Download as pdf or txt
You might also like
- Certificate of Earnings PDFDocument1 pageCertificate of Earnings PDFHoney BunniNo ratings yet
- Kuhhy PDFDocument2 pagesKuhhy PDFJay EvansNo ratings yet
- KPMG Oil and Gas Company Canada Job Application Form.Document2 pagesKPMG Oil and Gas Company Canada Job Application Form.SALMAN ANSARI100% (3)
- Tesco Oil and Gas Company United Kingdom Job Offer Application Form.Document2 pagesTesco Oil and Gas Company United Kingdom Job Offer Application Form.AJAY RAJBHAR100% (1)
- Tesco Oil and Gas Company United Kingdom Job Offer Application Form PDFDocument2 pagesTesco Oil and Gas Company United Kingdom Job Offer Application Form PDFAJAY RAJBHAR100% (1)
- Car PolicyDocument3 pagesCar PolicyimowaisqureshiNo ratings yet
- Sample Personal Information SheetDocument5 pagesSample Personal Information SheetJinky AsiloNo ratings yet
- 2021-Cmg Application FormDocument4 pages2021-Cmg Application FormCams SenoNo ratings yet
- 2021-CMG Application FormDocument4 pages2021-CMG Application Formmaykee01No ratings yet
- New Hire FormDocument13 pagesNew Hire Formbaron yustitoNo ratings yet
- Urban Rattan Employment Application FormDocument5 pagesUrban Rattan Employment Application FormOscar OyenNo ratings yet
- Application Form For EmploymentDocument1 pageApplication Form For EmploymentZiña SuilujNo ratings yet
- Employment Application: Applicant InformationDocument2 pagesEmployment Application: Applicant InformationErick AcostaNo ratings yet
- Employment ApplicationDocument3 pagesEmployment Applicationapi-355432617No ratings yet
- Application Form: Personal InformationDocument2 pagesApplication Form: Personal InformationRaymond RepitoNo ratings yet
- Employment ApplicationDocument2 pagesEmployment Applicationjackie4593No ratings yet
- Application Forms (Fillable)Document2 pagesApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNo ratings yet
- Belmont - Application For EmploymentDocument2 pagesBelmont - Application For Employmentchickennougat90No ratings yet
- 2017 Job ApplicationDocument2 pages2017 Job Applicationapi-379625810No ratings yet
- PERSONAL DATA FORM - OfferingDocument2 pagesPERSONAL DATA FORM - OfferingIGA Mirah SuwinitaNo ratings yet
- HR 001-Employee Application FormDocument4 pagesHR 001-Employee Application FormnugrasaktiNo ratings yet
- Application FormDocument1 pageApplication FormcounterpartresourceNo ratings yet
- Employment Application Form 1Document1 pageEmployment Application Form 1juNo ratings yet
- 2017 Job ApplicationDocument2 pages2017 Job Applicationapi-373188715No ratings yet
- High Point Golf Club: Employment Application 342 Shore Drive, Montague, NJ 07827 973-293-0180 Today's DateDocument2 pagesHigh Point Golf Club: Employment Application 342 Shore Drive, Montague, NJ 07827 973-293-0180 Today's DateKris TjornhomNo ratings yet
- BVC FormDocument2 pagesBVC FormArindom SenNo ratings yet
- Safer Recruitment Application Form TemplateDocument11 pagesSafer Recruitment Application Form TemplatefutureplusagraNo ratings yet
- HF02 Application For - EmploymentDocument2 pagesHF02 Application For - EmploymentkennethNo ratings yet
- KPMG Oil and Gas Company Canada Job Application Form.Document2 pagesKPMG Oil and Gas Company Canada Job Application Form.Abdul Mazith100% (2)
- FORM1Document5 pagesFORM1hasanuddinNo ratings yet
- Strand Bar AppDocument2 pagesStrand Bar AppGurlThats David Coyle's FineAssNo ratings yet
- Employment Application FormDocument3 pagesEmployment Application FormNurain AhmadNo ratings yet
- Job AppDocument2 pagesJob Appjojopaijo100% (1)
- Employment Application FormDocument2 pagesEmployment Application FormMochammad Zaki NasrullohNo ratings yet
