
Cardiology Fellowship Education in The Era of High-Density Training, Data Tracking, and Quality Measures
Cardiology Fellowship Education in The Era of High-Density Training, Data Tracking, and Quality Measures
You might also like
- Study The Effect of Acids and Bases On The Tensile Strength of A FibreDocument15 pagesStudy The Effect of Acids and Bases On The Tensile Strength of A FibreHiaderKhokhawala75% (69)
- Sample Midterm 2 F303Document12 pagesSample Midterm 2 F303philmoreNo ratings yet
- Cardiovascular Perfusion ThesisDocument4 pagesCardiovascular Perfusion Thesisamandagraytulsa100% (2)
- S561 FullDocument14 pagesS561 FullrizkydimasaputraNo ratings yet
- Medicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterDocument13 pagesMedicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterDiana C Muñoz VidalNo ratings yet
- Capstone Final PaperDocument27 pagesCapstone Final Paperapi-533585896No ratings yet
- Ims Mini Case2Document2 pagesIms Mini Case2Ms KaniaNo ratings yet
- Guideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureDocument30 pagesGuideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureNindy Yantika MciNo ratings yet
- Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureDocument30 pagesPhysical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureSyahriadin SyamNo ratings yet
- Literature Review Cardiac RehabilitationDocument5 pagesLiterature Review Cardiac Rehabilitationafmzitaaoxahvp100% (1)
- High-Intensity Interval Training in Patients With Intermittent ClaudicationDocument13 pagesHigh-Intensity Interval Training in Patients With Intermittent ClaudicationAntónio José OliveiraNo ratings yet
- The Promise Perils Problems and Progress of Competency Based Medical EducationDocument8 pagesThe Promise Perils Problems and Progress of Competency Based Medical EducationJasmik SinghNo ratings yet
- Korean Guidelines For Interventional Recanalization of Lower Extremity ArteriesDocument27 pagesKorean Guidelines For Interventional Recanalization of Lower Extremity ArteriesIsaias García PalafoxNo ratings yet
- Enhancing UK Core Medical Training Through Simulation-Based Education: An Evidence-Based ApproachDocument36 pagesEnhancing UK Core Medical Training Through Simulation-Based Education: An Evidence-Based ApproachAndxp51No ratings yet
- Cathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicDocument9 pagesCathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicvaleriaNo ratings yet
- Medical Surgical Nursing ThesisDocument6 pagesMedical Surgical Nursing Thesisjanchampagnefargo100% (2)
- 07 NadderDocument6 pages07 NaddervioletirisesNo ratings yet
- Literature Review Cardiopulmonary ResuscitationDocument6 pagesLiterature Review Cardiopulmonary Resuscitationaflskkcez100% (1)
- 03 Do We Need Other GuidelinesDocument7 pages03 Do We Need Other GuidelinesGold4allNo ratings yet
- Development of Models For Regional Cardiac SurgeryDocument9 pagesDevelopment of Models For Regional Cardiac SurgeryJoji BorromeoNo ratings yet
- Ebj M3 Rle24Document6 pagesEbj M3 Rle24Ayen PaloNo ratings yet
- Advanced Life Support Training and Assessment PDFDocument6 pagesAdvanced Life Support Training and Assessment PDFwilmaNo ratings yet
- Postoperative Care: Who Should Look After Patients Following Surgery?Document5 pagesPostoperative Care: Who Should Look After Patients Following Surgery?kishanm77No ratings yet
- The Evolution and Future of ACC/AHA Clinical Practice Guidelines: A 30-Year JourneyDocument12 pagesThe Evolution and Future of ACC/AHA Clinical Practice Guidelines: A 30-Year JourneyYouyouNo ratings yet
- Stroke Nursing DissertationDocument4 pagesStroke Nursing DissertationBestCollegePaperWritingServiceCanada100% (1)
- Article Print 209Document9 pagesArticle Print 209Brenda Shaffitry OriNo ratings yet
- MD StudentDocument3 pagesMD StudentgailNo ratings yet
- Cardiac Rehabilitation Adherence: A Multifaceted ApproachDocument13 pagesCardiac Rehabilitation Adherence: A Multifaceted ApproachBOHR International Journal of Research on Cardiology and Cardiovascular DiseasesNo ratings yet
- Evolution of Outcomes in Cardiothoracic SurgeryDocument8 pagesEvolution of Outcomes in Cardiothoracic Surgeryannisa statiraNo ratings yet
