Month________________
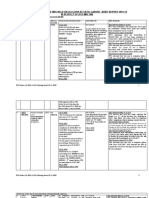
APPLICATION FORM FOR REIMBURSEMENT OF MEPDICAL CHARGES IN RESPECT OF
SERVING/RETIRED GOVERNMENT SERVANT AND HIS DEPENDENTS.
PART-A
1. Name, designation, BPS of the serving/retired Federal Government servant Alive/Deceased)
Rab Nawaz,
Inspector Inland Revenue (BPS-16) RTO Multan.
2. Name of the patient and relationship with the claimant as dependent, as specified in rule 2(d) of the
Federal Services Medical Attendance Rules, 1990.
Mrs. Shahnaz Begum (Wife)
______________________________________________________________________________________________
3. Diagnosis of the patient
Diabetic/Magrine/AVN
4. Ministry/Division/Department/Office of the serving/retired Government servant at S.No.1.
Ministry of Finance/Federal Board of Revenue/RTO Multan
5. Vendor No. and PPO No. For retired Government Servant __________________________N.A__________________
6. List of medicines with quantity/hospital bill/laboratory and other diagnostic charges etc. for which reimbursement is
claimed through this bill (format attached).
PART-B
Certificates by Government servant (or member of his family in case of deceased Government servant).
Certified that:i)
The member of my family for whose treatment reimbursement has been claimed is wholly dependent
upon me.
ii)
The claim was not drawn before.
iii)
I shall have no objection to the recovery of any amount overpaid, if any, from my pay/pension
or otherwise.
Signature ________________________________
FULL NAME OF THE GOVERNMENT SERVANT
or (claimant family member in case of deceased)
RAB NAWAZ
(in block letters)
Dated: ________________
CERTIFICATE BY THE AUTHORIZED MEDICAL ATTENDANT
Certified that the medicines/drugs/hospitalization/clinical tests/examinations listed below were essential for the
recovery and restoration of the patient, Shahnaz Begum W/o Rab Nawaz.
2.
It is further certified that neither the medicines/drugs etc. nor their effective substitutes could be supplied from the
hospital/dispensary.
Signature __________________________________
Designation ________________________________
Official Stamp ______________________________
COUNTERSIGNATURES
Departmental Controlling Authority
Hospital Authority
Signature __________________________________
Signature __________________________________
Designation ________________________________
Designation ________________________________
Official Stamp ______________________________
Official Stamp ______________________________
M.Haider Khan/M.Cla.
S.#
No. & Date of
Bill/Cash Memo
1
2
3
4
5
6
7
8
9
10
643 dt. 2-9-2014
Name of the Chemist
Shop/Hospital/Clinic/
Dispensary
Makkah Medicos, Multan
Name of Drugs/Medicines with
Quantity/Details of Tests etc.
Amount
Mixtrad Insulin
Tab. Viglip M 50/1000
Cap. Sibelium 5mg
Tab. Hitop 50mg
Cap. Celbex 200 mg
Tab. Neoprox 500mg
Cap. Tramal Plus
Cap. Sante 2mg
Tab. Carsel 50 mg.
BD Syring Insuline 1cc
1992/1440/750/596/960/828/882/356/109/150/-
TOTAL
(Rupees:
(04)
(60)
(60)
(30)
(60)
(90)
(60)
(30)
(30)
(10)
8063/-
Eight Thousand Sixty Three only )
Signature________________________
RAB NAWAZ
Inspector Inland Revenue, RTO Multan
(Full Name of the Government Servant)
M.Haider Khan/M.Cla.
S.#
No. & Date of
Bill/Cash Memo
Name
of
the
Chemist
Shop/Hospital/Clinic/Dispensary
Name
of
Drugs/Medicines with
Quantity/Details
of
Tests etc.
Amount
1
2
3
4
TOTAL
(Rupees
Signature________________________
MUHAMMAD MUZAFFAR KHAN LASHARI
(Full Name of the Government Servant
M.Haider Khan/M.Cla.
