Download as pdf or txt
You might also like
- Hypokalemia Nursing Care PlanDocument2 pagesHypokalemia Nursing Care PlanCyrus De Asis92% (36)
- Test Bank For Williams Essentials of Nutrition and Diet Therapy 12th Edition Eleanor Schlenker Joyce Ann GilbertDocument11 pagesTest Bank For Williams Essentials of Nutrition and Diet Therapy 12th Edition Eleanor Schlenker Joyce Ann Gilbertdennisgallegosmkrgyabsod100% (20)
- Live NCLEX Review Lecture Slides-2Document510 pagesLive NCLEX Review Lecture Slides-2Ronny Andres Carrasco100% (10)
- Cardiac Drugs Study Guide CourseDocument19 pagesCardiac Drugs Study Guide CourseAmanda Brittain100% (6)
- Preformulation Study of Moxifloxacin Hydrochloride 2Document20 pagesPreformulation Study of Moxifloxacin Hydrochloride 2زياد سلمانNo ratings yet
- Refeeding Syndome GuidelineDocument31 pagesRefeeding Syndome GuidelineFidya ArdinyNo ratings yet
- Potassium Liquiuv: (Ref) (Control)Document1 pagePotassium Liquiuv: (Ref) (Control)MaherNo ratings yet
- KetoconazoleDocument9 pagesKetoconazolePradeep BhimaneniNo ratings yet
- Cyclophosphamide For Injection, USPDocument2 pagesCyclophosphamide For Injection, USPemilia candraNo ratings yet
- Analgesic OintmentDocument3 pagesAnalgesic OintmentTim BorjaNo ratings yet
- Prep. BUROW'S SOLUTIONDocument1 pagePrep. BUROW'S SOLUTIONJoanna Carla Marmonejo Estorninos-Walker100% (1)
- Case Study 1 (Muscular) - ALSDocument5 pagesCase Study 1 (Muscular) - ALSSamantha AquinoNo ratings yet
- HomatropinDocument11 pagesHomatropinDesma ParayuNo ratings yet
- Aluminum HydroxideDocument3 pagesAluminum HydroxidemrkrlndNo ratings yet
- LantusDocument1 pageLantusSandrine BarredoNo ratings yet
- Jurnal Elbow Manual Therapy For Aging & Older AdultsDocument7 pagesJurnal Elbow Manual Therapy For Aging & Older AdultsKyoNo ratings yet
- Analgesic OintmentDocument1 pageAnalgesic OintmentLorenNo ratings yet
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Linezolid: Antibiotic ClassDocument2 pagesLinezolid: Antibiotic ClassEdison Patricio Vallejo PasquelNo ratings yet
- 3B Drug Study 2Document23 pages3B Drug Study 2Kristine Dela CruzNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- Drug Study (Pedia)Document7 pagesDrug Study (Pedia)Caurrine Monsalud100% (1)
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- TelfastDocument3 pagesTelfastjbahalkehNo ratings yet
- The Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016Document10 pagesThe Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016ddandan_2No ratings yet
- Monsalud - Drug StudyDocument5 pagesMonsalud - Drug StudyJanielle Christine MonsaludNo ratings yet
- Morphine (Astramorph)Document1 pageMorphine (Astramorph)Adrianne BazoNo ratings yet
- Lovastatin PDFDocument3 pagesLovastatin PDFHannaNo ratings yet
- Triamcinolone (Topical) - Drug InformationDocument5 pagesTriamcinolone (Topical) - Drug InformationMauricio Sv0% (1)
- What Is Alkaptonuria? Highlights: SymptomsDocument4 pagesWhat Is Alkaptonuria? Highlights: SymptomsJustin PerezNo ratings yet
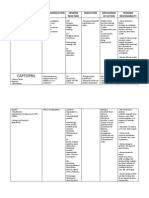
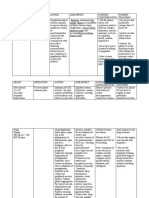
- Amlodipine Captopril MetronidazoleDocument5 pagesAmlodipine Captopril Metronidazolekhrysty1506No ratings yet
- Adults and Children 15 Y Pediatric 6 - 14 YDocument2 pagesAdults and Children 15 Y Pediatric 6 - 14 YFildehl Janice Bomediano Catipay100% (1)
