Download as pdf or txt
You might also like
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDocument5 pagesHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriNo ratings yet
- THE EIGHT PRINCIPLES OF TAI CHI CHUAN - Energy Arts - Learn Tai (PDFDrive - Com) (1) 8885162263945383523 PDFDocument47 pagesTHE EIGHT PRINCIPLES OF TAI CHI CHUAN - Energy Arts - Learn Tai (PDFDrive - Com) (1) 8885162263945383523 PDFTakis Abatzopoulos100% (1)
- ACCP - Comprehensive Medication Management in Team-Based CareDocument8 pagesACCP - Comprehensive Medication Management in Team-Based CareThuane SalesNo ratings yet
- GastroenteritisDocument29 pagesGastroenteritisKatherine 'Chingboo' Leonico Laud100% (8)
- Journal Casereport 1Document5 pagesJournal Casereport 1Arif MohammadNo ratings yet
- Shin2016 Retinal Pigment Epithelium Wound Healing After Traumatic Choroidal RuptureDocument5 pagesShin2016 Retinal Pigment Epithelium Wound Healing After Traumatic Choroidal RuptureMilzan MurtadhaNo ratings yet
- Behcet DiseaseDocument6 pagesBehcet DiseasejbahalkehNo ratings yet
- Spectral-Domain Optical Coherence Tomographic Findings at Each Stage of Punctate Inner Choroidopathy Zhang2013Document6 pagesSpectral-Domain Optical Coherence Tomographic Findings at Each Stage of Punctate Inner Choroidopathy Zhang2013kubi.ilskiNo ratings yet
- Laporan Kasus NeurooftalmologiDocument12 pagesLaporan Kasus NeurooftalmologiPradistya Syifa YudiasariNo ratings yet
- 2023 Article 32184Document10 pages2023 Article 32184Diana TricoracheNo ratings yet
- Alsberg 1 s2.0 S2451993621002279 MainDocument5 pagesAlsberg 1 s2.0 S2451993621002279 MainDoug PulaNo ratings yet
- Orbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusDocument4 pagesOrbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusYosiita KartinaaNo ratings yet
- EED Uveitis 4 Get - FileDocument3 pagesEED Uveitis 4 Get - FileAmirahShalehaNo ratings yet
- Ophthal Notes PGDocument6 pagesOphthal Notes PGSwati TyagiNo ratings yet
- Ni Hms 12505Document10 pagesNi Hms 12505noorhadi.n10No ratings yet
- A Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeDocument3 pagesA Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeSriana K. LaliyoNo ratings yet
- Moon2019 PDFDocument7 pagesMoon2019 PDFGusti Zidni FahmiNo ratings yet
- Parade Wspos Tipe 2Document3 pagesParade Wspos Tipe 2irwan_201291No ratings yet
- Masquerade SyndromesDocument10 pagesMasquerade Syndromestony_chrisNo ratings yet
- Esferofauia Aislada y GlaucomaDocument3 pagesEsferofauia Aislada y GlaucomaManuel VasquezNo ratings yet
- Classification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic ChangeDocument26 pagesClassification of Visual Field Abnormalities in Highly Myopic Eyes Without Pathologic Change钟华No ratings yet
- Herpes Zoster OphthalmicusDocument12 pagesHerpes Zoster OphthalmicusGio Vano NaihonamNo ratings yet
- Choroidal and Retinal Thickening in Severe Preeclampsia: RetinaDocument7 pagesChoroidal and Retinal Thickening in Severe Preeclampsia: RetinaAssifa RidzkiNo ratings yet
- Sympathetic Ophthalmia After Vitreoretinal Surgery: A Report of Two CasesDocument11 pagesSympathetic Ophthalmia After Vitreoretinal Surgery: A Report of Two CasesAlexander RezaNo ratings yet
- The Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanDocument6 pagesThe Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanNurul Falah KalokoNo ratings yet
- Neuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientDocument6 pagesNeuroretinitis Syphilis in Human Immunodeficiency Virus-Infected PatientAnindya AgrasidiNo ratings yet
- PIIS0002939422003890Document9 pagesPIIS0002939422003890Anca Florina GaceaNo ratings yet
- Neurosyphilis Masquerading As An Acute Adie's Tonic Pupil: Report of A CaseDocument6 pagesNeurosyphilis Masquerading As An Acute Adie's Tonic Pupil: Report of A CaseOlvaria MisfaNo ratings yet
- Francisco Trincão, João Feijão, Vítor Maduro, Nuno Alves, Carlos Batalha, Pedro Candelária, José Pita-NegrãoDocument1 pageFrancisco Trincão, João Feijão, Vítor Maduro, Nuno Alves, Carlos Batalha, Pedro Candelária, José Pita-NegrãoVitor MaduroNo ratings yet
- Pi Is 0161642022006923Document12 pagesPi Is 0161642022006923Anca Florina GaceaNo ratings yet