S.#
No. & Date of
Bill/Cash Memo
Name of the Chemist
Shop/Hospital/Clinic/Dispensary
Azmat Medical Store Multan.
No.3061 dated
23-05-2011
-do-
-do-
-do-
-do-
-do-
-do-
TOTAL
(Rupees Nine Thousand Six Hundred & Thirty only)
M.Haider Khan/M.Cla.
Name of
Drugs/Medicines with
Quantity/Details of
Tests etc.
02 Insulin Humalog
Plain.
01 Insulin Humalog 50
X 50
1 X 100 Dis.Syringes
ICC insolin 100
Teststrip Optium
Glucometer.
Amount
Rs.3,060/Rs.2,700/Rs.1,200/Rs.2,700/Rs.9,630/-
APPLICATION FORM FOR REIMBURSEMENT OF MEPDICAL CHARGES IN RESPECT OF
SERVING/RETIRED GOVERNMENT SERVANT AND HIS DEPENDENTS.
PART-A
1. Name, designation, BPS of the serving/retired Federal Government servant Alive/Deceased)
___________________________________________________________________________________________________
2. Name of the patient and relationship with the claimant as dependent, as specified in rule 2(d) of the
Federal Services Medical Attendance Rules, 1990.
_________________________________________________________________________________________________
3. Diagnosis of the patient _______________________
4. Ministry/Division/Department/Office of the serving/retired Government servant at S.No.1. RTO, MULTAN
_________________________________________________________________________________________________
5. Vendor No. and PPO No. For retired Government Servant ____________________________________________
6. List of medicines with quantity/hospital bill/laboratory and other diagnostic charges etc. for which reimbursement is
claimed through this bill (format attached).
PART-B
Certificates by Government servant (or member of his family in case of deceased Government servant).
Certified that:i)
The member of my family for whose treatment reimbursement has been claimed is wholly dependent
upon me.
ii)
The claim was not drawn before.
iv)
I shall have no objection to the recovery of any amount overpaid, if any, from my pay/pension
or otherwise.
Signature ________________________________
FULL NAME OF THE GOVERNMENT SERVANT
M.Haider Khan/M.Cla.
or (claimant family member in case of deceased)
_____________________________________
(IN BLOCK LETTERS)
Dated: ________________
CERTIFICATE BY THE AUTHORIZED MEDICAL ATTENDANT
Certified that the medicines/drugs/hospitalization/clinical tests/examinations listed below were essential for the
recovery and restoration of the patient, _______________________
2.
It is further certified that neither the medicines/drugs etc. nor their effective substitutes could be supplied from the
hospital/dispensary.
Signature __________________________________
Designation ________________________________
Official Stamp ______________________________
COUNTERSIGNATURES
Departmental Controlling Authority
Hospital Authority
Signature __________________________________
Signature __________________________________
Designation ________________________________
Designation ________________________________
Official Stamp ______________________________
Official Stamp ______________________________
M.Haider Khan/M.Cla.