- Anti-Anemic Drugs - 210619200800Document40 pagesAnti-Anemic Drugs - 210619200800Yohannes MeridNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- Drug StudyDocument7 pagesDrug Studyanne009No ratings yet
- Drug StudyDocument7 pagesDrug StudyCharm LorenzoNo ratings yet
- Zinc OxideDocument4 pagesZinc OxideyundayundaaNo ratings yet
- Antiviral DrugsDocument56 pagesAntiviral DrugsciccianoNo ratings yet
- Pathophysiology of Peptic Ulcer DiseaseDocument1 pagePathophysiology of Peptic Ulcer DiseaseJhade RelletaNo ratings yet
- The Child With Hematologic DisordersDocument149 pagesThe Child With Hematologic DisordersNics FranciscoNo ratings yet
- Brand Name: Generic Name: Drug ClassificationDocument2 pagesBrand Name: Generic Name: Drug ClassificationChristine Pialan SalimbagatNo ratings yet
- DRUGSDocument5 pagesDRUGSDanica EspejoNo ratings yet
- Intake & Output Monitoring Sheet: 11 PM 11-7 1000 ML 0 550 ML 0 0Document2 pagesIntake & Output Monitoring Sheet: 11 PM 11-7 1000 ML 0 550 ML 0 0Renea Joy ArruejoNo ratings yet
- Resurrection University Medication CardDocument2 pagesResurrection University Medication CardBohung ConNo ratings yet
- ORS Package InsertDocument1 pageORS Package InsertwhothehellisarcticmonkeysNo ratings yet
- Ferrous SulfateDocument2 pagesFerrous SulfateKylahNo ratings yet
- VincristineDocument2 pagesVincristineBigBoostingNo ratings yet
- Module 3 Activity 2 Drug Study Ciprofloxacin PaxilDocument6 pagesModule 3 Activity 2 Drug Study Ciprofloxacin PaxilEugene MananganNo ratings yet
- ChlorhexidineDocument11 pagesChlorhexidineDienNguyen100% (1)
- CEPHALOSPORINSDocument18 pagesCEPHALOSPORINSVikas SharmaNo ratings yet
- Antimalarial DrugsDocument7 pagesAntimalarial DrugsHilmanNo ratings yet
- Timolol Maleate Pilocarpine HCLDocument21 pagesTimolol Maleate Pilocarpine HCLapi-414913553100% (1)
- Oral Rehydration SolutionDocument4 pagesOral Rehydration SolutionMomerNo ratings yet
- Clarithromycin & AvamysDocument1 pageClarithromycin & AvamysSandrine BarredoNo ratings yet
- Warfarin Mechanism of ActionDocument7 pagesWarfarin Mechanism of ActionIna GrigorasNo ratings yet
- Pharmacologic Management: BleomycinDocument1 pagePharmacologic Management: BleomycinKim ApuradoNo ratings yet
- VancomycinDocument2 pagesVancomycinxoxo318No ratings yet
- Dextrose 50 InjectionDocument6 pagesDextrose 50 InjectionLip StickNo ratings yet
- CyclophosphamideDocument2 pagesCyclophosphamideksumanpharma8801No ratings yet
- DrugDocument3 pagesDrugPeace Andong PerochoNo ratings yet
- Drugs and NCPDocument4 pagesDrugs and NCPApril Anne CostalesNo ratings yet
- ISONIAZIDDocument2 pagesISONIAZIDPoet POet PoEtNo ratings yet
- Adults, Elderly and Children Over 1 YearDocument7 pagesAdults, Elderly and Children Over 1 YeardindaikaputriNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Pediatric Drug ReferenceDocument86 pagesPediatric Drug Referenceromaine_as100% (1)
- AntidotesDocument36 pagesAntidotesMohamed Haggag100% (1)
- Hfo 2Document9 pagesHfo 2markus_danusantosoNo ratings yet
- Turvallinen Koti Lapselle enDocument24 pagesTurvallinen Koti Lapselle enmarkus_danusantosoNo ratings yet
- Hfo 3Document8 pagesHfo 3markus_danusantosoNo ratings yet
- The Complete Guide To Baby CarryingDocument6 pagesThe Complete Guide To Baby Carryingmarkus_danusantosoNo ratings yet
- Baby SlingDocument20 pagesBaby Slingmarkus_danusantosoNo ratings yet
- HFO - WikipediaDocument4 pagesHFO - Wikipediamarkus_danusantosoNo ratings yet
- HIE - ImagingDocument73 pagesHIE - Imagingmarkus_danusantosoNo ratings yet