- Align Technologies Application FormDocument2 pagesAlign Technologies Application FormSamuel PiedraNo ratings yet
- 2010 Lakeside Association Employment ApplicationDocument3 pages2010 Lakeside Association Employment ApplicationJessica BennettNo ratings yet
- Wp-Contentuploadssites6575202001employment Application JCD Revised PDFDocument3 pagesWp-Contentuploadssites6575202001employment Application JCD Revised PDFAdriona MarshallNo ratings yet
- Employment ApplicationDocument2 pagesEmployment ApplicationAlkejo HernandezNo ratings yet
- Copper City Ultra Lounge: Employment ApplicationDocument3 pagesCopper City Ultra Lounge: Employment ApplicationScott HerrigNo ratings yet
- Application For Employment-Full SetDocument4 pagesApplication For Employment-Full SetArmie FisherNo ratings yet
- Employment ApplicationDocument3 pagesEmployment ApplicationsavageculturekidNo ratings yet
- HR-F02, Emp Application Form Rev.01Document4 pagesHR-F02, Emp Application Form Rev.01Permata NoelNo ratings yet
- Application Form SampleDocument2 pagesApplication Form SampleBen MabiasanNo ratings yet
- Employment ApplicationDocument2 pagesEmployment ApplicationCassandra TufanoNo ratings yet
- Oadway Application - 58703Document2 pagesOadway Application - 58703KimoraLeeNo ratings yet
- Atlas+pizza+application 2Document2 pagesAtlas+pizza+application 2mekenzie groverNo ratings yet
- Employment ApplicationDocument4 pagesEmployment ApplicationAndre DixonNo ratings yet
- Love in A Cup Frozen Yogurt Bar: Employment ApplicationDocument3 pagesLove in A Cup Frozen Yogurt Bar: Employment ApplicationMoniqueLeeperNo ratings yet
- Employment Application For Round 6 BrewingDocument2 pagesEmployment Application For Round 6 BrewingKennyNo ratings yet
- Please Fill Out The Form Completely in UPPERCASE LETTERS Only. Put "N/A" On The Field If Not ApplicableDocument3 pagesPlease Fill Out The Form Completely in UPPERCASE LETTERS Only. Put "N/A" On The Field If Not ApplicableLlandCortezNo ratings yet
- JOB APPLICATION FORM - (Revised August 27)Document3 pagesJOB APPLICATION FORM - (Revised August 27)Ephraim RubioNo ratings yet
- Employment Application Form 1Document1 pageEmployment Application Form 1andrew malsonNo ratings yet
- Candidate Information Sheet 2017 V2Document7 pagesCandidate Information Sheet 2017 V2TesdaSibugay TvetNo ratings yet
- VHM - Employment Application Form - 2020Document5 pagesVHM - Employment Application Form - 2020NZ Smart CentreNo ratings yet
- Mlat-Form - 2022-2023 AdmissionDocument2 pagesMlat-Form - 2022-2023 AdmissionAlleah LeeNo ratings yet
- Employment Application FormDocument1 pageEmployment Application FormSelesteNo ratings yet
- Application For EmploymentDocument4 pagesApplication For EmploymentRudhi WahyudiNo ratings yet
- Task 3 - BBPP1103 Principles of ManagementDocument6 pagesTask 3 - BBPP1103 Principles of ManagementPuneswaran UmapathyNo ratings yet
- Organizational ChartDocument9 pagesOrganizational ChartSeverino ValerioNo ratings yet
- JSA For WaterproofingDocument4 pagesJSA For WaterproofingSeverino ValerioNo ratings yet
- Safety Violation ExeedDocument1 pageSafety Violation ExeedSeverino ValerioNo ratings yet
- Diploma in Accounting 2010editDocument319 pagesDiploma in Accounting 2010editSeverino Valerio100% (2)
- Harvard Referencing BasicsDocument6 pagesHarvard Referencing BasicsAnonymous y1pIqcNo ratings yet
- Fire Safety Plan TemplateDocument73 pagesFire Safety Plan TemplateSeverino Valerio100% (1)
- Admissions Code of Practice For Applicants Declaring A Criminal ConvictionsDocument8 pagesAdmissions Code of Practice For Applicants Declaring A Criminal ConvictionsSeverino ValerioNo ratings yet