- Final Curriculum Guidelines Interventional CardiologyDocument47 pagesFinal Curriculum Guidelines Interventional Cardiologychase parksNo ratings yet
- New Way To ListenDocument2 pagesNew Way To ListenVITRIA NOVITA SARINo ratings yet
- ESC Heart Failure - 2022 - Zhang - Efficacy and Safety of Digital Therapeutics Based Cardiac Rehabilitation in Heart FailureDocument10 pagesESC Heart Failure - 2022 - Zhang - Efficacy and Safety of Digital Therapeutics Based Cardiac Rehabilitation in Heart FailurehimadootNo ratings yet
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocument3 pagesTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioNo ratings yet
- Perit Dial Int 2011 Blake 218 39Document22 pagesPerit Dial Int 2011 Blake 218 39Ika AgustinNo ratings yet
- Musculoskeletal Radiology Curriculum ForDocument27 pagesMusculoskeletal Radiology Curriculum ForHardik AgrawalNo ratings yet
- Artigo 10 Reabili.Document15 pagesArtigo 10 Reabili.Gabriela GhissardiNo ratings yet
- Care Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WereDocument10 pagesCare Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WerenanikNo ratings yet
- Building A Clinical Cardiothoracic Surgical Program: A Multi-Institutional ModelDocument4 pagesBuilding A Clinical Cardiothoracic Surgical Program: A Multi-Institutional Modelnouha jhiderNo ratings yet
- Vandermolen CurrProbCadiol2022Document14 pagesVandermolen CurrProbCadiol2022doubaoheroNo ratings yet
- CPAxDocument9 pagesCPAxCarla CrivellaroNo ratings yet
- Basic Life SupportDocument15 pagesBasic Life Supportmiss betawiNo ratings yet
- Cardiac Point-of-Care Ultrasound: State of The Art in Medical School EducationDocument12 pagesCardiac Point-of-Care Ultrasound: State of The Art in Medical School Educationmariano villavicencioNo ratings yet
- CR QolDocument14 pagesCR Qollita PhDNo ratings yet
- National Clin Ed Guidelines 2011Document23 pagesNational Clin Ed Guidelines 2011Meet singhNo ratings yet
- A Cost-Consequence Analysis ofDocument10 pagesA Cost-Consequence Analysis ofviviana benavidesNo ratings yet
- Comments, Opinions, and Reviews: Recommendations For Advancing Development of Acute Stroke TherapiesDocument9 pagesComments, Opinions, and Reviews: Recommendations For Advancing Development of Acute Stroke TherapiesDaniela Paredes QuirozNo ratings yet
- Student Objectives - ACOGDocument164 pagesStudent Objectives - ACOGmango91286100% (1)
- Article 3Document11 pagesArticle 3Anonymous zXwP003No ratings yet
- IFOMPT Cervical Framework Final September 2020Document41 pagesIFOMPT Cervical Framework Final September 2020Maximiliano LabraNo ratings yet
- Clinical Services Roadmap Operational Plan For Clinical Work TeamDocument14 pagesClinical Services Roadmap Operational Plan For Clinical Work TeamAhmed M. RafatNo ratings yet
- Priorities For Physiotherapy Research in The UK: Topics Prioritised by The Cardiorespiratory Expert PanelDocument35 pagesPriorities For Physiotherapy Research in The UK: Topics Prioritised by The Cardiorespiratory Expert PaneljoshuagnanasekarNo ratings yet
- Oup Accepted Manuscript 2019Document26 pagesOup Accepted Manuscript 2019akusayang1029No ratings yet
- Competency Based Medical Education (CBME) : An Overview and Relevance To The Education of Future Surgical OncologistsDocument11 pagesCompetency Based Medical Education (CBME) : An Overview and Relevance To The Education of Future Surgical Oncologistsdeepak sharmaNo ratings yet
- Understanding Prehabilitation: General Anaesthesia Tutorial394Document5 pagesUnderstanding Prehabilitation: General Anaesthesia Tutorial394Abhishek LonikarNo ratings yet
- Case Study Weight Loss ClinicDocument11 pagesCase Study Weight Loss ClinicsambitdwivediNo ratings yet
- Separating Science From EconomicsDocument3 pagesSeparating Science From Economicsbenny christantoNo ratings yet
- Mcnichols 2012Document1 pageMcnichols 2012hugogrupononnaNo ratings yet
- ASE Reintro Statement FINALDocument14 pagesASE Reintro Statement FINALIrina Cabac-PogoreviciNo ratings yet
