Download as docx, pdf, or txt
You might also like
- The Muqarrabeen File Book 1 CompleteDocument94 pagesThe Muqarrabeen File Book 1 CompleteDhulkifl Bey96% (24)
- English: Quarter 3 - Module 1: Composing An Argumentative EssayDocument15 pagesEnglish: Quarter 3 - Module 1: Composing An Argumentative EssayMarife Magsino71% (24)
- Bachs Suites For Solo Cello BWV 1007 101 PDFDocument289 pagesBachs Suites For Solo Cello BWV 1007 101 PDFLuca Franceschelli100% (1)
- The Liver Cure: Natural Solutions for Liver Health to Target Symptoms of Fatty Liver Disease, Autoimmune Diseases, Diabetes, Inflammation, Stress & Fatigue, Skin Conditions, and Many MoreFrom EverandThe Liver Cure: Natural Solutions for Liver Health to Target Symptoms of Fatty Liver Disease, Autoimmune Diseases, Diabetes, Inflammation, Stress & Fatigue, Skin Conditions, and Many MoreRating: 3 out of 5 stars3/5 (1)
- English: Quarter 3 - Module 5Document20 pagesEnglish: Quarter 3 - Module 5Liezl Sabado89% (9)
- PronounDocument4 pagesPronounLiezl Sabado100% (1)
- Chronic Kidney Disease Case PresDocument32 pagesChronic Kidney Disease Case Presnnaesor_1091No ratings yet
- Template Career Guidance Program Action Plan Sy.20!21!1Document4 pagesTemplate Career Guidance Program Action Plan Sy.20!21!1Liezl Sabado67% (3)
- Template Career Guidance Program Action Plan Sy.20!21!1Document4 pagesTemplate Career Guidance Program Action Plan Sy.20!21!1Liezl Sabado67% (3)
- Directions: Listen To Your Teacher As He/she Reads The Song Twice Then, Answer The Questions byDocument9 pagesDirections: Listen To Your Teacher As He/she Reads The Song Twice Then, Answer The Questions byLiezl SabadoNo ratings yet
- Hepatobiliary System: Anatomy & PhysiologyDocument22 pagesHepatobiliary System: Anatomy & PhysiologyMargaret Xaira Rubio Mercado100% (1)
- Anatomy and Physiology of The Human LungDocument13 pagesAnatomy and Physiology of The Human LungRosal ClarinoNo ratings yet
- Liver: Southern Technical University Collage of Health and Medical Technology Department of Medical Lab TechnologyDocument6 pagesLiver: Southern Technical University Collage of Health and Medical Technology Department of Medical Lab Technologymortda jassimNo ratings yet
- Functions of Liver in Human BodyDocument3 pagesFunctions of Liver in Human BodyalikhanbalouchNo ratings yet
- Anatomy: Cell TypesDocument19 pagesAnatomy: Cell Typessunilsunny317No ratings yet
- Liver Disease in TCMDocument37 pagesLiver Disease in TCMrendao100% (3)
- Liver Cirrhosis: A Case Study OnDocument31 pagesLiver Cirrhosis: A Case Study OnCharmaine del RosarioNo ratings yet
- Chapter II - Digestive System: StomachDocument4 pagesChapter II - Digestive System: StomachIndranil SinhaNo ratings yet
- Anatomy and Physiology of CHOLELITHIASISDocument4 pagesAnatomy and Physiology of CHOLELITHIASISLarisse de LeonNo ratings yet
- Brief Background of The Disease: Liver CirrhosisDocument7 pagesBrief Background of The Disease: Liver CirrhosisLyra Lustre RNNo ratings yet
- Physiology of The LiverDocument12 pagesPhysiology of The Liverرشاد خالد عماد Rashad Khaled EmadNo ratings yet
- Cirrhosis Description Highlights Causes of CirrhosisDocument18 pagesCirrhosis Description Highlights Causes of Cirrhosisen-oleNo ratings yet
- Alcoholic Live DiseaseDocument53 pagesAlcoholic Live DiseaseKuldeep SinghNo ratings yet
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonNo ratings yet
- PUT 822 Coursework 1Document19 pagesPUT 822 Coursework 1Stephen KokoNo ratings yet
- The LiverDocument7 pagesThe LiverBarrameda NegideasisNo ratings yet