- Clinical Pharmacists Job Description FinalDocument3 pagesClinical Pharmacists Job Description FinalSeverino ValerioNo ratings yet
- DBC Edp Org CharDocument1 pageDBC Edp Org CharSeverino ValerioNo ratings yet
- Gcs Application Form 91Document6 pagesGcs Application Form 91Severino ValerioNo ratings yet
- Unit 2: Working With Service Users in Care Settings (Level 3)Document11 pagesUnit 2: Working With Service Users in Care Settings (Level 3)Severino ValerioNo ratings yet
- Student Nurse Enquiry Form in UKDocument1 pageStudent Nurse Enquiry Form in UKSeverino ValerioNo ratings yet
- Chapter 3 Fluid, Electrolyte and Acid BaseDocument7 pagesChapter 3 Fluid, Electrolyte and Acid BaseSeverino Valerio100% (2)
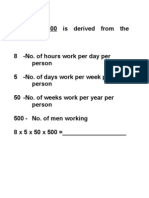
- 1,000,000 FactorDocument1 page1,000,000 FactorSeverino ValerioNo ratings yet
- INDIBEH-Group Case Study AnalysisDocument2 pagesINDIBEH-Group Case Study AnalysisRaqs GabrielNo ratings yet
- Shachi 002Document3 pagesShachi 002Dr-Vikas RathoreNo ratings yet
- Revenue Per Employee Excel TemplateDocument7 pagesRevenue Per Employee Excel TemplateMustafa Ricky Pramana SeNo ratings yet
- Lagatic Vs NLRCDocument2 pagesLagatic Vs NLRCkwok_kc100% (2)
- Social Security System: Collection List Thru UsbDocument8 pagesSocial Security System: Collection List Thru UsbLala MagayanesNo ratings yet
- BDO App FormDocument2 pagesBDO App FormIan PalmaNo ratings yet
- April 2007Document27 pagesApril 2007Amit LalchandaniNo ratings yet
- Job Satisfication QustionareDocument2 pagesJob Satisfication QustionareSachuNo ratings yet
- Payroll ManagementDocument6 pagesPayroll ManagementNisha_Yadav_6277No ratings yet
- Measuring Value of Employee Relation RetentionDocument21 pagesMeasuring Value of Employee Relation Retentionshivali_chandra100% (2)
- Week 16c Communication For Work PurposesDocument3 pagesWeek 16c Communication For Work PurposesAlexajane Jhackie100% (1)
- 5-Form12B - Previous Income DetailsDocument2 pages5-Form12B - Previous Income DetailssrinivasNo ratings yet
- Uber - JDDocument5 pagesUber - JDShipra AgrawalNo ratings yet
- Shekhar Gajendar Mandhare - Offer Letter2Document2 pagesShekhar Gajendar Mandhare - Offer Letter2shekhar mandhareNo ratings yet
- Department of Labor: Dol4eDocument2 pagesDepartment of Labor: Dol4eUSA_DepartmentOfLaborNo ratings yet
- G.R. No. L-12503Document4 pagesG.R. No. L-12503Eloissa Mae FloresNo ratings yet
- HRM 9Document18 pagesHRM 9Faizan KhanNo ratings yet
- Herrera Vs NPC - Docx 20Document1 pageHerrera Vs NPC - Docx 20Mark Bryant VitorNo ratings yet
- The Payment of Bonus Act Annual ReturnDocument4 pagesThe Payment of Bonus Act Annual ReturnNasir AhmedNo ratings yet
- PDFDocument51 pagesPDFrohandeshpande100100% (1)
- A Good HR Manager Is No Longer Just A Hirer and Firer of MenDocument5 pagesA Good HR Manager Is No Longer Just A Hirer and Firer of MenBadeesh Veluthaparambil Damodhar100% (3)
- DBMSDocument4 pagesDBMSNeil FowlerNo ratings yet
- Job Application FormDocument2 pagesJob Application Formapi-287057069No ratings yet
- HR CHAPTER 1 (Complete)Document2 pagesHR CHAPTER 1 (Complete)Rysa Mission0% (1)
- Assignment Amazon As An EmployerDocument8 pagesAssignment Amazon As An EmployerKazi Shuvo100% (1)
- 12 - Padillo v. Rural Bank of Nabunturan, IncDocument2 pages12 - Padillo v. Rural Bank of Nabunturan, IncJesi CarlosNo ratings yet
- Unfair Labor PracticesDocument3 pagesUnfair Labor PracticesKate MabanagNo ratings yet
- Sample Offer - Offer LetterDocument2 pagesSample Offer - Offer LetterharithcgNo ratings yet