- The Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c MiceDocument12 pagesThe Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c Miceracut_khansatraNo ratings yet
- Bilateral Congenital Toxoplasmosis Complicated by Choroidal Neo-Vessels A Case ReportDocument3 pagesBilateral Congenital Toxoplasmosis Complicated by Choroidal Neo-Vessels A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Staphylococcus Epidermidis End PDFDocument4 pagesStaphylococcus Epidermidis End PDFNisaNo ratings yet
- Steptoe Et Al. - 2020 - Evolving Longitudinal Retinal Observations in A CoDocument9 pagesSteptoe Et Al. - 2020 - Evolving Longitudinal Retinal Observations in A Copaul steptoeNo ratings yet
- BR J Ophthalmol-2014-Chan-79-81 PDFDocument4 pagesBR J Ophthalmol-2014-Chan-79-81 PDFRomi Mauliza FauziNo ratings yet
- 1 s2.0 S1350946217300599 MainDocument15 pages1 s2.0 S1350946217300599 MainPatricia RodriguesNo ratings yet
- Case Report Diabetic Retinopaty in EnglishDocument13 pagesCase Report Diabetic Retinopaty in Englishsasha anka DilanNo ratings yet
- American Journal of Ophthalmology Case ReportsDocument3 pagesAmerican Journal of Ophthalmology Case ReportsElison Jaya PanggaloNo ratings yet
- Acute Retinal Necrosis Following Contralateral Herpes Zoster OphthalmicusDocument4 pagesAcute Retinal Necrosis Following Contralateral Herpes Zoster Ophthalmicusnurul_sharaswatiNo ratings yet
- Granuloma Epididimitisarticle-2Document4 pagesGranuloma Epididimitisarticle-2Feby Kurnia PutriNo ratings yet
- Management of Double-Penetrating Ocular Injury With Retained Intraorbital Metallic Foreign BodyDocument4 pagesManagement of Double-Penetrating Ocular Injury With Retained Intraorbital Metallic Foreign BodyShirakawa AlmiraNo ratings yet
- Bjophthalmol 2019 315520.fullDocument5 pagesBjophthalmol 2019 315520.fullRemNo ratings yet
- Management of Submacula Bleeding With Pneumatic DisplacementDocument8 pagesManagement of Submacula Bleeding With Pneumatic DisplacementNaufal Hilmi MarzuqNo ratings yet
- Is Episcleritis Associated To Glaucoma?Document3 pagesIs Episcleritis Associated To Glaucoma?Alvin JulianNo ratings yet
- 1600-Article Text-5930-1-10-20231002Document12 pages1600-Article Text-5930-1-10-20231002Yunisa astiaraniNo ratings yet
- 100152-Article Text-841-1-10-20210226Document5 pages100152-Article Text-841-1-10-20210226Rachel DenonaNo ratings yet
- Faure 2017Document8 pagesFaure 2017zazaza94No ratings yet
- Tonic Pupil and Corneal Anesthesia After Vitrectomy and Encircling Band For Retinal Detachment in An Ex-Premature ChildDocument5 pagesTonic Pupil and Corneal Anesthesia After Vitrectomy and Encircling Band For Retinal Detachment in An Ex-Premature ChildOlvaria MisfaNo ratings yet
- Opth 9 1041Document7 pagesOpth 9 1041petrarizkyNo ratings yet
- Tumor OrbitaDocument4 pagesTumor OrbitaIda Bagus Deny PrayudiNo ratings yet
- Ojoph 2022111815222395Document12 pagesOjoph 2022111815222395budi rahmawatiNo ratings yet
- None 3Document11 pagesNone 3Yehiel FlaviusNo ratings yet
- White Dot Syndromes Harvey S. Uy, M.DDocument11 pagesWhite Dot Syndromes Harvey S. Uy, M.DShimaa MersalNo ratings yet
- Rapidly Progressive Severe Proptosis Esthesioneuroblastoma Case ReportDocument5 pagesRapidly Progressive Severe Proptosis Esthesioneuroblastoma Case ReportSSR-IIJLS JournalNo ratings yet
- Perilimbal Conjunctival Pigmentation in Chinese Patients With Vernal KeratoconjunctivitisDocument4 pagesPerilimbal Conjunctival Pigmentation in Chinese Patients With Vernal KeratoconjunctivitisDwi HardiyantiNo ratings yet
- Highlights in Neuro OphthalmologyDocument2 pagesHighlights in Neuro OphthalmologyShruthi VMNo ratings yet
- Jurnal Mata 5Document6 pagesJurnal Mata 5Dahru KinanggaNo ratings yet
- Journal Pre-Proof: Annals of Medicine and SurgeryDocument23 pagesJournal Pre-Proof: Annals of Medicine and SurgeryDaniel GuevaraNo ratings yet
- Retinal Pigment Epithelium Tear in VKH DiseaseDocument3 pagesRetinal Pigment Epithelium Tear in VKH DiseasePhilip McNelsonNo ratings yet
- Retina 39 426Document9 pagesRetina 39 426ryaalwiNo ratings yet
- IndianJOphthalmol632164-4403297 121352Document3 pagesIndianJOphthalmol632164-4403297 121352Mohammad Abdullah BawtagNo ratings yet
