Download as pdf or txt
You might also like
- Science Stage 4 P2 2023Document10 pagesScience Stage 4 P2 2023Weijie Weng100% (4)
- ICAO PhraseologyDocument15 pagesICAO Phraseologyahmed4dodi100% (2)
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- IV Fluids InternetDocument59 pagesIV Fluids Internetmark100% (18)
- Fluid & Electrolyte TherapyDocument38 pagesFluid & Electrolyte Therapyharjuna100% (1)
- Hoarding DesignDocument6 pagesHoarding DesignBhavin JoshiNo ratings yet
- Fluids & Electrolytes Acid/Bas Balance: DR Wael SadaqahDocument72 pagesFluids & Electrolytes Acid/Bas Balance: DR Wael Sadaqahdr wael sadaqaNo ratings yet
- Fluid, Electrolyte, and Acid-Base Balance: Distribution of Body FluidsDocument12 pagesFluid, Electrolyte, and Acid-Base Balance: Distribution of Body Fluidsadadan100% (1)
- Perioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud UniversityDocument47 pagesPerioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud Universityarifjo7999No ratings yet
- 2012-Fluid and ElectrolytesDocument192 pages2012-Fluid and ElectrolytesHarley Justiniani Dela CruzNo ratings yet
- IV FluidDocument49 pagesIV Fluidibrahimadnan040No ratings yet
- Intravenous FluidsDocument19 pagesIntravenous Fluidsnicolinna2000yahoo.comNo ratings yet
- Fluid Therapy Final 2019 DR TaanoDocument39 pagesFluid Therapy Final 2019 DR TaanoCabdi WaliNo ratings yet
- CH 27 Acid & BasesDocument6 pagesCH 27 Acid & BasesRJ ManierNo ratings yet
- 2012-Fluid and ElectrolytesDocument192 pages2012-Fluid and Electrolyteskyuss2No ratings yet
- Fluids, Blood and Blood Products ManagementDocument19 pagesFluids, Blood and Blood Products ManagementNur Amin MuhammadNo ratings yet
- Hypovolemic ShockDocument8 pagesHypovolemic ShockLyka Flores100% (1)
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedNo ratings yet
- Fluid ManagementDocument10 pagesFluid ManagementdradaadNo ratings yet
- PPC15 FEN SlidesDocument88 pagesPPC15 FEN SlidesbrianzflNo ratings yet
- Terapi Cairan CompDocument33 pagesTerapi Cairan CompWidychii GadiestchhetyaNo ratings yet
- Medical and Surgical Nursing by Sonny M Moreno RN MAN PDFDocument328 pagesMedical and Surgical Nursing by Sonny M Moreno RN MAN PDFfanchasticommsNo ratings yet
- Intro To Fluid and Electrolytes 2022Document42 pagesIntro To Fluid and Electrolytes 2022David Dwane Art SilorioNo ratings yet
- Fluids and ElectrolytesDocument123 pagesFluids and ElectrolytesAiza Apelada-NievaNo ratings yet
- Manajemen Perioperatif Terapi Cairan Pada PediatriDocument35 pagesManajemen Perioperatif Terapi Cairan Pada PediatriZulhendraNo ratings yet
- Dehydration 'Acid Base Balance DisordersDocument38 pagesDehydration 'Acid Base Balance DisordersMalika SadridinovaNo ratings yet
- 7.vet Fluid TherapyDocument44 pages7.vet Fluid TherapyAshishNo ratings yet
- Overview of Fluid and Electrolyte MaintenanceDocument54 pagesOverview of Fluid and Electrolyte MaintenanceIan WongNo ratings yet
- Fluid and Electrolyte Balance: M. Rasjad Indra Laboratorium Ilmu Faal Fk. UnibrawDocument26 pagesFluid and Electrolyte Balance: M. Rasjad Indra Laboratorium Ilmu Faal Fk. UnibrawRahardian SigmawanNo ratings yet
- Balda Electrolyte DisbalanceDocument33 pagesBalda Electrolyte DisbalanceBaldandorj KhavalkhaanNo ratings yet
- Fluid 2021Document65 pagesFluid 2021ditof58671No ratings yet
- Fluids and ElectrolytesDocument192 pagesFluids and ElectrolytesTeodora JoghiuNo ratings yet
- Pathophysiology (NUR 190) Carmen Corder, MSN, RN Fluids and Electrolyte BalanceDocument17 pagesPathophysiology (NUR 190) Carmen Corder, MSN, RN Fluids and Electrolyte BalanceSydney DeringNo ratings yet
- Fluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWDocument43 pagesFluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWaslanNo ratings yet
- Fluids ElectrolytesDocument37 pagesFluids ElectrolytesAlpascaFirdausNo ratings yet
- Intane Eng-03-Disturbances of Fluid and Electrolyte BalanceDocument50 pagesIntane Eng-03-Disturbances of Fluid and Electrolyte BalancerNo ratings yet
- Fluid TherapyDocument44 pagesFluid Therapyhacker ammerNo ratings yet
- Body FluidDocument37 pagesBody FluidBir Mohammad SonetNo ratings yet
- Fluid TherapyDocument36 pagesFluid TherapyAmin MasromNo ratings yet
- Intravenous FluidDocument42 pagesIntravenous Fluid2mvdsg9cm7No ratings yet
- Week 3Document396 pagesWeek 3Danica Mae BianitoNo ratings yet
- Dr. Faiez Alhmoud Albashir Teaching HospitalDocument76 pagesDr. Faiez Alhmoud Albashir Teaching HospitalDr-Firas Nayf Al-ThawabiaNo ratings yet
- Lots of Salt Causes Retention of WaterDocument8 pagesLots of Salt Causes Retention of WaterMarchant Lowry BleyNo ratings yet
- Approach To AKIDocument51 pagesApproach To AKImaruf47774No ratings yet
- Sr. No. 92-Alternatives of Blood Transfusion+Clinical AwarenessDocument10 pagesSr. No. 92-Alternatives of Blood Transfusion+Clinical Awarenessbushan warpeNo ratings yet
- Body Fluid, Electrolyte FcpsDocument73 pagesBody Fluid, Electrolyte FcpsInzamamul Haque ShihabNo ratings yet
- IV Fluid Management: Islam Awni Abu SamraDocument41 pagesIV Fluid Management: Islam Awni Abu SamraIslam AwniNo ratings yet
- Pleno Pakar Blok EmergencyDocument30 pagesPleno Pakar Blok EmergencyakhomanNo ratings yet
- Turkey Book 03 Internal Medicine PDFDocument47 pagesTurkey Book 03 Internal Medicine PDFPreaisNo ratings yet
- FLUID and ELECTROLYTE THERAPY Latest Changes 2018 - 2019 For Medical StudentsDocument41 pagesFLUID and ELECTROLYTE THERAPY Latest Changes 2018 - 2019 For Medical StudentssyafiqahNo ratings yet
- Principles of Dialysis: Diffusion, Convection, and Dialysis MachinesDocument6 pagesPrinciples of Dialysis: Diffusion, Convection, and Dialysis MachinesD'phiLea EyFfaNo ratings yet
- Disturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NDocument52 pagesDisturbances in Water, Electrolyte and Acid-Base Balance: Dr. Njau.N.NKeith OmwoyoNo ratings yet
- Fluid and Electrolytes: Ma. Medine L. Amorsolo RN ManDocument29 pagesFluid and Electrolytes: Ma. Medine L. Amorsolo RN ManMichael Baylon Dueñas100% (1)
- b0907 FluidDocument43 pagesb0907 FluidyamtotlNo ratings yet
- Intravenous Fluid (6th. 7th. Weeks)Document20 pagesIntravenous Fluid (6th. 7th. Weeks)Samer AlBaghdadiNo ratings yet
- Fluid and Blood TherapyDocument84 pagesFluid and Blood Therapyjean uwakijijweNo ratings yet
- Most of Your Questions Exam Will Be On The Nursing AspectDocument8 pagesMost of Your Questions Exam Will Be On The Nursing AspectLarine WinkleblackNo ratings yet
- Water and Electrolyte ImbalanceDocument49 pagesWater and Electrolyte ImbalanceNur atikahNo ratings yet
- ORS and IV Fluids (Handout)Document30 pagesORS and IV Fluids (Handout)NeshrenNo ratings yet
- Sodium and Water Metabolism: A C J HutchessonDocument66 pagesSodium and Water Metabolism: A C J Hutchessonmonday125No ratings yet
- IV Fluid TherapyDocument28 pagesIV Fluid Therapyansuh2250% (2)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Physiology of Pregnancy Yang 2003Document21 pagesPhysiology of Pregnancy Yang 2003Divaa OktavianitaNo ratings yet
- Nutrition in Pregnancy: Dr. Minidian FasitasariDocument39 pagesNutrition in Pregnancy: Dr. Minidian FasitasariDivaa OktavianitaNo ratings yet
- Cirrhosis CT and MR Imaging EvaluationDocument13 pagesCirrhosis CT and MR Imaging EvaluationDivaa OktavianitaNo ratings yet
