Download as pdf or txt
You might also like
- Prometric Exam Sample QuestionsDocument9 pagesPrometric Exam Sample QuestionsDe Dios JV100% (6)
- Eukaryotes: Base of Questions of Krok-1 Exam Medical BiologyDocument54 pagesEukaryotes: Base of Questions of Krok-1 Exam Medical BiologyKarla IngaNo ratings yet
- Surgical Wound ClassificationDocument1 pageSurgical Wound Classificationgeclear323No ratings yet
- Discharge-Summary-Template JogiDocument1 pageDischarge-Summary-Template JogiJoginderNo ratings yet
- Mahi Diagnostics: Mri: Both Hip JointDocument1 pageMahi Diagnostics: Mri: Both Hip JointManish KumarNo ratings yet
- Hepatitis FinalDocument73 pagesHepatitis FinalAkhil MuraliNo ratings yet
- Hepatitis A-EDocument34 pagesHepatitis A-EVer Garcera TalosigNo ratings yet
- HIV&HepatitisDocument46 pagesHIV&HepatitisRaja RuzannaNo ratings yet
- 2018 Hepatitis Viral InfectionDocument51 pages2018 Hepatitis Viral Infectionkomang nickoNo ratings yet
- Viral HepatitisDocument49 pagesViral HepatitisAster WidodoNo ratings yet
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- Part 2 of Medical VirologyDocument113 pagesPart 2 of Medical Virologygatete samNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument48 pagesHepatitis A-E Viruses: An OverviewPrajakta TawdeNo ratings yet
- Jaundice and Hepatitis in Children: Dr. MwendwaDocument46 pagesJaundice and Hepatitis in Children: Dr. MwendwaAlvin OmondiNo ratings yet
- Hepatitis: Dr. Amany A. GhazyDocument44 pagesHepatitis: Dr. Amany A. GhazyJosé Luis García GarcíaNo ratings yet
- Hepatitis A-E Viruses: Ni Putu Galuh Wibhutisari (10-169)Document49 pagesHepatitis A-E Viruses: Ni Putu Galuh Wibhutisari (10-169)Echa Anskariani Jon PutriNo ratings yet
- HepatitisDocument39 pagesHepatitisRahmiati LaoNo ratings yet
- Hepatitis A, B and C VirusDocument46 pagesHepatitis A, B and C VirusChyzhi SylviaNo ratings yet
- CCE090 Liver and Biliary TractDocument21 pagesCCE090 Liver and Biliary TractBharathi ManiyanNo ratings yet
- Hepatitis C VirusDocument16 pagesHepatitis C Virusمصطفى رسول هاديNo ratings yet
- Viral Hepatitis: Nining Sri Wuryaningsih Bagian Patologi Klinik FK UNSDocument36 pagesViral Hepatitis: Nining Sri Wuryaningsih Bagian Patologi Klinik FK UNSdayanr02No ratings yet
- HepatitisDocument55 pagesHepatitisAbdirashidNo ratings yet
- HepatitisDocument19 pagesHepatitisDayana PrasanthNo ratings yet
- Chromosomal Structure Transmission - Epidemiology Pathogenesis - Symptoms Lab Id - Immunity Prevention and TreatmentDocument5 pagesChromosomal Structure Transmission - Epidemiology Pathogenesis - Symptoms Lab Id - Immunity Prevention and Treatmentsunnyorange88No ratings yet
- 3.0HEPATIT Lecture 5Document48 pages3.0HEPATIT Lecture 5Jiya MuhammadNo ratings yet
- HEPATITIS Compilation (From Various Sources)Document44 pagesHEPATITIS Compilation (From Various Sources)Cathy TajaoNo ratings yet
- Hepatitis BDocument23 pagesHepatitis BMarty Asis100% (1)
- HepatitisDocument55 pagesHepatitisdebdeepbhattacharya411No ratings yet
- Hepatitis: DR Putra Hendra SPPD UnibaDocument87 pagesHepatitis: DR Putra Hendra SPPD Unibayoga yogafenkanoNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument55 pagesHepatitis A-E Viruses: An OverviewRitu TripathiNo ratings yet
- HepatitisDocument55 pagesHepatitisSUTHAN100% (1)
- Hep B VirusDocument20 pagesHep B VirusBhupesh ChandNo ratings yet
- Infeksi Virus Pada Sistem Pencernaan Bawah: Hepatitis: Ety AprilianaDocument27 pagesInfeksi Virus Pada Sistem Pencernaan Bawah: Hepatitis: Ety AprilianaAsmorowatiNo ratings yet
- Hepatitis Viral - Dr. José Gonzáles BenavidesDocument64 pagesHepatitis Viral - Dr. José Gonzáles BenavidesEfrain Brian SilvaNo ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHKailash Nagar100% (1)