- Fungal Keratitis and Ocular Surface Squamous Neoplasia in A HIV Positive PatientDocument4 pagesFungal Keratitis and Ocular Surface Squamous Neoplasia in A HIV Positive PatientSherly AsrianiNo ratings yet
- Ijeb 48 (7) 642-650Document9 pagesIjeb 48 (7) 642-650dedypurnamaNo ratings yet
- Intoxication GuidelinesDocument3 pagesIntoxication GuidelinesdedypurnamaNo ratings yet
- Special TopicDocument7 pagesSpecial TopicdedypurnamaNo ratings yet
- (Melastoma Malabathricum L.), Moist Exposed Burn Ointment (MEBO) andDocument2 pages(Melastoma Malabathricum L.), Moist Exposed Burn Ointment (MEBO) anddedypurnamaNo ratings yet
- A Toolkit For Women's Empowerment and Leadership in Health and WelfareDocument56 pagesA Toolkit For Women's Empowerment and Leadership in Health and WelfarededypurnamaNo ratings yet
- Corneal Transplantation at An Ophthalmological Referral Center in Colombia: Indications and Techniques (2004-2011)Document4 pagesCorneal Transplantation at An Ophthalmological Referral Center in Colombia: Indications and Techniques (2004-2011)dedypurnamaNo ratings yet
- Refractive Surgery: The Never Ending Task of Improving Vision CorrectionDocument2 pagesRefractive Surgery: The Never Ending Task of Improving Vision CorrectiondedypurnamaNo ratings yet
- Pharma ExamDocument10 pagesPharma Examteabagman0% (1)
- Smart Sensor 4 Gases AS8900 - Manual de OperaçãoDocument12 pagesSmart Sensor 4 Gases AS8900 - Manual de OperaçãoRogerioPascualNo ratings yet
- Nasopharyngeal Carcinoma in Children and AdolescentsDocument5 pagesNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahNo ratings yet
- Famco Important ChaptersDocument7 pagesFamco Important ChaptersFiryal BalushiNo ratings yet
- Details of NACO Supported Blood BanksDocument2 pagesDetails of NACO Supported Blood BanksRajeev SinghNo ratings yet
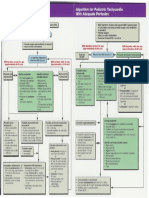
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Msds Guano DiscsDocument5 pagesMsds Guano Discsapi-289433849No ratings yet
- Top Dental Schools - Admission RequirementsDocument10 pagesTop Dental Schools - Admission RequirementsDental school admission0% (1)
- A Hands-On Guide For Essbase Report ScriptDocument9 pagesA Hands-On Guide For Essbase Report ScriptAmit SharmaNo ratings yet
- Hindu Ast.Document418 pagesHindu Ast.ANANTHPADMANABHAN100% (1)
- Spectrum - Bone Densitometry WOrkshopDocument16 pagesSpectrum - Bone Densitometry WOrkshopanbufelix1939No ratings yet
- Aitecs 3017 DATASHEETDocument2 pagesAitecs 3017 DATASHEETJose Antonio Diaz FierrezNo ratings yet
- Đề Thi Vào 10 Chuyên Anh Đáp Án ĐỀ THI THỬ LẦNDocument7 pagesĐề Thi Vào 10 Chuyên Anh Đáp Án ĐỀ THI THỬ LẦNVân OriNo ratings yet
- Changes in PregnancyDocument13 pagesChanges in PregnancyZarlyn MirafloresNo ratings yet
- ADRnewReporting Form 1.4Document2 pagesADRnewReporting Form 1.4Sourabh kundara50% (2)
- Aroma TherapyDocument14 pagesAroma Therapysandhyapanicker1988No ratings yet
- AGS 2023 BEERS PocketDocument9 pagesAGS 2023 BEERS Pocketerika avelina rodriguez jaureguiNo ratings yet
- JACKSON V AEGLive April 30th RICHARD SENEFF/ Martinez DetectiveDocument208 pagesJACKSON V AEGLive April 30th RICHARD SENEFF/ Martinez DetectiveTeamMichael100% (1)
- Rice Bran Healthy OilDocument25 pagesRice Bran Healthy OilMusheer BashaNo ratings yet
- Digestion Enzyme Practice TestDocument15 pagesDigestion Enzyme Practice TestJila HafiziNo ratings yet
- Iksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewDocument6 pagesIksir-e-Badan (Elixir) : Unique Influence From Unani Medicine - A ReviewAmjad NaseerNo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- Critical Care EnvironmentDocument16 pagesCritical Care EnvironmentJeffrey KauvaNo ratings yet
- Pharmacology Connections To Nursing Practice 3rd Edition Adams Test Bank 1Document32 pagesPharmacology Connections To Nursing Practice 3rd Edition Adams Test Bank 1matthew100% (57)
- Management of Cutaneous ErythrasmaDocument11 pagesManagement of Cutaneous ErythrasmaDesi RatnaningtyasNo ratings yet
- SAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaDocument25 pagesSAI's vs. STD'S: - Syphilis - Chlamydia - Vaginitis - Herpes - GonnorheaMark CheneyNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet