Download as pdf or txt
You might also like
- APC CAOP Practice Paper Answer Sheet v1.2014 PDFDocument4 pagesAPC CAOP Practice Paper Answer Sheet v1.2014 PDFhappyscottlee3438100% (1)
- Anesthetic Formulation of Tumescent SolutionsDocument9 pagesAnesthetic Formulation of Tumescent SolutionsJorgeNo ratings yet
- Premalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Document60 pagesPremalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Rajat NangiaNo ratings yet
- Rough DraftDocument3 pagesRough Draftapi-285224563No ratings yet
- Cannabis ReportDocument7 pagesCannabis ReportKlaudija LutovskaNo ratings yet
- Symbicort LeafletDocument10 pagesSymbicort Leafletsheeno2607No ratings yet
- Ophthalmic Drugs PDFDocument21 pagesOphthalmic Drugs PDFHussain Syed100% (2)
- 494 PDFDocument6 pages494 PDFranz ibonkNo ratings yet
- Oral Lichen PlanusDocument10 pagesOral Lichen PlanusChander KantaNo ratings yet
- Australian Dental Journal - 2010 - Schifter - Oral Mucosal Diseases The Inflammatory DermatosesDocument16 pagesAustralian Dental Journal - 2010 - Schifter - Oral Mucosal Diseases The Inflammatory Dermatosesneetika guptaNo ratings yet
- Painfulorallesions: Istvan A. HargitaiDocument13 pagesPainfulorallesions: Istvan A. HargitaiAlejandro Ln CNo ratings yet
- OLPandupdate Carrozzo ThorpeDocument13 pagesOLPandupdate Carrozzo ThorpeAstrid Dwi SattiNo ratings yet
- Oral Leukoplakia and ErythroplakiaDocument8 pagesOral Leukoplakia and ErythroplakiadeepaNo ratings yet
- 4 PDFDocument5 pages4 PDFLisda PraditaNo ratings yet
- KP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutDocument58 pagesKP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutAditya ZulfikarNo ratings yet
- Lichen Planus and Lichenoid Reactions of The Oral Mucosa: Bethanee J. SchlosserDocument17 pagesLichen Planus and Lichenoid Reactions of The Oral Mucosa: Bethanee J. SchlosserYeni PuspitasariNo ratings yet
- Keratoses IIDocument83 pagesKeratoses IIGomogi SouqNo ratings yet
- Arduino 2017Document8 pagesArduino 2017neetika guptaNo ratings yet
- Leukoplakia 170519204224Document27 pagesLeukoplakia 170519204224Mihai SemeniucNo ratings yet
- White Lesions of The Oral MucosaDocument213 pagesWhite Lesions of The Oral MucosaJunaid Ramzan100% (1)
- Keratoses and Related Disorders of Oral Mucosa II (Slide 4 + 5 + 6)Document83 pagesKeratoses and Related Disorders of Oral Mucosa II (Slide 4 + 5 + 6)JustDen09No ratings yet
- Oral Lichenoid Lesions Distinguishing The Benign From The Deadly Modern PathologyDocument1 pageOral Lichenoid Lesions Distinguishing The Benign From The Deadly Modern PathologyPreda MihaelaNo ratings yet
- DR Meenakshi MDS Oral PathologyDocument29 pagesDR Meenakshi MDS Oral PathologyDr. Meenakshi SinghalNo ratings yet
- Accepted Manuscript: Oral Surgery, Oral Medicine, Oral Pathology and Oral RadiologyDocument33 pagesAccepted Manuscript: Oral Surgery, Oral Medicine, Oral Pathology and Oral RadiologyJihan AttamimiNo ratings yet
- Oral Pathology: Hyperplasia of Oral MucosaDocument7 pagesOral Pathology: Hyperplasia of Oral Mucosaعلي صادق جعفرNo ratings yet
- Oral Lichen PlanusDocument12 pagesOral Lichen PlanusMeuthia AzzahraNo ratings yet
- Lec. 13 &14 Epithelial DisordersDocument10 pagesLec. 13 &14 Epithelial DisordersZainab Alshamary0% (1)
- Scientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportDocument6 pagesScientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportSasa AprilaNo ratings yet
