Download as pdf or txt
You might also like
- FDA Approval GuideDocument38 pagesFDA Approval GuideYuwono WibowoNo ratings yet
- Evaluation of Non Stress Test in Monitoring High Risk PregnanciesDocument3 pagesEvaluation of Non Stress Test in Monitoring High Risk PregnanciesIOSRjournalNo ratings yet
- Grand Rounds: Jinghua Chen, MD, PHD July 15Th, 2016Document23 pagesGrand Rounds: Jinghua Chen, MD, PHD July 15Th, 2016miraNo ratings yet
- Population Based Study of EpisiotomyDocument6 pagesPopulation Based Study of EpisiotomyMeriton Stanly ANo ratings yet
- Intussusception Korea ResearchDocument11 pagesIntussusception Korea ResearchУрнго Ө.No ratings yet
- Effectiveness of Monovalent Rotavirus Vaccine in The PhilippinesDocument8 pagesEffectiveness of Monovalent Rotavirus Vaccine in The PhilippinesRomulo Vincent PerezNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Typhoid Fever in Children: Immunization A Preventive Strategy To Reduce The Burden of DiseaseDocument24 pagesTyphoid Fever in Children: Immunization A Preventive Strategy To Reduce The Burden of Diseasemoon1312No ratings yet
- Research Article: Treatment and Outcome For Children With Esophageal Atresia From A Gender PerspectiveDocument7 pagesResearch Article: Treatment and Outcome For Children With Esophageal Atresia From A Gender PerspectivedaxNo ratings yet
- Comparison Between Small and Large Bowel Intussusception in ChildrenDocument3 pagesComparison Between Small and Large Bowel Intussusception in ChildrenParamartha KesumaNo ratings yet
- Infecção Urinária em Refluxo Vesico UreteralDocument87 pagesInfecção Urinária em Refluxo Vesico UreteralLuiz renatoNo ratings yet
- Prenatal Factors Associated With The Risk of Stunting: A Multilevel Analysis Evidence From Nganjuk, East JavaDocument7 pagesPrenatal Factors Associated With The Risk of Stunting: A Multilevel Analysis Evidence From Nganjuk, East JavaRido SaputraNo ratings yet
- C01110916 PDFDocument8 pagesC01110916 PDFLestari Chye PouedanNo ratings yet
- Integrated Management of Childhood Illness in Outpatient Department of A University HospitalDocument6 pagesIntegrated Management of Childhood Illness in Outpatient Department of A University Hospitalpastizal123456No ratings yet
- Current Success in The Treatment of Intussusception in ChildrenDocument9 pagesCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniNo ratings yet
- Day 1 TasP PrEP - DitangcoDocument20 pagesDay 1 TasP PrEP - DitangcoRye CalderonNo ratings yet
- Einc Newborn Mar 2011Document70 pagesEinc Newborn Mar 2011maxicap73100% (2)
- Hiperalgesia PDFDocument6 pagesHiperalgesia PDFannagm97No ratings yet
- Antenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane LibraryDocument88 pagesAntenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane Libraryjavier dauvergneNo ratings yet
- Type 1 Diabetes Impairs Female Fertility Even Before It Is DiagnosedDocument8 pagesType 1 Diabetes Impairs Female Fertility Even Before It Is DiagnosedAuliana FENo ratings yet
- 1 s2.0 S0264410X14000085 Main PDFDocument8 pages1 s2.0 S0264410X14000085 Main PDFwilmaNo ratings yet
- Critical Appraisal RCT B.ingDocument3 pagesCritical Appraisal RCT B.ingﺳﻮﺘﻴﺎﺳﻴﻪNo ratings yet
- Clinical Study: Nitazoxanide in Acute Rotavirus Diarrhea: A Randomized Control Trial From A Developing CountryDocument6 pagesClinical Study: Nitazoxanide in Acute Rotavirus Diarrhea: A Randomized Control Trial From A Developing CountryputraodNo ratings yet
- The PediQUEST Study - Evaluation of Pediatric Quality of Life and Evaluation of Symptoms Technology - Smart PatientsDocument10 pagesThe PediQUEST Study - Evaluation of Pediatric Quality of Life and Evaluation of Symptoms Technology - Smart PatientsDwiNo ratings yet
- Gaviscon ClinicalDocument7 pagesGaviscon ClinicalMuhammad Nadzri NoorhayatuddinNo ratings yet
- Wales 2004Document6 pagesWales 2004Subha ManivannanNo ratings yet
- Anesthesia-Related Complications in ChildrenDocument14 pagesAnesthesia-Related Complications in ChildrenAissyiyah Nur An NisaNo ratings yet
- EndometritisDocument6 pagesEndometritisMuh Syarifullah ANo ratings yet
- Diarrhea Among Children Admitted To A Private Tertiary-Care Hospital, Bangkok, Thailand: A Case SeriesDocument9 pagesDiarrhea Among Children Admitted To A Private Tertiary-Care Hospital, Bangkok, Thailand: A Case SeriesSrkyn MeritNo ratings yet