- Comparison of Ultrasound andDocument7 pagesComparison of Ultrasound andDivaa OktavianitaNo ratings yet
- L-Arginine and Vitamin D Adjunctive Therapies in Pulmonary Tuberculosis: A Randomised, Double-Blind, Placebo-Controlled TrialDocument12 pagesL-Arginine and Vitamin D Adjunctive Therapies in Pulmonary Tuberculosis: A Randomised, Double-Blind, Placebo-Controlled TrialDivaa OktavianitaNo ratings yet
- CKDDocument8 pagesCKDDivaa OktavianitaNo ratings yet
- Date of The Earthquake Place of The Earthquake Magnitude Intensity DamagesDocument3 pagesDate of The Earthquake Place of The Earthquake Magnitude Intensity DamagesJerardwyn Grace PeñaNo ratings yet
- 2022 Photo Contest WinnersDocument5 pages2022 Photo Contest WinnersMeghan O'DellNo ratings yet
- Tsunami Safety ChecklistDocument1 pageTsunami Safety ChecklistAmerican Red Cross100% (2)
- Tire Size Chart ENG 151106 PDFDocument1 pageTire Size Chart ENG 151106 PDFBashry BassNo ratings yet
- Weather Disturbances in The Philippines PDF FileDocument40 pagesWeather Disturbances in The Philippines PDF FileERVIN DANCANo ratings yet
- Dev Comm Plan 3 4Document5 pagesDev Comm Plan 3 4Hannah Zemira Aduana EndozoNo ratings yet
- WBS For Metro ProjectDocument3 pagesWBS For Metro ProjectPooja PawarNo ratings yet
- CWTS 2 Module 1 Disaster PreparednessDocument18 pagesCWTS 2 Module 1 Disaster PreparednessJozel ValenzuelaNo ratings yet
- Aerator Type ABS Venturi Jet: ApplicationsDocument4 pagesAerator Type ABS Venturi Jet: ApplicationsRafael ZimmermannNo ratings yet
- CLASS - 6th SCIENCE CHAPTER - WATERDocument2 pagesCLASS - 6th SCIENCE CHAPTER - WATERexperimentoboyNo ratings yet
- S166T PDFDocument2 pagesS166T PDFAndrea Devky KresnaNo ratings yet
- Lift VentDocument4 pagesLift Ventismi iqhwan ihsanNo ratings yet
- Eo Suspension of Work August 24Document2 pagesEo Suspension of Work August 24Aimeereen CuregNo ratings yet
- Geography General Studies-I Mains Previous Year QuestionsDocument5 pagesGeography General Studies-I Mains Previous Year QuestionssalmanNo ratings yet
- Weather Forecasting Made Simple PDFDocument65 pagesWeather Forecasting Made Simple PDFAndis OrravsNo ratings yet
- Andrew Antena CV3PX310R1 CRET INTEGRADODocument2 pagesAndrew Antena CV3PX310R1 CRET INTEGRADOMarianoNo ratings yet
- Irfp460a PDFDocument8 pagesIrfp460a PDFMihai RobertNo ratings yet
- Action Song Competition Song Lyrics SK Lubok Tekurok, LimbangDocument1 pageAction Song Competition Song Lyrics SK Lubok Tekurok, LimbangDollynaNo ratings yet
- KBE Main Brochure Handling Care Ventilation 334PR1000 0315 Web PDFDocument12 pagesKBE Main Brochure Handling Care Ventilation 334PR1000 0315 Web PDFJoão Paulo Fernandes MonteiroNo ratings yet
- Steam Trap Calculation Sheet - 01Document7 pagesSteam Trap Calculation Sheet - 01Erwin Firmansyah Saputro0% (1)
- East Flowing Rivers Between Pennar and Kanyakumari BasinDocument147 pagesEast Flowing Rivers Between Pennar and Kanyakumari BasinpujaNo ratings yet
- CHP 20 Major Natural Regions of The WorldDocument61 pagesCHP 20 Major Natural Regions of The WorldAlfiya PathanNo ratings yet
- Aisc - 7-10-Wind Load CalculationDocument18 pagesAisc - 7-10-Wind Load CalculationameyyammaiNo ratings yet
- ChemicalDocument1 pageChemicalTimothy John IgnacioNo ratings yet
- 1 PBDocument12 pages1 PBVitus AntonioNo ratings yet
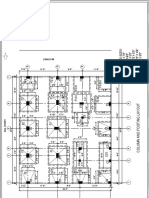
- Column and Footing LayoutDocument1 pageColumn and Footing LayoutV.m. RajanNo ratings yet
- Route Description: State Route 157 (SR 157) Is A 39.1-Mile-Long (62.9 KM)Document2 pagesRoute Description: State Route 157 (SR 157) Is A 39.1-Mile-Long (62.9 KM)Unknown24No ratings yet