- Pre Malignant Conditions of Oral CavityDocument20 pagesPre Malignant Conditions of Oral CavityAsma sultanaNo ratings yet
- Transformasi Ganas Lichen Planus F, Rosif Mukosamulut: IJD 2006 Edisi Khusus KppkgxiyDocument3 pagesTransformasi Ganas Lichen Planus F, Rosif Mukosamulut: IJD 2006 Edisi Khusus KppkgxiyMuhammadNaufalNo ratings yet
- KalmarDocument8 pagesKalmarKING COMICNo ratings yet
- Oral Leukoerythroplakia A Case ReportDocument6 pagesOral Leukoerythroplakia A Case ReportArdelvie YoandaNo ratings yet
- Unilateral LeUkoedema - Case ReportDocument2 pagesUnilateral LeUkoedema - Case ReportBramita Beta ArnandaNo ratings yet
- LeukoplakiaDocument60 pagesLeukoplakiadimasahadiantoNo ratings yet
- Vesicubullous Diseases & Mucocutaneous DisordersDocument23 pagesVesicubullous Diseases & Mucocutaneous Disordersshahlaraib001No ratings yet
- A Clinical Approach White LesionDocument5 pagesA Clinical Approach White LesionTirta KusumaNo ratings yet
- Desquamative Gingivitis: A Sign of Mucocutaneous Disorders - A ReviewDocument6 pagesDesquamative Gingivitis: A Sign of Mucocutaneous Disorders - A Reviewsidra malikNo ratings yet
- Speckled Leukoplakia-Case Report and Review of LiteratureDocument3 pagesSpeckled Leukoplakia-Case Report and Review of LiteratureAlya Hana NatasyaNo ratings yet
- White & Red Lesion 33333 Lecture (1)Document16 pagesWhite & Red Lesion 33333 Lecture (1)ربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنNo ratings yet
- Premalignant LesionsDocument76 pagesPremalignant LesionsGowri RaguNo ratings yet
- LP 160610182350Document25 pagesLP 160610182350Karthik TNo ratings yet
- Report OncoDocument23 pagesReport Oncoabdallahtarek2000No ratings yet
- Chronic Oral LesionsDocument16 pagesChronic Oral LesionsJAVIERA HIDALGONo ratings yet
- Proceedings 35 00001 v3Document3 pagesProceedings 35 00001 v3Georgi GugicevNo ratings yet
- Premalignant Oral LesionsDocument94 pagesPremalignant Oral LesionssdinyantiNo ratings yet
- Jurnalku OsccDocument4 pagesJurnalku OsccAndiOctafiantoNo ratings yet
- Out 7Document8 pagesOut 7Musthafa Afif WardhanaNo ratings yet
- DBST Dlja INO Studentov (PDF - Io)Document6 pagesDBST Dlja INO Studentov (PDF - Io)eidNo ratings yet
- Oral Leukoplakia: Well-Demarcated, White Plaques Are Visible On The Lateral Aspects of The TongueDocument3 pagesOral Leukoplakia: Well-Demarcated, White Plaques Are Visible On The Lateral Aspects of The TonguePhúc Hồ Văn TâmNo ratings yet
- Management of Oral Lichen Plannus: A Clinical Study: Jayachandran S, Koijamsashikumar SDocument4 pagesManagement of Oral Lichen Plannus: A Clinical Study: Jayachandran S, Koijamsashikumar Sranz ibonkNo ratings yet
- Vulvar Lichen Planus - Goldstein MetzDocument6 pagesVulvar Lichen Planus - Goldstein MetzMahmud Abdullah RrahmanosmaniNo ratings yet
- Leukoplakia and HomoeopathyDocument8 pagesLeukoplakia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Pathology of The Oral Cavity and Salivary GlandsDocument10 pagesPathology of The Oral Cavity and Salivary GlandsAbdul hadiNo ratings yet
- Salinan Terjemahan Jamur Fitzpatricks Dermatology in General Medicine 8ed - 1Document4 pagesSalinan Terjemahan Jamur Fitzpatricks Dermatology in General Medicine 8ed - 1RubiahSheBiachNo ratings yet
- Oral Oncology: Isaäc Van Der WaalDocument3 pagesOral Oncology: Isaäc Van Der WaalFrancisco VargasNo ratings yet
- Lichen Planus: DR Hira BashirDocument37 pagesLichen Planus: DR Hira BashirSaroash SadruddinNo ratings yet
- Keratosis PatologiaDocument9 pagesKeratosis PatologiakaryNo ratings yet