- Coronary Care Unit To Cardiac Intensive Care Unit: Acute Medical Cardiac Caredadapting With The TimesDocument3 pagesCoronary Care Unit To Cardiac Intensive Care Unit: Acute Medical Cardiac Caredadapting With The TimesBahtiar AfandiNo ratings yet
- Clinical Application DissertationDocument4 pagesClinical Application DissertationDoMyPaperForMoneyUK100% (1)
- Acutecarenurse Practitionersin Oncologiccritical Care:Thememorial Sloan-Kettering Cancercenter ExperienceDocument11 pagesAcutecarenurse Practitionersin Oncologiccritical Care:Thememorial Sloan-Kettering Cancercenter Experienceemanuel sibonike mwambonaNo ratings yet
- Emergent Vascular Access: A Guide for Healthcare ProfessionalsFrom EverandEmergent Vascular Access: A Guide for Healthcare ProfessionalsJames H. PaxtonNo ratings yet
- Essentials of PsychologyDocument519 pagesEssentials of PsychologyhodovskyNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
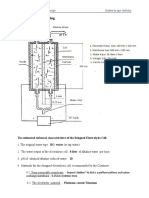
- Elecrolysis Cell DrawingDocument2 pagesElecrolysis Cell DrawingRimaNo ratings yet
- Swc5-Ld: Specified PerformanceDocument1 pageSwc5-Ld: Specified PerformanceBenjamin MillerNo ratings yet
- Specifications Is 950-1980Document13 pagesSpecifications Is 950-1980anuavi93No ratings yet
- Week 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Document3 pagesWeek 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Rebecca Miller HorneNo ratings yet
- Anti-Drunk and Drugged Driving Act of 2013Document19 pagesAnti-Drunk and Drugged Driving Act of 2013Atoy Liby OjeñarNo ratings yet
- Thickening Time and Compressive Strength Correlations For Bentonitic-Class "G" Cement SlurriesDocument9 pagesThickening Time and Compressive Strength Correlations For Bentonitic-Class "G" Cement Slurriesصفاء رجبNo ratings yet
- Manejo de Suelos Salinos y SodicoDocument189 pagesManejo de Suelos Salinos y SodicoJean Marco Gozme AcostaNo ratings yet
- Surgical OrthodonticsDocument4 pagesSurgical OrthodonticsFernaz Behlim100% (2)
- Bir Form 1600Document9 pagesBir Form 1600Vincent De GuzmanNo ratings yet
- A Rasch Analysis On Collapsing Categories in Item - S Response Scales of Survey Questionnaire Maybe It - S Not One Size Fits All PDFDocument29 pagesA Rasch Analysis On Collapsing Categories in Item - S Response Scales of Survey Questionnaire Maybe It - S Not One Size Fits All PDFNancy NgNo ratings yet
- CL312: Computer Aided Process Equipment DesignDocument11 pagesCL312: Computer Aided Process Equipment DesignWilliam AdamsNo ratings yet
- NeidanDocument3 pagesNeidanRiccardo LautiziNo ratings yet
- Is QualityDocument14 pagesIs QualityArathy VikramNo ratings yet
- 24 Management of Facial FracturesDocument32 pages24 Management of Facial FracturesxienaistNo ratings yet
- Guantanamo BayDocument6 pagesGuantanamo Bayleddy101No ratings yet
- Entrepreneurship Business Plan: Group Ha Rufon 12 HUMSS - A DisiplinaDocument6 pagesEntrepreneurship Business Plan: Group Ha Rufon 12 HUMSS - A DisiplinaNathalie UbaNo ratings yet
- Week 7 - Rheumatoid ArthritisDocument1 pageWeek 7 - Rheumatoid ArthritisTuTitNo ratings yet
- Technical Datasheet of SBRDocument13 pagesTechnical Datasheet of SBRKSPCB KalaburagiNo ratings yet
- Overview of The Changing Family Pattern in Rural BangladeshDocument9 pagesOverview of The Changing Family Pattern in Rural BangladeshSadia Noor0% (1)
- Art 1Document6 pagesArt 1Cristina VladutaNo ratings yet
- CDS57006 Bosch LSU 4.9 Sensor PDFDocument4 pagesCDS57006 Bosch LSU 4.9 Sensor PDFAnonymous K3FaYFlNo ratings yet
- Fire Engine SpecsDocument432 pagesFire Engine SpecsDarin WateNo ratings yet
- 2.TECHNICAL PROPOSAL For Scope Study of Compensation For Survivors of Sexual and GBVDocument32 pages2.TECHNICAL PROPOSAL For Scope Study of Compensation For Survivors of Sexual and GBVTaufiq Us Samad TonmoyNo ratings yet
- MTC-100 Treasury FormDocument1 pageMTC-100 Treasury FormvijiNo ratings yet
- Whether Ordinance On Self-Denial of Nuclear Power Harmful To IndiaDocument55 pagesWhether Ordinance On Self-Denial of Nuclear Power Harmful To IndiabksubbaraoNo ratings yet
- Learning Challenges of Student Nurses in Virtual Learning QuestionnairesDocument8 pagesLearning Challenges of Student Nurses in Virtual Learning QuestionnairesJelaveil De VeraNo ratings yet
























































