You might also like
- Hospital Planning and DesigningDocument132 pagesHospital Planning and DesigningViky Singh50% (2)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
- Analysis of Health City Cayman IslandsDocument4 pagesAnalysis of Health City Cayman IslandsRitika Sharma100% (1)
- Letting Go by Atul GawandeDocument18 pagesLetting Go by Atul Gawandetakoyakilovers100% (2)
- Email Ids of Purchase Managers Andgeneral Managers For Hospitals in BangaloreDocument79 pagesEmail Ids of Purchase Managers Andgeneral Managers For Hospitals in BangalorePawan KinnalNo ratings yet
- Form of Essentiality Certificate B PDFDocument2 pagesForm of Essentiality Certificate B PDFAnji KaringuNo ratings yet
- FMLA Blank FormDocument4 pagesFMLA Blank FormAndy WilsonNo ratings yet
- CSC FORM 41 Med.Document5 pagesCSC FORM 41 Med.editha salahayNo ratings yet
- 02 D Joint Affidavit UndertakingDocument1 page02 D Joint Affidavit UndertakingTony DawaNo ratings yet
- Joint Affidavit of UndertakingDocument1 pageJoint Affidavit of UndertakingKeyn TejadaNo ratings yet
- PHM MediSavers 2015 BrochureDocument4 pagesPHM MediSavers 2015 BrochureNazim SalehNo ratings yet
- Field Trip Report To UTHM Health CentreDocument2 pagesField Trip Report To UTHM Health CentreAkmal Zharif100% (1)
- Medical FormDocument3 pagesMedical FormTahir HussainNo ratings yet
- Medical ProformaDocument2 pagesMedical ProformaKaleemUddinNo ratings yet
- Medical Proforma Latest 1Document2 pagesMedical Proforma Latest 1beastbaloch12345No ratings yet
- Medical Reimbursement FormDocument2 pagesMedical Reimbursement FormMEMOONA ASHARNo ratings yet
- Application Med. Re-ImbDocument2 pagesApplication Med. Re-Imbzahid hussainNo ratings yet
- FormsDocument31 pagesFormsSuvam Sinha100% (1)
- Emlpyees Application Form MAR-3Document1 pageEmlpyees Application Form MAR-3Muhammad ShoaibNo ratings yet
- 1582808855278-Reimbursement FormDocument14 pages1582808855278-Reimbursement FormSuresh MeenaNo ratings yet
- Application FormDocument1 pageApplication FormAglaia OrtileNo ratings yet
- Surety BondDocument1 pageSurety Bondshahafridi017No ratings yet
- Notification of Claim - Prudential GuaranteeDocument2 pagesNotification of Claim - Prudential GuaranteeZen Catolico ErumNo ratings yet
- COHP FamilyDocument4 pagesCOHP FamilyAbigail Aracely Ochoa AlvaradoNo ratings yet
- Checklist of Requirements For Hospital Accreditation (Secondary)Document4 pagesChecklist of Requirements For Hospital Accreditation (Secondary)pamgelNo ratings yet
- Form of Essentiality Certificate BDocument2 pagesForm of Essentiality Certificate BSantosh Kori50% (2)
- Signature/thumb Impression of Person Whose Examination Has Been Conducted or Guardian (In Case Victim Is Minor, Relation, Student, Insane)Document8 pagesSignature/thumb Impression of Person Whose Examination Has Been Conducted or Guardian (In Case Victim Is Minor, Relation, Student, Insane)Joy SinghNo ratings yet
- Affidavit of Continous ComplianceDocument1 pageAffidavit of Continous ComplianceRocky MontañerNo ratings yet
- Refusal FormDocument1 pageRefusal FormViral Chann3LNo ratings yet
- FORM - (FMLA) FAMILY HealthDocument3 pagesFORM - (FMLA) FAMILY HealthRavi SankarNo ratings yet
- Proforma For Claiming Refund of Medical Expenses - 1 - Split - 1Document5 pagesProforma For Claiming Refund of Medical Expenses - 1 - Split - 1Ajay SinglaNo ratings yet
- FORM 4 (See Rules 19) Medical Certificate For Non-Gazetted Officers Recommended Leave or Extension of Leave or Commutation of LeaveDocument1 pageFORM 4 (See Rules 19) Medical Certificate For Non-Gazetted Officers Recommended Leave or Extension of Leave or Commutation of LeaveSaurabh Singraore100% (1)
- Medical Certificate: C.S. FORM No. 41Document1 pageMedical Certificate: C.S. FORM No. 41adoriza0218No ratings yet
- Bsnlmrs FormsDocument5 pagesBsnlmrs FormsdurgendraNo ratings yet
- Medical Certificate (Form 41)Document1 pageMedical Certificate (Form 41)Nasra AbdulganiNo ratings yet
- CSC Form41Document1 pageCSC Form41Epifanio AranezNo ratings yet
- Records ReleaseDocument1 pageRecords ReleasechelseaNo ratings yet
- Denr Application For Agricultural Free PatentDocument3 pagesDenr Application For Agricultural Free PatentAngelica Dulce100% (1)
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- Daycare Treatment FormDocument2 pagesDaycare Treatment FormBineesh TNo ratings yet
- TH STDocument1 pageTH STDeepakIkharNo ratings yet
- 3 VSR Updated Form (6-3-2021) 2Document5 pages3 VSR Updated Form (6-3-2021) 2Zeeshan KhanNo ratings yet
- New Leave Form 2020 ProgramDocument2 pagesNew Leave Form 2020 ProgramMarife TremedalNo ratings yet
- Annex A RR 11-2018Document1 pageAnnex A RR 11-2018Reegan MasarateNo ratings yet
- Application For Leave - HRHDocument1 pageApplication For Leave - HRHJepoi ClementeNo ratings yet
- FORM 41 Medical CertificateDocument1 pageFORM 41 Medical CertificateWANNA CABALLERONo ratings yet
- Annexure II - Medical Fitness Form - 2020 22 - 20 MayDocument1 pageAnnexure II - Medical Fitness Form - 2020 22 - 20 MayAgrim RawatNo ratings yet
- Medical Reimbursement Form 2Document2 pagesMedical Reimbursement Form 2Rakesh KumarNo ratings yet
- Mediclaim FormDocument1 pageMediclaim Formpicrush2pmNo ratings yet
- Authorization-Consent FormDocument1 pageAuthorization-Consent FormValeria HannahNo ratings yet
- 02 D Joint Affidavit UndertakingDocument1 page02 D Joint Affidavit UndertakingStella MaghanoyNo ratings yet
- 02 D Joint Affidavit UndertakingDocument1 page02 D Joint Affidavit UndertakingPPHNo ratings yet
- 02 DJoint Affidavit UndertakingDocument1 page02 DJoint Affidavit UndertakingCarmxNo ratings yet
- U.S. Department of Labor Wage and Hour Division Certification of Health Care Provider For Employee's Serious Health Condition Under The Family and Medical Leave ActDocument4 pagesU.S. Department of Labor Wage and Hour Division Certification of Health Care Provider For Employee's Serious Health Condition Under The Family and Medical Leave Actstawberry shortcakeNo ratings yet
- WH 380 eDocument4 pagesWH 380 ePor Justica EN YumaNo ratings yet
- Medical InformationDocument1 pageMedical InformationfaithchurchyouthNo ratings yet
- Hospital Discharge Summary Form InstructionsDocument2 pagesHospital Discharge Summary Form Instructionsepi bahoNo ratings yet
- Medical Leave FormatsDocument1 pageMedical Leave FormatsAdara deep100% (1)
- Cscform41 1Document1 pageCscform41 1Mica AlcazarNo ratings yet
- Rockford Rec Emergency Medical FormDocument2 pagesRockford Rec Emergency Medical FormRyan ThompsonNo ratings yet
- CS Form 41 NTCDocument2 pagesCS Form 41 NTCneriNo ratings yet
- Proforma For Claiming Refund of Medical Expenses - 1 - Split - 2Document2 pagesProforma For Claiming Refund of Medical Expenses - 1 - Split - 2ajayNo ratings yet
- For Muli R Claim RJ Individ U FinalDocument1 pageFor Muli R Claim RJ Individ U FinalSuhendin SoehendinNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Slip 0232 01 2019Document513 pagesSlip 0232 01 2019Shahaan ZulfiqarNo ratings yet
- S 0232 01Document50 pagesS 0232 01Shahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument6 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- NO Marriage CertificateDocument5 pagesNO Marriage CertificateShahaan ZulfiqarNo ratings yet
