Download as pdf or txt
You might also like
- Advanced Muscle Integration TechniqueDocument4 pagesAdvanced Muscle Integration Techniquepatsim0% (1)
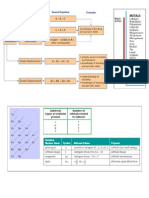
- Chemistry Cheat SheetDocument10 pagesChemistry Cheat Sheetbrook93% (40)
- Raising Power Practices OccultDocument5 pagesRaising Power Practices OccultRaúl Antonio Morales DomínguezNo ratings yet
- Clinical Prescription Management Problems: Laura Kravitz and Aamer SafdarDocument32 pagesClinical Prescription Management Problems: Laura Kravitz and Aamer SafdarAnand RajNo ratings yet
- LWUA PrimerDocument5 pagesLWUA Primeralbinoski20053388No ratings yet
- Maternity Blue Final ThesisDocument70 pagesMaternity Blue Final ThesismanuNo ratings yet
- Signs and Symptoms ofDocument8 pagesSigns and Symptoms ofNegin HekmatjooNo ratings yet
- Cervico Thoracic Rehab ProgramDocument20 pagesCervico Thoracic Rehab ProgramulaNo ratings yet
- A Different Chiropractic ApproachDocument2 pagesA Different Chiropractic ApproachEd RibeiroNo ratings yet
- Lecture Notes: Trigger Points - Massage TherapyDocument24 pagesLecture Notes: Trigger Points - Massage TherapyTaina Avramescu100% (2)
- Treating Trigger Points Reduces Pain From Knee OsteoarthritisDocument8 pagesTreating Trigger Points Reduces Pain From Knee OsteoarthritisAdi SuryawanNo ratings yet
- Sue Falsone Bridging The Gap Chapter One Excerpt1 PDFDocument14 pagesSue Falsone Bridging The Gap Chapter One Excerpt1 PDFAléssio Novais100% (2)
- Self Myofascial ReleaseDocument22 pagesSelf Myofascial ReleaseMuhammad Fahmy100% (1)
- DR Bachrach Explains Prolo, ThoroughlyDocument14 pagesDR Bachrach Explains Prolo, Thoroughlycindy.laverty5406No ratings yet
- Weebly Questions Week TwoDocument3 pagesWeebly Questions Week Twoapi-459697337No ratings yet
- Trigger Point BookDocument84 pagesTrigger Point BookRui Pedro MoreiraNo ratings yet
- SpasticityDocument13 pagesSpasticityVeny AjrinaNo ratings yet
- Soft Tissue Manipulation May Be Utilized ToDocument9 pagesSoft Tissue Manipulation May Be Utilized TopervinkumarNo ratings yet
- Fisiopatologia Do Ponto GatilhoDocument3 pagesFisiopatologia Do Ponto GatilhoAndréLuisVargasNo ratings yet
- Muscle Cramps Description Causes and TreatmentDocument2 pagesMuscle Cramps Description Causes and TreatmentVenkataNo ratings yet
- Stephens Painful AwarenessDocument4 pagesStephens Painful Awarenessmax00haNo ratings yet
- Muscle Cramps: Go ToDocument10 pagesMuscle Cramps: Go ToDewi AmeliyahNo ratings yet
- What Are Muscle CrampsDocument2 pagesWhat Are Muscle CrampsVenkataNo ratings yet
- Capstone SheetlebDocument58 pagesCapstone Sheetlebapi-675745408No ratings yet
- HandsOn Muscle TherapyDocument38 pagesHandsOn Muscle TherapyPhoenixRising61100% (2)
- MSK Shoulder Workbook Final DraftDocument36 pagesMSK Shoulder Workbook Final DraftTrailers MCNo ratings yet
- Chronic Low Back PainDocument2 pagesChronic Low Back PainRoswita RiswanNo ratings yet
- Trunk and Spine Stretching GuideDocument23 pagesTrunk and Spine Stretching GuideThiên ÂnNo ratings yet
- Working With Whiplash, Part I (Myofascial Techniques)Document5 pagesWorking With Whiplash, Part I (Myofascial Techniques)Advanced-Trainings.com100% (4)
- A Case To PointDocument5 pagesA Case To PointCJ PorrasNo ratings yet