- Viral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityDocument67 pagesViral Hepatitis: DR - Abiy F. Nov 2019 Arsi UniversityWakjira NigusuNo ratings yet
- HCVDocument33 pagesHCVsherif555No ratings yet
- Hepatitis A-E Viruses: Farida Purnamasari.,SKM 2012Document51 pagesHepatitis A-E Viruses: Farida Purnamasari.,SKM 2012siapaa01No ratings yet
- Hepatitis Virus A Sampai eDocument48 pagesHepatitis Virus A Sampai eaulia rahmahNo ratings yet
- Hepatitis Viruses: Dr. Muna. M. A. Yousif M.D Clinical MicrobiologyDocument45 pagesHepatitis Viruses: Dr. Muna. M. A. Yousif M.D Clinical MicrobiologyMAxeneNo ratings yet
- Acute Viral Hepatitis: Acute Inflamation of The Liver Caused by Primarly Hepatotropic Viruses (A, B, C, D, E)Document35 pagesAcute Viral Hepatitis: Acute Inflamation of The Liver Caused by Primarly Hepatotropic Viruses (A, B, C, D, E)Tarik PlojovicNo ratings yet
- 1010 M Balm - Viral HepatitisDocument17 pages1010 M Balm - Viral HepatitisSaad KhanNo ratings yet
- Viral HepatitisDocument30 pagesViral HepatitisAliya DawoodNo ratings yet
- Hepatitis: Hepatitis A Hepatitis B Hepatitis C Sirrosis HepatisDocument48 pagesHepatitis: Hepatitis A Hepatitis B Hepatitis C Sirrosis Hepatisfarah maulida martaNo ratings yet
- Hepatitis A VirusDocument27 pagesHepatitis A VirusAna KarlaNo ratings yet
- Microbiology and Parasitology 100: Trinity University of Asia St. Luke's College of NursingDocument11 pagesMicrobiology and Parasitology 100: Trinity University of Asia St. Luke's College of NursingFereli Joy SupanNo ratings yet
- 2 Hepatitis VirusDocument31 pages2 Hepatitis VirusDr. Md. Abdullah YusufNo ratings yet
- General Signs/Symptoms Labs/Diagnosis Prevention Treatment: Hepatitis ADocument2 pagesGeneral Signs/Symptoms Labs/Diagnosis Prevention Treatment: Hepatitis A85robertNo ratings yet
- Vaksinasi Hep BDocument28 pagesVaksinasi Hep BMahasti AndrariniNo ratings yet
- Hepatitis B Dan C Dalam KehamilanDocument15 pagesHepatitis B Dan C Dalam Kehamilanzrombie7No ratings yet
- Hepatitis B Dalam KehamilanDocument15 pagesHepatitis B Dalam KehamilanjenniNo ratings yet
- Hepatitis: Dr. Leonardo B Dairi SPPD KgehDocument114 pagesHepatitis: Dr. Leonardo B Dairi SPPD KgehIlham riandaNo ratings yet
- Class 3: Hepatitis Outline I. Hepatitis A Transmission RiskDocument5 pagesClass 3: Hepatitis Outline I. Hepatitis A Transmission RiskTonyNo ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHwira guna pratiwiNo ratings yet
- Hepatitis ADocument16 pagesHepatitis AIngrid Masson PintoNo ratings yet
- 1 HepatitisDocument62 pages1 HepatitisKamal AhmedNo ratings yet
- HepatitisDocument46 pagesHepatitisGusti Tirtha Drag JrNo ratings yet
- Infectious Gastrointestinal Diseases: MicrobiologyDocument37 pagesInfectious Gastrointestinal Diseases: MicrobiologyRakesh KumarNo ratings yet
- Hepatitis ViralDocument17 pagesHepatitis ViralKristine Joyce RabanoNo ratings yet
- Hepatologi 1 (CMP)Document61 pagesHepatologi 1 (CMP)Yun ZhaNo ratings yet
- GUASA MT 38 ACTIVITY 8 Hepatitis UPDATEDDocument46 pagesGUASA MT 38 ACTIVITY 8 Hepatitis UPDATEDAllyssa May Callao BongcawilNo ratings yet
- Hepatitis Virus: Bagian Mikrobiologi FK UnissulaDocument36 pagesHepatitis Virus: Bagian Mikrobiologi FK UnissulaKarina Mega WNo ratings yet
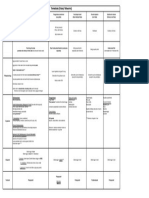
- Feature HAV HBV HCV HDV HEV: HepatitisDocument9 pagesFeature HAV HBV HCV HDV HEV: HepatitisPulseWangminNo ratings yet
- Urinechemistries: Walter P. Mutter,, Cynthia A. KorzeliusDocument15 pagesUrinechemistries: Walter P. Mutter,, Cynthia A. Korzeliusshiner99No ratings yet
- Chart TrematodsDocument1 pageChart Trematodsshiner99No ratings yet