- Para NO Cases Under Process Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and VerifiedDocument6 pagesPara NO Cases Under Process Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and VerifiedShahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument7 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument6 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- Drra 12Document966 pagesDrra 12Shahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument5 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument7 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- 114 CasesDocument29 pages114 CasesShahaan ZulfiqarNo ratings yet
- Para No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedDocument6 pagesPara No Amount Pointed Out by Audit Amount Charged But Not Recovered Amount Recovered and Verified Amount Recovered But Un-VerifiedShahaan ZulfiqarNo ratings yet
- 2013-14 - Multan 25112019Document47 pages2013-14 - Multan 25112019Shahaan ZulfiqarNo ratings yet
- 2017-18 - 17.08.2020 Multan Audit ReportDocument25 pages2017-18 - 17.08.2020 Multan Audit ReportShahaan ZulfiqarNo ratings yet
- 2011-12 - Dac 14.01.2020Document38 pages2011-12 - Dac 14.01.2020Shahaan ZulfiqarNo ratings yet
- RN-BSN ResumeDocument2 pagesRN-BSN Resumeapi-405284134No ratings yet
- C4 Swimming Carnval 2020 PDFDocument1 pageC4 Swimming Carnval 2020 PDFjonNo ratings yet
- Misappropriation: A. Slander B. LibelDocument3 pagesMisappropriation: A. Slander B. Libelrica sebabillonesNo ratings yet
- Comp 01 Instructor ManualDocument54 pagesComp 01 Instructor ManualP D SpencerNo ratings yet
- Lexie ResumeDocument1 pageLexie ResumeLexie VigilNo ratings yet
- Sulfa Nil Amide Deaths of 1937Document4 pagesSulfa Nil Amide Deaths of 1937api-3810976No ratings yet
- Teks Presentasi Maju BeDocument3 pagesTeks Presentasi Maju BeGita FitrisiaNo ratings yet
- Statement Dated 2023-05-10Document13 pagesStatement Dated 2023-05-10Logan casillasNo ratings yet
- CV April 1Document2 pagesCV April 1api-281813422No ratings yet
- Healthcare Facility Department Manager Director in Portland OR Resume Glyndon Ruth KimbroughDocument2 pagesHealthcare Facility Department Manager Director in Portland OR Resume Glyndon Ruth KimbroughGlyndonRuthKimbroughNo ratings yet
- ALL Filipinos Are Covered: National Health Insurance Program (NHIP)Document3 pagesALL Filipinos Are Covered: National Health Insurance Program (NHIP)Ei Ar TaradjiNo ratings yet
- HAM ReportDocument25 pagesHAM ReportljmacabeoNo ratings yet
- Exhibitor ListDocument9 pagesExhibitor ListflinstonesNo ratings yet
- 2018 03 01 - An Introduction To LOINCDocument59 pages2018 03 01 - An Introduction To LOINCDaniel VreemanNo ratings yet
- All India Network Hospitals GeneralDocument480 pagesAll India Network Hospitals Generalshiva lakshmiNo ratings yet
- Indian Wound Care Market Overview Morulaa HealthTechDocument1 pageIndian Wound Care Market Overview Morulaa HealthTechSakshi KhuranaNo ratings yet
- MEDICARD PHILIPPINES, INC VS. Commissioner of Internal Revenue (GR NO. 222743) April 5, 2017Document24 pagesMEDICARD PHILIPPINES, INC VS. Commissioner of Internal Revenue (GR NO. 222743) April 5, 2017Emil BautistaNo ratings yet
- CMAM Community Based Management ofDocument18 pagesCMAM Community Based Management ofZia BalochNo ratings yet
- 5.casts and MoldsDocument30 pages5.casts and MoldsKatrina PonceNo ratings yet
- Drug Fridge - Cleaning Procedure: WCDHB-PN-0061Document2 pagesDrug Fridge - Cleaning Procedure: WCDHB-PN-0061Rika VerdikaNo ratings yet
- Commercial Dispatch Eedition 8-7-20Document12 pagesCommercial Dispatch Eedition 8-7-20The DispatchNo ratings yet
- Access Florida Application Details 657026137Document5 pagesAccess Florida Application Details 657026137James WashingtonNo ratings yet
- Aidet FinalDocument11 pagesAidet Finalapi-273608948100% (1)
- DamaDocument2 pagesDamajerimiah_manzon100% (1)