- CirrhosisDocument29 pagesCirrhosisHarshika KDGNo ratings yet
- Function of Liver in Human Body: Liver Physiology, Larry Frolich, Yavapai College, March 10, 2006Document16 pagesFunction of Liver in Human Body: Liver Physiology, Larry Frolich, Yavapai College, March 10, 2006alikhanbalouchNo ratings yet
- Science Reveiw JRDocument13 pagesScience Reveiw JRgemNo ratings yet
- LiverDocument2 pagesLiverHazel Ann Bragado CabacunganNo ratings yet
- A General Guide To Liver Disease in Children and Young PeopleDocument28 pagesA General Guide To Liver Disease in Children and Young PeopleAxon Physiotherapy Dr Rohit RathoreNo ratings yet
- Metabolism and EndocrineDocument156 pagesMetabolism and EndocrineGren May Angeli MagsakayNo ratings yet
- Anatomy of The Biliary System: Click To EnlargeDocument23 pagesAnatomy of The Biliary System: Click To EnlargeMohit JoshiNo ratings yet
- My Study1Document11 pagesMy Study1محمد العراقيNo ratings yet
- Diit Penyakit Hati & Kantung EmpeduDocument36 pagesDiit Penyakit Hati & Kantung EmpeduFitri RohmaniyahNo ratings yet
- Biochemistry of Liver BCM 412Document20 pagesBiochemistry of Liver BCM 412onuorahu94No ratings yet
- Liver - WikipediaDocument148 pagesLiver - WikipediaMuhammad HuzaifaNo ratings yet
- BioDocument12 pagesBioKAMESH .GNo ratings yet
- Cirrhosis ToolkitDocument39 pagesCirrhosis Toolkitvr venkatesanNo ratings yet
- The Liver: Anatomy and FunctionsDocument2 pagesThe Liver: Anatomy and FunctionsJharene BasbañoNo ratings yet
- Content Practice TeachingDocument5 pagesContent Practice TeachingIshika RoyNo ratings yet
- LiverDocument89 pagesLiverM.GANESHNo ratings yet
- Digestive System - Lecture IIDocument6 pagesDigestive System - Lecture IISaru BashaNo ratings yet
- ChirrosisDocument19 pagesChirrosisamalia rosaNo ratings yet
- Bab Ii Tinjauan Teori 2. 1 Konsep Teori 2.1.1 PengertianDocument10 pagesBab Ii Tinjauan Teori 2. 1 Konsep Teori 2.1.1 PengertianImanuel tassiNo ratings yet
- Ex Final de EnfermeriaDocument2 pagesEx Final de EnfermeriaAdriana EdithNo ratings yet
- Running Head: Human Anatomy Articles 1Document7 pagesRunning Head: Human Anatomy Articles 1Abin S ShajiNo ratings yet
- Geb203 AssignmentDocument11 pagesGeb203 AssignmentAysha Siddika MimNo ratings yet
- Digestive GlandsDocument17 pagesDigestive GlandsPrazwal RegmiNo ratings yet
- Human Body SystemDocument32 pagesHuman Body SystemMehedi MahinNo ratings yet
- Histology of LiverDocument9 pagesHistology of LiverSunil BasnetNo ratings yet
- Cholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarDocument25 pagesCholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarMc Crister Silang100% (1)
- 2017-Ozougwuj C 2017Document13 pages2017-Ozougwuj C 2017DebNo ratings yet
- How Does The Liver FunctionDocument2 pagesHow Does The Liver FunctionAnonymous j6GPMfYNo ratings yet
- 1 LiverDocument2 pages1 LiverJonance YeeNo ratings yet
- Vsmmc-Or 2009Document3 pagesVsmmc-Or 2009june allenNo ratings yet
- Liver, Gallbladder and Pancreas Final PresentationDocument60 pagesLiver, Gallbladder and Pancreas Final PresentationqueenuagNo ratings yet
- محاضرة نظري 7 19Document12 pagesمحاضرة نظري 7 19Samah AlshamiNo ratings yet
- Liver Function TestsDocument52 pagesLiver Function TestsAhaisibwe GordonNo ratings yet
- Liver Function and AnatomyDocument2 pagesLiver Function and AnatomyKeanna Nicole CollantesNo ratings yet
- Ylei The Liver ProjectDocument5 pagesYlei The Liver Projectblue55No ratings yet
- Digestive Glands Liver, Gallbladder, PancreasDocument20 pagesDigestive Glands Liver, Gallbladder, PancreasAtaberk GencerNo ratings yet
- Liver, Pancreas & Biliary Tract Lecture No. 1 John O'Dowd Outline of LecturesDocument79 pagesLiver, Pancreas & Biliary Tract Lecture No. 1 John O'Dowd Outline of LecturesZul Azim AnuarNo ratings yet
- The Liver FINALDocument9 pagesThe Liver FINALangelvic73No ratings yet
- Gastrointestinal SystemDocument3 pagesGastrointestinal SystemxhemhaeNo ratings yet
- The Liver, Biliary System and Pancreas: Group 2Document58 pagesThe Liver, Biliary System and Pancreas: Group 2Jethro GueverraNo ratings yet
- Presentation ScriptDocument3 pagesPresentation Scriptskywalking skywalkerNo ratings yet
- Abdominal Assessment: Jonalyn S. Esco,.Rn.,ManDocument77 pagesAbdominal Assessment: Jonalyn S. Esco,.Rn.,ManClifford Subagan Patil-aoNo ratings yet
- English: Quarter 3 - Module 6: Critiquing A Literary Selection Using Structuralism and Formalism ApproachDocument20 pagesEnglish: Quarter 3 - Module 6: Critiquing A Literary Selection Using Structuralism and Formalism ApproachLiezl Sabado70% (10)
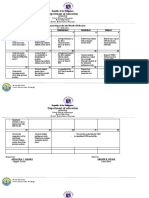
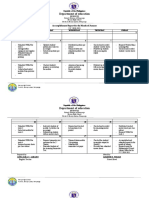
- Department of Education: Accomplishment Report For The Month of FebruaryDocument3 pagesDepartment of Education: Accomplishment Report For The Month of FebruaryLiezl SabadoNo ratings yet
- Department of Education: Accomplishment Report For The Month of JanuaryDocument3 pagesDepartment of Education: Accomplishment Report For The Month of JanuaryLiezl SabadoNo ratings yet
- (Page 1) Transmittal Letter Attention: Bernadette L. Lejarde, Phd. Magc Division Career Guidance Program and Homeroom Guidance CoordinatorDocument6 pages(Page 1) Transmittal Letter Attention: Bernadette L. Lejarde, Phd. Magc Division Career Guidance Program and Homeroom Guidance CoordinatorLiezl SabadoNo ratings yet
- Department of Education: Accomplishment Report For The Month of DecemberDocument2 pagesDepartment of Education: Accomplishment Report For The Month of DecemberLiezl SabadoNo ratings yet
- Daily Lesson Log: Day 2 (Week 1, Quarter 3)Document3 pagesDaily Lesson Log: Day 2 (Week 1, Quarter 3)Liezl SabadoNo ratings yet
- Department of Education: What Is A Context ClueDocument45 pagesDepartment of Education: What Is A Context ClueLiezl SabadoNo ratings yet
- Guide-Inventory of Modules For Teachers English 10 - Quarter 1Document3 pagesGuide-Inventory of Modules For Teachers English 10 - Quarter 1Liezl SabadoNo ratings yet
- Guide-Inventory of Modules For Teachers English 8 - Quarter 1Document3 pagesGuide-Inventory of Modules For Teachers English 8 - Quarter 1Liezl SabadoNo ratings yet
- Positive Mood Words Negative Mood Words: Some Common Mood Descriptors AreDocument2 pagesPositive Mood Words Negative Mood Words: Some Common Mood Descriptors AreLiezl Sabado100% (1)
- Elements of Stage PlayDocument1 pageElements of Stage PlayLiezl SabadoNo ratings yet
- English 10Document2 pagesEnglish 10Liezl Sabado100% (1)
- Grade 9Document11 pagesGrade 9Liezl Sabado100% (2)
- Day 1 Attitude Is AltitudeDocument1 pageDay 1 Attitude Is AltitudeLiezl SabadoNo ratings yet
- Adjectives Underlining P 1 IntermediateDocument2 pagesAdjectives Underlining P 1 IntermediateVlad VizcondeNo ratings yet
- Cline SamplesDocument1 pageCline SamplesLiezl SabadoNo ratings yet
- Semi-Detailed Lesson Plan in English Grade 10: (Continuation of The Lesson As of January 24, 2019)Document1 pageSemi-Detailed Lesson Plan in English Grade 10: (Continuation of The Lesson As of January 24, 2019)Liezl SabadoNo ratings yet
- Pre-Assessment TestDocument6 pagesPre-Assessment TestLiezl SabadoNo ratings yet
