Download as docx, pdf, or txt
You might also like
- A Critical Review of Manufacturing Processes Used in Regenerated Cellulosic Fibers Viscose Cellulose Acetate Cuprammonium EtcDocument28 pagesA Critical Review of Manufacturing Processes Used in Regenerated Cellulosic Fibers Viscose Cellulose Acetate Cuprammonium EtcMoqeet AwanNo ratings yet
- Eccentric FootingDocument8 pagesEccentric Footinghemantkle2uNo ratings yet
- WarfarinDocument23 pagesWarfarinminaNo ratings yet
- Article - Roerich and The Chintamani Stone PDFDocument5 pagesArticle - Roerich and The Chintamani Stone PDFrosyua100% (1)
- EV BleedingDocument45 pagesEV BleedingJay KumarNo ratings yet
- GI Bleeding in Patients Receiving Antiplatelets and Anticoagulant TherapyDocument11 pagesGI Bleeding in Patients Receiving Antiplatelets and Anticoagulant TherapyTony LeeNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage - Treatment and Prognosis - UpToDateDocument49 pagesAneurysmal Subarachnoid Hemorrhage - Treatment and Prognosis - UpToDateSerque777No ratings yet
- Management of Antithrombotic Therapy After Bleeding in Patients With Coronary Artery Disease And/or Atrial FibrillationDocument20 pagesManagement of Antithrombotic Therapy After Bleeding in Patients With Coronary Artery Disease And/or Atrial Fibrillationdeni2razmoskiNo ratings yet
- Acetylsalicyclic Acid 08july2022Document6 pagesAcetylsalicyclic Acid 08july2022Cuong LeNo ratings yet
- Art:10.1186/s13054 016 1413 3 PDFDocument6 pagesArt:10.1186/s13054 016 1413 3 PDFFelipe GuerraNo ratings yet
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- 1 s2.0 S2667100X22000469 MainDocument10 pages1 s2.0 S2667100X22000469 MainAlfonso Ga MaNo ratings yet
- Fondaparinux in Acute Coronary Syndromes CA5068 Admin OnlyDocument9 pagesFondaparinux in Acute Coronary Syndromes CA5068 Admin OnlynaeamzNo ratings yet
- STD 2Document45 pagesSTD 2Alejandra CastroNo ratings yet
- Treatment Approach Considerations: Pericardial SclerosisDocument7 pagesTreatment Approach Considerations: Pericardial SclerosisDikie MustofadijayaNo ratings yet
- Combining Antiplatelet and Anticoagulant Therapy in Cardiovascular Disease - 2020 - AHADocument7 pagesCombining Antiplatelet and Anticoagulant Therapy in Cardiovascular Disease - 2020 - AHADrHellenNo ratings yet
- DVT TreatmentDocument24 pagesDVT TreatmentphoechoexNo ratings yet
- Acute Coronary Syndrome Oral Anticoagulation in Medically Treated Patients - UpToDateDocument14 pagesAcute Coronary Syndrome Oral Anticoagulation in Medically Treated Patients - UpToDateBrian VianaNo ratings yet
- Treatment of NSTE-ACSDocument4 pagesTreatment of NSTE-ACSAnuradha NanayakkaraNo ratings yet
- StreptokinaseDocument4 pagesStreptokinaseAfiqah So Jasmi100% (1)
- Management Acute Variceal BleedingDocument7 pagesManagement Acute Variceal BleedingSilminaNo ratings yet
- Farmakologi Kel 3Document33 pagesFarmakologi Kel 3SalsabilaRiyadiniNo ratings yet
- UntitledDocument26 pagesUntitledGian CarloNo ratings yet
- Unanswered Questions During The Live EventDocument9 pagesUnanswered Questions During The Live Eventyash_acharya007No ratings yet
- Journal Reading Circulatory Shock-1Document33 pagesJournal Reading Circulatory Shock-1bimanda aldoNo ratings yet
- Sepsis Guidelines PocketDocument2 pagesSepsis Guidelines Pocket陳悅生No ratings yet
- AFP 2014 12 Clinical RahmanDocument6 pagesAFP 2014 12 Clinical RahmanmyscribeNo ratings yet
- Desmopressin - StatPearls - NCBI BookshelfDocument2 pagesDesmopressin - StatPearls - NCBI BookshelfkikiagrivitaNo ratings yet
- Updates From The New American College of Chest Physicians: Antithrombotic Therapy and Prevention of Thrombosis, 9 EditionDocument22 pagesUpdates From The New American College of Chest Physicians: Antithrombotic Therapy and Prevention of Thrombosis, 9 Editionbuddho81No ratings yet
- Articulo - FarmacologíaDocument13 pagesArticulo - FarmacologíaJhon RVNo ratings yet
- 1 s2.0 S097368832100236XDocument8 pages1 s2.0 S097368832100236XHưng Nguyễn KiềuNo ratings yet
- Br. J. Anaesth. 2007 Chassot 316 28Document13 pagesBr. J. Anaesth. 2007 Chassot 316 28Rhahima SyafrilNo ratings yet
- Clinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeDocument4 pagesClinical Liver Disease - 2012 - Reverter - Management of An Acute Variceal Bleeding EpisodeEUODIA HANA KRISTINANo ratings yet
- Stroke Clinical PathwayDocument35 pagesStroke Clinical PathwayLaurencia Leny100% (2)
- Ehad 123Document12 pagesEhad 123Daiane GonçalvesNo ratings yet
- Antiplatelet and Antithrombotic Therapy (Triple Therapy) Risk and Benefits (Am J Med 2014)Document7 pagesAntiplatelet and Antithrombotic Therapy (Triple Therapy) Risk and Benefits (Am J Med 2014)Eduardo MenaNo ratings yet
- Intensive - Care - Medicine. VasopressorDocument4 pagesIntensive - Care - Medicine. VasopressorSa7arNo ratings yet
- Impact of Intravenous Aspirin Administration On Ventriculostomy-Associated Hemorrhage in Coiled Acute Subarachnoid Hemorrhage PatientsDocument9 pagesImpact of Intravenous Aspirin Administration On Ventriculostomy-Associated Hemorrhage in Coiled Acute Subarachnoid Hemorrhage PatientsRichard FNo ratings yet
- Antiplatelet Drugs, Anticoagulants and Elective SurgeryDocument5 pagesAntiplatelet Drugs, Anticoagulants and Elective SurgeryJanice WongNo ratings yet
- 2196Document28 pages2196andi rahmatNo ratings yet
- AnticoagulantsDocument3 pagesAnticoagulantsKarthik SubramaniamNo ratings yet
- Control of Spinal Anesthesia-Induced Hypotension in Adults - PMCDocument14 pagesControl of Spinal Anesthesia-Induced Hypotension in Adults - PMCAkash SharmaNo ratings yet
- Vasoconstriction in Septic Shock: What'S New in Intensive CareDocument4 pagesVasoconstriction in Septic Shock: What'S New in Intensive CareGabriela PachecoNo ratings yet
- Haematology DrugsDocument17 pagesHaematology DrugsParyNo ratings yet
- Bahan Bleeding 1Document6 pagesBahan Bleeding 1jalaludinsyahNo ratings yet
- 1000 - Johnson Venous ThrombDocument33 pages1000 - Johnson Venous ThrombAlejandro Kanito Alvarez SNo ratings yet
- QH GDL 951Document15 pagesQH GDL 951Candra YogiswaraNo ratings yet
- Portal HTNDocument34 pagesPortal HTNfeeo8266No ratings yet
- First PeriodDocument11 pagesFirst PeriodHapsari Kartika DewiNo ratings yet
- Hepatic CirrhosisDocument1 pageHepatic CirrhosisHoomi BeautyNo ratings yet
- Restart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalDocument11 pagesRestart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalPhaimNo ratings yet
- DVT PE ManagementDocument6 pagesDVT PE Managementகோகுல் தங்கவேல்No ratings yet
- Significant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd ToDocument8 pagesSignificant Early In-Hospital Benefit Was Seen. Clopidogrel Is Prefferd TogilnifNo ratings yet
- Ten Tips To Optimize VasopressorsDocument4 pagesTen Tips To Optimize VasopressorsSimon HiouNo ratings yet
- Rivaroxaban or Aspirin For Extended Treatment of Venous Thromboembolism EINSTEIN CHOICE 2017 NEJMDocument12 pagesRivaroxaban or Aspirin For Extended Treatment of Venous Thromboembolism EINSTEIN CHOICE 2017 NEJMGustavo MartinezNo ratings yet
- Ventilatory SupportDocument21 pagesVentilatory SupportAllahbesertkitaNo ratings yet
- Official Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument43 pagesOfficial Reprint From Uptodate ©2018 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedVictor M' PimentelNo ratings yet
- Current Cardiovascular Therapy Pharmacological-229-246Document18 pagesCurrent Cardiovascular Therapy Pharmacological-229-246Yulian 53No ratings yet
- Warfarin Dan AspirinDocument10 pagesWarfarin Dan Aspirindita novia maharaniNo ratings yet
- Venous Thromboembolism: Anticoagulation After Initial ManagementDocument30 pagesVenous Thromboembolism: Anticoagulation After Initial ManagementKhor Chin PooNo ratings yet
- Preoperative Care of Patients With Kidney DiseaseDocument13 pagesPreoperative Care of Patients With Kidney Disease84ghmynprvNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Nikon E200 ManualDocument88 pagesNikon E200 ManualrosyuaNo ratings yet
- postMBBSallotmentROUNDone PDFDocument163 pagespostMBBSallotmentROUNDone PDFrosyuaNo ratings yet
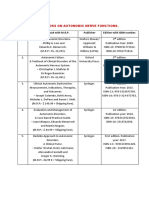