- BPD - DART Regiment DexamethasoneDocument4 pagesBPD - DART Regiment Dexamethasonemarkus_danusantosoNo ratings yet
- Resuscitation - NeopuffDocument11 pagesResuscitation - Neopuffmarkus_danusantosoNo ratings yet
- Resuscitation - AdvancedDocument17 pagesResuscitation - Advancedmarkus_danusantosoNo ratings yet
- List of ParticipantsDocument7 pagesList of Participantsmarkus_danusantosoNo ratings yet
- DRUG StudyDocument43 pagesDRUG StudyNathalie Faith CotengNo ratings yet
- Medical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesDocument20 pagesMedical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesBlanca Herrera MoralesNo ratings yet
- ELECTROLYTESDocument8 pagesELECTROLYTESvarshith gandlaNo ratings yet
- 04.06.2018 - 5 - M. Zerafa - Fluid and Electrolyte PhysiologyDocument20 pages04.06.2018 - 5 - M. Zerafa - Fluid and Electrolyte PhysiologyPhilippe KinnaerNo ratings yet
- Fluids Electrolytes - Acid-Base BalanceDocument11 pagesFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (2)
- CP Acute Renal Failure Chap7Document128 pagesCP Acute Renal Failure Chap7Katherine 'Chingboo' Leonico LaudNo ratings yet
- Fluid and Electrolyte MCQSDocument55 pagesFluid and Electrolyte MCQSAshraf ShalbiNo ratings yet
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedNo ratings yet
- AdvorDocument11 pagesAdvorJuan Manuel Lopez VargasNo ratings yet
- Manuskrip Jurnal Terapi Nutrisi English VersionDocument22 pagesManuskrip Jurnal Terapi Nutrisi English VersionKhumaira SantaNo ratings yet
- Patophysiology Oral Q 1Document134 pagesPatophysiology Oral Q 1TijanaNo ratings yet
- Treatment of Liver CirrhosisDocument85 pagesTreatment of Liver CirrhosisPetru Boaghi100% (1)
- Practice Questions Fluids and ElectrolytesDocument55 pagesPractice Questions Fluids and ElectrolytesKathleen Ellize BetchaydaNo ratings yet
- Chapter 39: Fluid, Electrolytes, and Acid-Base Balance Yoost & Crawford: Fundamentals of Nursing: Active Learning For Collaborative Practice, 2nd EditionDocument12 pagesChapter 39: Fluid, Electrolytes, and Acid-Base Balance Yoost & Crawford: Fundamentals of Nursing: Active Learning For Collaborative Practice, 2nd Editionbafraley7No ratings yet
- Fluid and Electrolytes - Balance and DisturbancesDocument129 pagesFluid and Electrolytes - Balance and DisturbancesEmmy SaNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults - Treatment - UpToDateDocument36 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adults - Treatment - UpToDateHiKa SaGoNo ratings yet
- Sodium Imbalances (Hyponatremia Vs Hypernatremia)Document17 pagesSodium Imbalances (Hyponatremia Vs Hypernatremia)Angel FiloteoNo ratings yet
- Pyloric Stenosis in AdultsDocument6 pagesPyloric Stenosis in AdultsAlna Shelah IbañezNo ratings yet
- Unit 05 (A) Cardiac Glycosides, Educational PlatformDocument41 pagesUnit 05 (A) Cardiac Glycosides, Educational PlatformSajid AhmadNo ratings yet
- Acid BaseDocument29 pagesAcid BaseOlivia LowellNo ratings yet
- Electrolyte Mnemonic QuizletDocument3 pagesElectrolyte Mnemonic QuizletA.h.Murad100% (2)
- Toronto Notes Nephrology 2015 16Document1 pageToronto Notes Nephrology 2015 16JUSASBNo ratings yet
- Fluid and Electrolytes, Balance and DisturbancesDocument245 pagesFluid and Electrolytes, Balance and DisturbancesEdward Vladimir MoncayNo ratings yet
- Fluid Calculation For Iv InfusionDocument8 pagesFluid Calculation For Iv InfusionAsma SaleemNo ratings yet