- Pharmaceutical Sciences: Efficacy of First Dose of Nitazoxanide in Management of Rotavirus Diarrhea in ChildrenDocument5 pagesPharmaceutical Sciences: Efficacy of First Dose of Nitazoxanide in Management of Rotavirus Diarrhea in ChildreniajpsNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleastutikNo ratings yet
- The Effect of Preoperative Fasting To Postoperative NauseaDocument7 pagesThe Effect of Preoperative Fasting To Postoperative NauseasantiNo ratings yet
- Management of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDocument7 pagesManagement of Premature Rupture of Membranes: Ashraf Olabi and Lucy Shikh MousaDesi SafiraNo ratings yet
- TafeseDocument28 pagesTafeseWubishet TeferaNo ratings yet
- 16859604Document8 pages16859604Brent DoolanNo ratings yet
- Morning SicknessDocument7 pagesMorning SicknessNovadilah Arifia ShintadewiNo ratings yet
- 1 SM PDFDocument7 pages1 SM PDFCintia FloresNo ratings yet
- Medi 95 E2791Document5 pagesMedi 95 E2791Harnoor GhumanNo ratings yet
- Protective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsDocument5 pagesProtective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsChika FebrianiNo ratings yet
- Paediatrica Indonesiana: Teny Tjitrasari, MD Agus Firmansyah, MD, PHD Imral Chair, MDDocument7 pagesPaediatrica Indonesiana: Teny Tjitrasari, MD Agus Firmansyah, MD, PHD Imral Chair, MDakreditasi rsunhNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Comparative Study of Nifedipine and Isoxpurine As Tocolytics For Preterm LaborDocument4 pagesComparative Study of Nifedipine and Isoxpurine As Tocolytics For Preterm LaborMeitika Wahyu Wedha WatiNo ratings yet
- Prevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFDocument4 pagesPrevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFMaría Alejandra López AriasNo ratings yet
- Sureshkumar2014 PDFDocument8 pagesSureshkumar2014 PDFFadel BilondatuNo ratings yet
- Cord Care PDFDocument7 pagesCord Care PDFudupisonyNo ratings yet
- Study DesignsDocument36 pagesStudy Designsz6f9cw8vwvNo ratings yet
- Pediatric Urinary Tract Infections: Joshua A. Hodge, Maj, USAF, MC Staff Family Physician Andrews AFB, MDDocument26 pagesPediatric Urinary Tract Infections: Joshua A. Hodge, Maj, USAF, MC Staff Family Physician Andrews AFB, MDBeep TerradoNo ratings yet
- Pubmed Preocedimiento Invasivos NeonatalesDocument2 pagesPubmed Preocedimiento Invasivos NeonataleseddcitoNo ratings yet
- 1 35Document8 pages1 35Saiful HudaNo ratings yet
- Dental Caries and Gingivitis Among Pregnant and Non-Pregnant Women in Chiang Mai, ThailandDocument8 pagesDental Caries and Gingivitis Among Pregnant and Non-Pregnant Women in Chiang Mai, ThailandAmalia Dwi AryantiNo ratings yet
- Clinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiaDocument6 pagesClinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiamariaprincesitaNo ratings yet
- Sedation Practice Outside The Operating Room For Pediatric Gastrointestinal EndosDocument2 pagesSedation Practice Outside The Operating Room For Pediatric Gastrointestinal EndosAngeles ChNo ratings yet
- Mitchell Pretb P1041ipt For Childrencroi TB Hiv MeetingDocument27 pagesMitchell Pretb P1041ipt For Childrencroi TB Hiv Meetingalemd23No ratings yet
- Pediatrics 2003 Clark 986 90Document7 pagesPediatrics 2003 Clark 986 90Giavanny Eka Rani PuteriNo ratings yet
- Systematic Review of The Occurrence of Infantile Colic in The CommunityDocument7 pagesSystematic Review of The Occurrence of Infantile Colic in The CommunityJovitaNo ratings yet
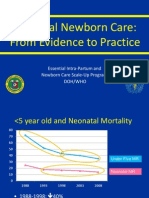
- Essential Intrapartum Care: From Evidence To PracticeDocument78 pagesEssential Intrapartum Care: From Evidence To PracticeGeline Joy D. SamillanoNo ratings yet
- Yes, Materi 16 Januari 2013Document42 pagesYes, Materi 16 Januari 2013Hendra SetyawanNo ratings yet
- Trismus Xerostomia and Nutrition Status PDFDocument9 pagesTrismus Xerostomia and Nutrition Status PDFAstutikNo ratings yet
- Corticosteroid Dosing in Pediatric Acute Severe Ulcerative Colitis: A Propensity Score AnalysisDocument7 pagesCorticosteroid Dosing in Pediatric Acute Severe Ulcerative Colitis: A Propensity Score AnalysisfandyNo ratings yet