- LIST OF BOOKS ON AUTONOMIC NERVE FUNCTIONS With ISBN.-1Document1 pageLIST OF BOOKS ON AUTONOMIC NERVE FUNCTIONS With ISBN.-1rosyuaNo ratings yet
- JJJJJJJJJJJJJ KKKKKKKKKKKKKKKK LLLL YyyyyyyyyyDocument1 pageJJJJJJJJJJJJJ KKKKKKKKKKKKKKKK LLLL YyyyyyyyyyrosyuaNo ratings yet
- 15 Minute WorkoutDocument1 page15 Minute WorkoutrosyuaNo ratings yet
- Electrolux Oven Cum Steam Oven DetailDocument4 pagesElectrolux Oven Cum Steam Oven DetailrosyuaNo ratings yet
- HC Plant Based FoodsDocument3 pagesHC Plant Based Foodsrosyua100% (1)
- Brain 101 Info (Merged) PDFDocument186 pagesBrain 101 Info (Merged) PDFrosyuaNo ratings yet
- Creativity: Thinking Outside The Box: Creative QuestionsDocument2 pagesCreativity: Thinking Outside The Box: Creative QuestionsrosyuaNo ratings yet
- Surgical KnotDocument99 pagesSurgical KnotmherbergNo ratings yet
- Test SetupDocument11 pagesTest SetupKarthik PariharNo ratings yet
- CG Report ADocument8 pagesCG Report AsachinNo ratings yet
- Soleic - Volt Solar Energy - Solar Installation AgreementDocument5 pagesSoleic - Volt Solar Energy - Solar Installation AgreementCamilo EspinosaNo ratings yet
- Petronas Technical Standards: Separator Modelling TechniquesDocument26 pagesPetronas Technical Standards: Separator Modelling Techniquesahmadreza777No ratings yet
- Foriegn Investment in Real Estate - IndiaDocument6 pagesForiegn Investment in Real Estate - IndiasirishdsNo ratings yet
- Administration and ManagementDocument28 pagesAdministration and ManagementMonikaNo ratings yet
- SOP SAP Landed Cost 0.1Document9 pagesSOP SAP Landed Cost 0.1supendra phuyalNo ratings yet
- Foundations of MathematicsDocument352 pagesFoundations of MathematicsPatrick MorgadoNo ratings yet
- Traffic Management and Accident Investigation With DrivingDocument18 pagesTraffic Management and Accident Investigation With DrivingPatrick LeysonNo ratings yet
- ICAEW - Bus - Fin - Chapter 5 - StudentDocument123 pagesICAEW - Bus - Fin - Chapter 5 - StudentMai HuyenNo ratings yet
- 5 - Pile FoundationsDocument15 pages5 - Pile FoundationspeterNo ratings yet
- Expression EncoderDocument34 pagesExpression EncoderIvan TašinNo ratings yet
- Damping Modification for Spectrum: Lap-Loi Chung (鍾立來)Document39 pagesDamping Modification for Spectrum: Lap-Loi Chung (鍾立來)陳俊鴻No ratings yet
- Neonatal JaundiceDocument15 pagesNeonatal JaundiceSharan SekhonNo ratings yet
- Injector Chain Length MeasurementDocument6 pagesInjector Chain Length MeasurementRami DalNo ratings yet
- Vapor Compression RefrigerationDocument8 pagesVapor Compression RefrigerationSepehr SaNo ratings yet
- Safety Perforation Gun IncidentDocument5 pagesSafety Perforation Gun IncidentB Deyse FernandesNo ratings yet
- Ablative Cooling Materials and SystemsDocument84 pagesAblative Cooling Materials and SystemsAerojet Rocketdyne RS-25No ratings yet
- ACADEMIC WRITING SKILLS - Part 2Document5 pagesACADEMIC WRITING SKILLS - Part 2MWENDA MOSESNo ratings yet
- JEE Advanced Full Test Xvi Paper 1Document23 pagesJEE Advanced Full Test Xvi Paper 1DurgeshJhaNo ratings yet
- Section: Expenditure Subsystem Subsection: 060-01 Subsection: Overview Page 1 of 2Document2 pagesSection: Expenditure Subsystem Subsection: 060-01 Subsection: Overview Page 1 of 2Clea Marie MissionNo ratings yet
- Tai Wai Maintenance Center: Planning, Design, and ConstructionDocument7 pagesTai Wai Maintenance Center: Planning, Design, and ConstructionSomesh SiddharthNo ratings yet
- Eco 270Document9 pagesEco 270Tarun Shankar ChoudharyNo ratings yet
- Earth Science: Safety Precautions Before, During, and After Volcanic EruptionDocument33 pagesEarth Science: Safety Precautions Before, During, and After Volcanic Eruptionrhalf tagaduarNo ratings yet
- Dynamic Positioning Revalidation: Online Application GuideDocument23 pagesDynamic Positioning Revalidation: Online Application GuideCandisftNo ratings yet
- New Microsoft Office Word DocumentDocument9 pagesNew Microsoft Office Word DocumentSanthiya SanjeeviNo ratings yet
- Slice Account Statement - May '22Document5 pagesSlice Account Statement - May '22Anil kumar kamathNo ratings yet
- Ree AnneDocument1 pageRee AnneRee Anne DiolesteNo ratings yet