- Oral UlcerationDocument10 pagesOral Ulcerationمحمد حسنNo ratings yet
- Mollaoglu 2000Document8 pagesMollaoglu 2000MilenaNo ratings yet
- Oral Patho Lecture Shlav BDocument65 pagesOral Patho Lecture Shlav Bشبيبةالروم الملكيين الكاثوليكNo ratings yet
- Erosive Lichen Planus: A Case ReportDocument4 pagesErosive Lichen Planus: A Case ReportNuningK93No ratings yet
- Hairy LeukoplakiaDocument2 pagesHairy LeukoplakiaEka Septariana PuspaNo ratings yet
- Leukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeukoplakia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- 2012 Resistant HypertensionDocument9 pages2012 Resistant HypertensionBarry Tumpal Wouter NapitupuluNo ratings yet
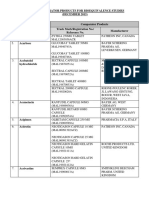
- Malaysia-NPRA List of Comparator Products For Bioequivalence Studies December 2015Document47 pagesMalaysia-NPRA List of Comparator Products For Bioequivalence Studies December 2015Noples RozaliaNo ratings yet
- Case-A-Thon Group 2Document9 pagesCase-A-Thon Group 2MatthiasNo ratings yet
- SteroidsDocument13 pagesSteroidsPrajakta DhumaleNo ratings yet
- Primaxin (Imipenem - Cilistatin)Document2 pagesPrimaxin (Imipenem - Cilistatin)ENo ratings yet
- GST Price List - Dt. 14.12.18 - Updated MRPDocument11 pagesGST Price List - Dt. 14.12.18 - Updated MRPSuryaji TelavekarNo ratings yet
- VIVIX COLLECTION PART IIedit PDFDocument4 pagesVIVIX COLLECTION PART IIedit PDFFelicia MgNo ratings yet
- Glyphosate Poisoning: Presenter: Prabu Medical Officer: Dr. NG KL Specialist: DR KauthmanDocument39 pagesGlyphosate Poisoning: Presenter: Prabu Medical Officer: Dr. NG KL Specialist: DR KauthmanPrabu PonuduraiNo ratings yet
- Jurnal Alveolar Osteitis PDFDocument6 pagesJurnal Alveolar Osteitis PDFkrwulanNo ratings yet
- Learning Book: Name: HQ: DivisionDocument39 pagesLearning Book: Name: HQ: DivisionkurutalaNo ratings yet
- Dream Job AssignmentDocument3 pagesDream Job Assignmentapi-354947009No ratings yet
- Infusion Pump & Syringe Pump RevisedDocument18 pagesInfusion Pump & Syringe Pump Revisedfrances182871% (7)
- NyeriDocument1 pageNyeriIlmiyatul MuhimmahNo ratings yet
- Potential of Piperine As A Bioavailability Enhancer: Vasika LeavesDocument10 pagesPotential of Piperine As A Bioavailability Enhancer: Vasika LeavesSushilkumar ShindeNo ratings yet
- SOP in OPTHAMOLOGYDocument6 pagesSOP in OPTHAMOLOGYKynachasya' RiverNo ratings yet
- Prescription Drug Abuse Crisis in NYS - Comprehensive ApproachDocument26 pagesPrescription Drug Abuse Crisis in NYS - Comprehensive ApproachNew York SenateNo ratings yet
- Albizzia The Tree of HappinessDocument4 pagesAlbizzia The Tree of HappinessslowhaNo ratings yet
- Paxil Withdrawal Guide 2005Document102 pagesPaxil Withdrawal Guide 2005Sunit P MehtaNo ratings yet
- Starting A PharmacyDocument8 pagesStarting A PharmacyLloyd Fyl O. RazoNo ratings yet
- Pneumococcus ExpertRules V3.2 20190613Document3 pagesPneumococcus ExpertRules V3.2 20190613Julyadharma Wangsa DharmaNo ratings yet
- Beyond Use DateDocument56 pagesBeyond Use DateDa Chan100% (1)
- Public Assessment Report Decentralised ProcedureDocument22 pagesPublic Assessment Report Decentralised ProcedureHemang M. GajjarNo ratings yet
- Antidepressant Medication - Physiologic Processes and ExerciseDocument1 pageAntidepressant Medication - Physiologic Processes and ExerciseGuille monsterNo ratings yet
- Misuse of Drugs Regulations (Document57 pagesMisuse of Drugs Regulations (Terrence LiNo ratings yet