- Parasitology SummaryDocument7 pagesParasitology Summaryshiner99100% (1)
- Chart ArbovirusesDocument1 pageChart Arbovirusesshiner99No ratings yet
- Chart RhabdovirusDocument2 pagesChart Rhabdovirusshiner99No ratings yet
- Treponema Pallidum Pallidum Borrelia Recurrentis & Hermsii Borellia Burgdorferi Leptospira InterrogansDocument2 pagesTreponema Pallidum Pallidum Borrelia Recurrentis & Hermsii Borellia Burgdorferi Leptospira Interrogansshiner99No ratings yet
- Chart Pox VirusesDocument1 pageChart Pox Virusesshiner99No ratings yet
- Intestinal Protozoa: Entamoeba Histolytica Giardia Lamblia Cryptosporidium ParvumDocument12 pagesIntestinal Protozoa: Entamoeba Histolytica Giardia Lamblia Cryptosporidium Parvumshiner99No ratings yet
- Lecture 2 (Prostatitis)Document43 pagesLecture 2 (Prostatitis)Rian Permana PNo ratings yet
- Asma Dan DBDDocument18 pagesAsma Dan DBDReynaldo SutantoNo ratings yet
- Endodontic EmmergenciesDocument27 pagesEndodontic EmmergenciesJitender Reddy100% (2)
- ABMM Sample QuestionsDocument7 pagesABMM Sample QuestionsRanjit Kumar ShahNo ratings yet
- Cephalosporins Quick ReviewDocument19 pagesCephalosporins Quick ReviewErinson Custodio PlasenciaNo ratings yet
- Non-Traditional Security Threats in Southeast Asia: Emerging Infectious DiseasesDocument103 pagesNon-Traditional Security Threats in Southeast Asia: Emerging Infectious DiseasesSophal Ear100% (1)
- 001 230277754 CC2 117 1Document1 page001 230277754 CC2 117 1irshad72No ratings yet
- Typhoid FeverDocument24 pagesTyphoid FeverHazielle BondocNo ratings yet
- Influenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionDocument3 pagesInfluenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionYusuf Rony LosongNo ratings yet
- Endodontic Microbiology: Dr. Ammar Abu MostafaDocument12 pagesEndodontic Microbiology: Dr. Ammar Abu MostafapattasonNo ratings yet
- VPD Surveillance Guidelines - PunjabDocument91 pagesVPD Surveillance Guidelines - PunjabjamshaidjiNo ratings yet
- Appendix-Vii Planned Video Teaching On Control and Prevention of Dengue FeverDocument11 pagesAppendix-Vii Planned Video Teaching On Control and Prevention of Dengue Feverkuruvagadda sagarNo ratings yet
- Pathology Mcqs 2Document6 pagesPathology Mcqs 2Numan Rox100% (5)
- An Introduction To Probiotics: Key PointsDocument6 pagesAn Introduction To Probiotics: Key PointsDinesh PuppalaNo ratings yet
- Hand Hygiene in Dental Health-Care SettingsDocument55 pagesHand Hygiene in Dental Health-Care SettingsManu DewanNo ratings yet
- Plac Pathology - Drucilla RobertsDocument11 pagesPlac Pathology - Drucilla RobertsconstantinilieNo ratings yet
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- "Bloody Scours": Swine DysenteryDocument29 pages"Bloody Scours": Swine DysenteryleaNo ratings yet
- Tumour Immunology: Von Ryan F. Lingcallo, RMTDocument20 pagesTumour Immunology: Von Ryan F. Lingcallo, RMTJuan SalenNo ratings yet
- Biodata March 19Document81 pagesBiodata March 19ULAGANATHAN MNo ratings yet
- B.SC in Nursing Syllabus 2018 For Web PDFDocument100 pagesB.SC in Nursing Syllabus 2018 For Web PDFYolanda Nadya0% (1)
- Red Eye The Role of Primary CareDocument16 pagesRed Eye The Role of Primary CareNatukunda DianahNo ratings yet
- Liver Nursing NotesDocument7 pagesLiver Nursing NotesHeather ShantaeNo ratings yet
- Retrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesDocument12 pagesRetrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesKlaus Ramirez SuarezNo ratings yet
- Thesis DoneDocument24 pagesThesis DoneAmira SaidinNo ratings yet
- Approach To Neurologic Infections.4 PDFDocument18 pagesApproach To Neurologic Infections.4 PDFosmarfalboreshotmail.comNo ratings yet
- tmpC061 TMPDocument34 pagestmpC061 TMPFrontiersNo ratings yet