesPharmacology Notes (Chapter 20 and 21)graycorypNo ratings yet
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocument2 pagesLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Pharmacology FirecrackerDocument37 pagesPharmacology FirecrackerRehan Usman100% (1)
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Drug-Drug InteractionDocument9 pagesDrug-Drug InteractionHo Shi XianNo ratings yet
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresNo ratings yet
- Pharmacology A - NSAIDSDocument14 pagesPharmacology A - NSAIDSselflessdoctorNo ratings yet
- Ultimate Pharm GuideDocument41 pagesUltimate Pharm GuideeanguyenNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- KDT Only ClassificationsDocument72 pagesKDT Only ClassificationsDebashis ParidaNo ratings yet
- A-Autonomic Drugs: 1) CholinergicDocument28 pagesA-Autonomic Drugs: 1) CholinergicMahmoud Ahmed MahmoudNo ratings yet
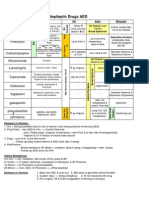
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Drug Recommendation GuideDocument6 pagesDrug Recommendation GuideGenNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- PCOL Maps PDFDocument11 pagesPCOL Maps PDFZinc YuloNo ratings yet
- Chart Antibacterial Drugs PDFDocument1 pageChart Antibacterial Drugs PDFMunaf AlsumaryNo ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Agents For Anemia, Hematopoietic, & Myeloproliferative DiseasesDocument2 pagesAgents For Anemia, Hematopoietic, & Myeloproliferative Diseaseskaylakmills_10135868No ratings yet
- Pharmacology TableDocument9 pagesPharmacology TableMaryam KhushbakhatNo ratings yet
- Drug of Choice in Various Diseases - Candidiasis - PharmacologyDocument1 pageDrug of Choice in Various Diseases - Candidiasis - PharmacologyPragnesh ParmarNo ratings yet
- (CV2) Pharmacology of AnticoagulantsDocument6 pages(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNo ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Common Medications UsedDocument3 pagesCommon Medications UsedRay Michael CasupananNo ratings yet
- Microbiology Step 1 Antimicrobials ChartDocument6 pagesMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Anti HypertensivesDocument15 pagesAnti HypertensivesFaye MillanesNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- Beta BlockersDocument1 pageBeta BlockersShrikant ThakurNo ratings yet
- Ischaemic Heart DiseaseDocument30 pagesIschaemic Heart DiseaseEB100% (1)
- Cancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationDocument5 pagesCancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationOndari gisemba OSINDENo ratings yet
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Antihistamines - AMBOSS PDFDocument5 pagesAntihistamines - AMBOSS PDFOpio IsaacNo ratings yet
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- DRUG of CHOICE - InfectiousDocument1 pageDRUG of CHOICE - InfectiousJoseph De JoyaNo ratings yet
- Classification of Drugs PDFDocument15 pagesClassification of Drugs PDFmuhammad ihtisham ul hassanNo ratings yet
- Hmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, InteractionsDocument6 pagesHmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, Interactionswaste78No ratings yet
- Anticoagulants Drug TableDocument1 pageAnticoagulants Drug TableNicole HoNo ratings yet
- NERVOUS MnemonicsDocument4 pagesNERVOUS MnemonicsHimNo ratings yet
- Drug TerminologyDocument5 pagesDrug Terminologyimdaking123No ratings yet
- OTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderDocument2 pagesOTC Pain Relievers Dosage Chart For Adults and Children 12 Years and OlderAdocueNo ratings yet
- Drug ListsDocument10 pagesDrug ListsAmber Merritt100% (1)
- List of Look-Alike MedicationsDocument5 pagesList of Look-Alike MedicationsAhmad TaramsyNo ratings yet
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsDocument17 pagesWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuNo ratings yet
- Pharm Drug Outline AdrDocument1 pagePharm Drug Outline AdrCess Lagera YbanezNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Parkinson's Disorder - Classification and MechanismDocument1 pageParkinson's Disorder - Classification and MechanismVương TúNo ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- C. Anti-Hypertensive Drugs.Document10 pagesC. Anti-Hypertensive Drugs.Nabeel AsifNo ratings yet