- Mental Health Services Data Set (MHSDS) Autism Statistics: Metadata FileDocument4 pagesMental Health Services Data Set (MHSDS) Autism Statistics: Metadata FileLauren-Jodie WilsonNo ratings yet
- Order SchedulingDocument26 pagesOrder Schedulingabhishek_s_gupta4753100% (1)
- Stippling Is It An Indicator of Gingival ThicknessDocument11 pagesStippling Is It An Indicator of Gingival ThicknessJoNo ratings yet
- Chap 13: Turning Customer Knowledge Into Sales KnowledgeDocument3 pagesChap 13: Turning Customer Knowledge Into Sales KnowledgeHEM BANSALNo ratings yet
- Kufr Can Occur...Document2 pagesKufr Can Occur...TheEmigrantNo ratings yet
- Cultural Psychology ReviewerDocument16 pagesCultural Psychology ReviewerKen JaurigueNo ratings yet
- LongT5 PaperDocument13 pagesLongT5 PaperRaihanul Haque RahiNo ratings yet
- Reguladores de Voltaje 79xxDocument13 pagesReguladores de Voltaje 79xxJuan Angel Cerda GuerraNo ratings yet
- Tony Thrasher (Editor) - Emergency Psychiatry (PRIMER ON SERIES) - Oxford University Press (2023)Document537 pagesTony Thrasher (Editor) - Emergency Psychiatry (PRIMER ON SERIES) - Oxford University Press (2023)Stefan100% (1)
- Vocabulary + Grammar Unit 3 Test ADocument3 pagesVocabulary + Grammar Unit 3 Test AJoana FernandesNo ratings yet
- Eating Disorder PPT by Shreyasi MittalDocument35 pagesEating Disorder PPT by Shreyasi MittalPrachi gattaniNo ratings yet
- What Is COBIT ?: COBIT Is A Framework Created by ISACA For InformationDocument41 pagesWhat Is COBIT ?: COBIT Is A Framework Created by ISACA For Informationkarthigajana1850No ratings yet
- Gender EqualityDocument3 pagesGender Equalityrhea penarubia100% (1)
- Lesson 5: Freedom of The Human PersonDocument4 pagesLesson 5: Freedom of The Human PersonRhica Jhane IINo ratings yet
- Management by Objective (Mbo)Document24 pagesManagement by Objective (Mbo)crazypankaj100% (1)
- (Lesson2) Cultural, Social, and Political Institutions: Kinship, Marriage, and The HouseholdDocument5 pages(Lesson2) Cultural, Social, and Political Institutions: Kinship, Marriage, and The HouseholdPlat JusticeNo ratings yet
- Activity 5 Educational Philosophy Inventory: Revision Status: Revision Date: Recommending Approval: Concurred: ApprovedDocument2 pagesActivity 5 Educational Philosophy Inventory: Revision Status: Revision Date: Recommending Approval: Concurred: ApprovedErichIsnainNo ratings yet
- Okatse Canyon: Mások Ezeket Keresték MégDocument1 pageOkatse Canyon: Mások Ezeket Keresték Mégtom kemNo ratings yet
- Reading Circle 2 - Vocabulary EnricherDocument7 pagesReading Circle 2 - Vocabulary EnricherLee Jia XiNo ratings yet
- 1 s2.0 S0888327017305654 MainDocument10 pages1 s2.0 S0888327017305654 MainchinnavenkateswarluNo ratings yet
- Customizable Daily Growth PlanDocument12 pagesCustomizable Daily Growth PlanManojkumar Nair100% (1)
- Stricklin I WOULD NOT...Document17 pagesStricklin I WOULD NOT...Karl LammNo ratings yet
- Step 7 Err Code125936644Document37 pagesStep 7 Err Code125936644mohammadNo ratings yet
- Reading 10 Points: The Simpsons Is A Popular TV Programme About An AmericanDocument2 pagesReading 10 Points: The Simpsons Is A Popular TV Programme About An AmericanSofia PSNo ratings yet
- 16SEE - Schedule of PapersDocument36 pages16SEE - Schedule of PapersPiyush Jain0% (1)
- Quantitative Analysis of Carbohydrates by Nelson'S MethodDocument3 pagesQuantitative Analysis of Carbohydrates by Nelson'S MethodSeph CordovaNo ratings yet
- Astro GramaDocument4 pagesAstro GramageorgemihailNo ratings yet
- Jadual Alimah 2021.V3Document6 pagesJadual Alimah 2021.V3maryam cookNo ratings yet