- North American Spine Society Public Education SeriesDocument12 pagesNorth American Spine Society Public Education Serieseryoktadiputra565No ratings yet
- Chiropractic PDFDocument20 pagesChiropractic PDFAlexandru Cristian StanciuNo ratings yet
- Muscleoveractivityinthe Uppermotorneuron Syndrome: Conceptualizing A Treatment Plan and Establishing Meaningful GoalsDocument18 pagesMuscleoveractivityinthe Uppermotorneuron Syndrome: Conceptualizing A Treatment Plan and Establishing Meaningful GoalsNacho MicheloniNo ratings yet
- Pain After Stroke: Spasticity and ContracturesDocument8 pagesPain After Stroke: Spasticity and ContracturesRhoneil DejarmeNo ratings yet
- Pain After Stroke: Spasticity and ContracturesDocument8 pagesPain After Stroke: Spasticity and ContracturesAnonymous RsvDbUVZHNo ratings yet
- Injuries Main BookDocument9 pagesInjuries Main Bookomar alaa kaiokenNo ratings yet
- The Brunnstrom Stages of Stroke RecoveryDocument6 pagesThe Brunnstrom Stages of Stroke RecoveryMukrimatunnisa AkbarNo ratings yet
- Foot Reflexology 1st LevelDocument10 pagesFoot Reflexology 1st LevelOnofrei Oana ElenaNo ratings yet
- Myofascial Pain Syndrome ALICEDocument14 pagesMyofascial Pain Syndrome ALICEAlice dakshNo ratings yet
- Elbow Forearm and Hand - Stretching For Pain Relief and RehabilitationDocument17 pagesElbow Forearm and Hand - Stretching For Pain Relief and RehabilitationCarmen Llerenas100% (2)
- Stretching For Pain Relief: Professional and Home UseDocument25 pagesStretching For Pain Relief: Professional and Home UseMuhammad Arifin100% (1)
- Physio Lab 1-3Document6 pagesPhysio Lab 1-3Allison Eunice Servando100% (1)
- Back Pain Relief PDFDocument3 pagesBack Pain Relief PDFStephen MooreNo ratings yet
- Cure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainFrom EverandCure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainNo ratings yet
- Fibromyalgia SyndromeDocument10 pagesFibromyalgia Syndromebujor2000ajaNo ratings yet
- CH 13Document7 pagesCH 13Emmanuel GaliciaNo ratings yet
- Stress ManagementDocument52 pagesStress ManagementKhushboo VadgamaNo ratings yet
- 10, Pain Management of Spinalcord Injury-1Document23 pages10, Pain Management of Spinalcord Injury-1Zeeshan AhmadNo ratings yet
- Chapter 8 - Clinical Examination of The ElbowDocument3 pagesChapter 8 - Clinical Examination of The ElbowkenthepaNo ratings yet
- Reflexology Manual PDFDocument13 pagesReflexology Manual PDFPraneshNo ratings yet
- Reflexology ManualDocument13 pagesReflexology ManualPranesh100% (1)
- Frozen Shoulder - Adhesive CapsulitisDocument8 pagesFrozen Shoulder - Adhesive CapsulitisfriskaNo ratings yet
- Turn Pain Off: How to Alleviate Musculo-skeletal Pain Using Trigger Point Relief TechniqueFrom EverandTurn Pain Off: How to Alleviate Musculo-skeletal Pain Using Trigger Point Relief TechniqueNo ratings yet
- Accidents Trauma or InjuryDocument43 pagesAccidents Trauma or InjurySoleil MaxwellNo ratings yet
- Healing LawsDocument11 pagesHealing LawsJoyce YoungNo ratings yet
- 15 - Mahima Bhatia - MyalgiaDocument14 pages15 - Mahima Bhatia - MyalgiaApoorvNo ratings yet
- Materi Joint ManipulationDocument3 pagesMateri Joint ManipulationAnDi Anggara PeramanaNo ratings yet
- Basic of Manual TherapyDocument30 pagesBasic of Manual Therapycamy bhagatNo ratings yet
- MFPSDocument18 pagesMFPSएम जी एम अलाइड हेल्थ साइंसेज इंस्टिट्यूट MAHSI MGMMC IndoreNo ratings yet