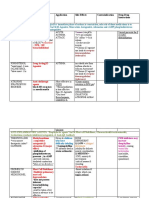
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- Klasifikasi Dan Mekanisme ABDocument8 pagesKlasifikasi Dan Mekanisme ABDeboyjackNo ratings yet
- Clinical Use of Monoclonal Antibodies: Abciximab Infliximab TrastuzumabDocument15 pagesClinical Use of Monoclonal Antibodies: Abciximab Infliximab TrastuzumabAndleeb ImranNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- DRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesDocument3 pagesDRUG SUMMARY TABLE - Anticoagulantes y AntiagregantesManuel BetancurNo ratings yet
- Antiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Document1 pageAntiplatelet Drug Comparison Chart (Asa-Clopi-Prasu-Tica)Ponpimol Odee BongkeawNo ratings yet
- PharmacologyDocument23 pagesPharmacologyAbhisek ChatterjeeNo ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- SettingsDocument2 pagesSettingsbjpalmer100% (3)
- The Profession of Physical Therapy - Definition and DevelopmentDocument50 pagesThe Profession of Physical Therapy - Definition and DevelopmentJiggs LimNo ratings yet
- Addiction ScienceDocument72 pagesAddiction ScienceAnizan SalimNo ratings yet
- Classification of Electrical Installations in Healthcare Jul10 enDocument20 pagesClassification of Electrical Installations in Healthcare Jul10 enAndres ZuñigaNo ratings yet
- Fundamentals of Nursing Gladys Bautista Jaime 2010Document10 pagesFundamentals of Nursing Gladys Bautista Jaime 2010Clarissa GuifayaNo ratings yet
- Nutraceuticals Leaflet ENGDocument2 pagesNutraceuticals Leaflet ENGDr. Dragos CobzariuNo ratings yet
- Cognitive Therapy of Anxiety DisordersDocument50 pagesCognitive Therapy of Anxiety DisordersJacquiNo ratings yet
- Enteral Feeding: Gastric Versus Post-Pyloric: Table 1Document22 pagesEnteral Feeding: Gastric Versus Post-Pyloric: Table 1tasmeow23No ratings yet
- Ilaç Listesi ESKIDocument11 pagesIlaç Listesi ESKIDursun KorkmazNo ratings yet
- Chronic Total OcclusionsDocument37 pagesChronic Total OcclusionsValentin CHIONCELNo ratings yet
- TB DrugsDocument14 pagesTB DrugsLexy CadigalNo ratings yet
- Community Pharmacy Case Studies: Case Study - Patient SafetyDocument2 pagesCommunity Pharmacy Case Studies: Case Study - Patient SafetyNuwaira BalochNo ratings yet
- Oxy CadDocument21 pagesOxy CadrlinaoNo ratings yet
- Mark Scheme: Biology 4411Document13 pagesMark Scheme: Biology 4411monjohnsonNo ratings yet
- Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATADocument61 pagesDiagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATAtabhsinghiNo ratings yet
- Hepatitis BDocument25 pagesHepatitis BJevon AndraNo ratings yet
- Countertransference As Active ImaginationDocument19 pagesCountertransference As Active ImaginationGubs SabanNo ratings yet
- BJD Methotrxate PDFDocument22 pagesBJD Methotrxate PDFSoumya MarangadNo ratings yet
- Vitamin b12 and Pregnancy - With ReferencesDocument2 pagesVitamin b12 and Pregnancy - With Referencesapi-271190857No ratings yet
- Portugal April 2014Document54 pagesPortugal April 2014Olga MihaelaNo ratings yet
- GK QA ProceduresDocument64 pagesGK QA ProceduresJared MehargNo ratings yet
- Introduction To Clinical Psychology 8th Edition Kramer Test BankDocument11 pagesIntroduction To Clinical Psychology 8th Edition Kramer Test Bankkayleelopezotwgncixjb100% (36)
- Renal Ultrasound in CKD OmicsDocument24 pagesRenal Ultrasound in CKD Omicskrishnadoctor1No ratings yet
- Assignement Blood Sugar LevelDocument4 pagesAssignement Blood Sugar LevelDeo NzigilwaNo ratings yet
- Micronutrients Assignment-14th EdDocument3 pagesMicronutrients Assignment-14th EdMan Tue ThaiNo ratings yet
- Red BiotechnologyDocument17 pagesRed BiotechnologyJonas SaintNo ratings yet
- Systematic Review On Sucess of Narrow-Diameter Dental ImplantsDocument37 pagesSystematic Review On Sucess of Narrow-Diameter Dental ImplantsMaryGonzalesʚïɞNo ratings yet
- Mr. Shoaib Hakeem How To Manage Recalls and Withdrawls of PharmaceuticalsDocument25 pagesMr. Shoaib Hakeem How To Manage Recalls and Withdrawls of PharmaceuticalsSally PujaNo ratings yet