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- Rotavirus Preventive Vaccines and A Rare Side EffectDocument6 pagesRotavirus Preventive Vaccines and A Rare Side EffectInternational Journal of Innovative Science and Research Technology100% (1)
- QLD Immunisation Schedule Under 10Document2 pagesQLD Immunisation Schedule Under 10Anonymous oTObTTNo ratings yet
- Diarrhea in Children: Dr. Hodan S. Ahmed, Dept of Pediatrics and Child Health Amoud Medical School, AUDocument20 pagesDiarrhea in Children: Dr. Hodan S. Ahmed, Dept of Pediatrics and Child Health Amoud Medical School, AUabdisalaan hassanNo ratings yet
- Prevention of DiseasesDocument27 pagesPrevention of DiseasesDhritismita KalitaNo ratings yet
- Global Illness and Deaths Caused by Rotavirus Disease in ChildrenDocument8 pagesGlobal Illness and Deaths Caused by Rotavirus Disease in ChildrenelyNo ratings yet
- Vaccines and Vaccination History and Emerging IssuesDocument15 pagesVaccines and Vaccination History and Emerging IssuesMěđ SimoNo ratings yet
- NO. Diseases Vaccine Type Doses Dosage Site Brand Names: Route Interval Age Given (First Dose)Document3 pagesNO. Diseases Vaccine Type Doses Dosage Site Brand Names: Route Interval Age Given (First Dose)Breezy ReveloNo ratings yet
- 2371 - Parents' Attitudes Regarding Childhood Vaccination With Focus On Rotavirus Vaccination in Bishkek, KyrgyzstanDocument8 pages2371 - Parents' Attitudes Regarding Childhood Vaccination With Focus On Rotavirus Vaccination in Bishkek, KyrgyzstanMustafa YılmazNo ratings yet
- BOPV SIA2024 OrientationDocument36 pagesBOPV SIA2024 OrientationFranz SalazarNo ratings yet
- CDC's Appendix B-Pink Book - Vaccines - Ingredient ListDocument4 pagesCDC's Appendix B-Pink Book - Vaccines - Ingredient ListmickelleNo ratings yet
- Acute Diarrhea in Adults and Children A Global PerspectiveDocument10 pagesAcute Diarrhea in Adults and Children A Global PerspectiverobyNo ratings yet
- Wyeth Rotashield Package InsertDocument19 pagesWyeth Rotashield Package InsertGeeleegoatNo ratings yet
- Pathophysiology: Poststreptococcal GlomerulonephritisDocument6 pagesPathophysiology: Poststreptococcal GlomerulonephritiscathycolNo ratings yet
- Rotavirus: Signs and SymptomsDocument17 pagesRotavirus: Signs and SymptomsLaura Anghel-MocanuNo ratings yet
- Science Magazine 5692 2004-09-24Document95 pagesScience Magazine 5692 2004-09-24WillimSmithNo ratings yet
- 07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingDocument10 pages07 Intussusception and Midgut Volvulus - 2015-05-12 - AHC Media: Continuing Medical Education PublishingPridina SyadirahNo ratings yet
- Diarrhea Among Hospitalized Children Under Five A Call For Inclusion Ofrotavirus Vaccine To The National Immunization Program in Indonesia PDFDocument6 pagesDiarrhea Among Hospitalized Children Under Five A Call For Inclusion Ofrotavirus Vaccine To The National Immunization Program in Indonesia PDFritaNo ratings yet
- HEALTH - Vaccine Ingredients Published by CDC - Updated February 2012Document3 pagesHEALTH - Vaccine Ingredients Published by CDC - Updated February 2012MoralVolcanoNo ratings yet
- Sample Chapter: Miscellaneous VirusesDocument7 pagesSample Chapter: Miscellaneous VirusesskNo ratings yet
- Safety Profile of Rotavac: Observational Prospective StudyDocument7 pagesSafety Profile of Rotavac: Observational Prospective StudyMalook Sekhon100% (1)
- Advances en Pediatrics 2013Document395 pagesAdvances en Pediatrics 2013Gris C. RicoNo ratings yet
- Dirty Vaccines: New Study Reveals Prevalence of ContaminantsDocument5 pagesDirty Vaccines: New Study Reveals Prevalence of Contaminantsrblais100% (1)
- Paediatric ProtocolsDocument434 pagesPaediatric ProtocolsJashveerBediNo ratings yet
- National Immunisation Program: Queensland ScheduleDocument1 pageNational Immunisation Program: Queensland ScheduleHarshpreet KaurNo ratings yet
- Viral Gastroenteritis-1Document17 pagesViral Gastroenteritis-1Abdus SubhanNo ratings yet
- Kepi Vaccines (2) - Gi - 1Document30 pagesKepi Vaccines (2) - Gi - 1okwadha simionNo ratings yet
- Viral Gastroenteritis 508Document8 pagesViral Gastroenteritis 508Billy ChandraNo ratings yet
- VAD Vesikari Scoring ManualDocument51 pagesVAD Vesikari Scoring Manualmuhamad mukhtarNo ratings yet
- 0900 1030 Nicolette Graham PDFDocument28 pages0900 1030 Nicolette Graham PDFhinaNo ratings yet