- Level 2 Anatomy and Physiology: Unit 2 - Muscles of The Body Lesson 2.7 - Muscle AttachmentsDocument6 pagesLevel 2 Anatomy and Physiology: Unit 2 - Muscles of The Body Lesson 2.7 - Muscle AttachmentsGeorge OstNo ratings yet
- Backache PDFDocument173 pagesBackache PDFteammrau100% (8)
- Understanding The Kinetic Chain - A Personal Trainers Guide To Movement Dysfunction Part 1 by Dax MoyDocument4 pagesUnderstanding The Kinetic Chain - A Personal Trainers Guide To Movement Dysfunction Part 1 by Dax Moymisty1ramirez0No ratings yet
- HuloDocument3 pagesHulodreampedlar_45876997No ratings yet
- Specific GravityDocument5 pagesSpecific GravityVenkiteshNo ratings yet
- BlackBook INDEXDocument12 pagesBlackBook INDEXDanishPawaskarNo ratings yet
- Documentary Regarding Sta. Rita Town and ParishDocument6 pagesDocumentary Regarding Sta. Rita Town and ParishApril Narciso-AbenillaNo ratings yet
- Question Papers 2Document9 pagesQuestion Papers 2Anonymous hYMWbA100% (1)
- Case of Kocherov and Sergeyeva v. RussiaDocument38 pagesCase of Kocherov and Sergeyeva v. RussiaAna-Maria GeorgescuNo ratings yet
- Final Exam Cookery Nc2Document3 pagesFinal Exam Cookery Nc2rhodefrancestuazon100% (1)
- Questionnaire For HappinessDocument4 pagesQuestionnaire For HappinessSantosh GyawaliNo ratings yet
- Poison Dart Frogs: by Guy BellerantiDocument7 pagesPoison Dart Frogs: by Guy BellerantiAlle LunagNo ratings yet
- A330 FactsDocument2 pagesA330 FactsGermanTobonNo ratings yet
- TDS Ultramid 8350 HS PDFDocument2 pagesTDS Ultramid 8350 HS PDFMoni ParadaNo ratings yet
- En 13565-1 (2019) (E)Document8 pagesEn 13565-1 (2019) (E)Mircea Ovidiu BecheruNo ratings yet
- Murder MemoDocument3 pagesMurder MemoRishika AgarwalNo ratings yet
- Laboratory Manual in BiochemistryDocument37 pagesLaboratory Manual in BiochemistrySOPHIA MARGARETTE NOVELONo ratings yet
- Psyc 101 Assignment 1Document22 pagesPsyc 101 Assignment 1lola988No ratings yet
- Edb - 7580022 - GBR - en Isolating Switching Amplifier 2-Channel IMX12-DI01-2S-2T-0 24VDC CC TurckDocument3 pagesEdb - 7580022 - GBR - en Isolating Switching Amplifier 2-Channel IMX12-DI01-2S-2T-0 24VDC CC Turckzeropoint_romeoNo ratings yet
- Graduation BookDocument207 pagesGraduation Bookashwin SureshNo ratings yet
- List of Sanitary and Plumbing ItemsDocument4 pagesList of Sanitary and Plumbing ItemssumalathaNo ratings yet
- Fact-And-Opinion-Worksheet 1Document2 pagesFact-And-Opinion-Worksheet 1Eisya Miranda100% (1)
- Enabling Health and Healthcare Through IctDocument416 pagesEnabling Health and Healthcare Through Ictarif candrautamaNo ratings yet
- Us 4981687Document14 pagesUs 4981687TRISHA MAYE AREOLANo ratings yet
- Dispelling Myths Surrounding ISO Final HenryDocument25 pagesDispelling Myths Surrounding ISO Final HenrySankaranarayananNo ratings yet
- Chem 17 Exercises - Coordination Chemistry & Electrochemistry Thermochromic ComplexDocument3 pagesChem 17 Exercises - Coordination Chemistry & Electrochemistry Thermochromic ComplexLizNo ratings yet
- Eating Disorders Reading AssignmentDocument2 pagesEating Disorders Reading AssignmentNasratullah sahebzadaNo ratings yet
- The Spirit Controlled Life Ebook PDF 1Document184 pagesThe Spirit Controlled Life Ebook PDF 1Okesola AbayomiNo ratings yet
- Chapter 10tifDocument41 pagesChapter 10tifManP130% (1)