Download as pdf or txt
You might also like
- Study The Effect of Acids and Bases On The Tensile Strength of A FibreDocument15 pagesStudy The Effect of Acids and Bases On The Tensile Strength of A FibreHiaderKhokhawala75% (69)
- Sample Midterm 2 F303Document12 pagesSample Midterm 2 F303philmoreNo ratings yet
- Cardiovascular Perfusion ThesisDocument4 pagesCardiovascular Perfusion Thesisamandagraytulsa100% (2)
- S561 FullDocument14 pagesS561 FullrizkydimasaputraNo ratings yet
- Medicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterDocument13 pagesMedicalschooltrainingfor Thesurgeon: Christopher P. Scally,, Rebecca M. MinterDiana C Muñoz VidalNo ratings yet
- Capstone Final PaperDocument27 pagesCapstone Final Paperapi-533585896No ratings yet
- Ims Mini Case2Document2 pagesIms Mini Case2Ms KaniaNo ratings yet
- Guideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureDocument30 pagesGuideline: Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureNindy Yantika MciNo ratings yet
- Physical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureDocument30 pagesPhysical Therapist Clinical Practice Guideline For The Management of Individuals With Heart FailureSyahriadin SyamNo ratings yet
- Literature Review Cardiac RehabilitationDocument5 pagesLiterature Review Cardiac Rehabilitationafmzitaaoxahvp100% (1)
- High-Intensity Interval Training in Patients With Intermittent ClaudicationDocument13 pagesHigh-Intensity Interval Training in Patients With Intermittent ClaudicationAntónio José OliveiraNo ratings yet
- The Promise Perils Problems and Progress of Competency Based Medical EducationDocument8 pagesThe Promise Perils Problems and Progress of Competency Based Medical EducationJasmik SinghNo ratings yet
- Korean Guidelines For Interventional Recanalization of Lower Extremity ArteriesDocument27 pagesKorean Guidelines For Interventional Recanalization of Lower Extremity ArteriesIsaias García PalafoxNo ratings yet
- Enhancing UK Core Medical Training Through Simulation-Based Education: An Evidence-Based ApproachDocument36 pagesEnhancing UK Core Medical Training Through Simulation-Based Education: An Evidence-Based ApproachAndxp51No ratings yet
- Cathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicDocument9 pagesCathet Cardio Intervent - 2019 - Baran - SCAI Clinical Expert Consensus Statement On The Classification of CardiogenicvaleriaNo ratings yet
- Medical Surgical Nursing ThesisDocument6 pagesMedical Surgical Nursing Thesisjanchampagnefargo100% (2)
- 07 NadderDocument6 pages07 NaddervioletirisesNo ratings yet
- Literature Review Cardiopulmonary ResuscitationDocument6 pagesLiterature Review Cardiopulmonary Resuscitationaflskkcez100% (1)
- 03 Do We Need Other GuidelinesDocument7 pages03 Do We Need Other GuidelinesGold4allNo ratings yet
- Development of Models For Regional Cardiac SurgeryDocument9 pagesDevelopment of Models For Regional Cardiac SurgeryJoji BorromeoNo ratings yet
- Ebj M3 Rle24Document6 pagesEbj M3 Rle24Ayen PaloNo ratings yet
- Advanced Life Support Training and Assessment PDFDocument6 pagesAdvanced Life Support Training and Assessment PDFwilmaNo ratings yet
- Postoperative Care: Who Should Look After Patients Following Surgery?Document5 pagesPostoperative Care: Who Should Look After Patients Following Surgery?kishanm77No ratings yet
- The Evolution and Future of ACC/AHA Clinical Practice Guidelines: A 30-Year JourneyDocument12 pagesThe Evolution and Future of ACC/AHA Clinical Practice Guidelines: A 30-Year JourneyYouyouNo ratings yet
- Stroke Nursing DissertationDocument4 pagesStroke Nursing DissertationBestCollegePaperWritingServiceCanada100% (1)
- Article Print 209Document9 pagesArticle Print 209Brenda Shaffitry OriNo ratings yet
- MD StudentDocument3 pagesMD StudentgailNo ratings yet
- Cardiac Rehabilitation Adherence: A Multifaceted ApproachDocument13 pagesCardiac Rehabilitation Adherence: A Multifaceted ApproachBOHR International Journal of Research on Cardiology and Cardiovascular DiseasesNo ratings yet
- Evolution of Outcomes in Cardiothoracic SurgeryDocument8 pagesEvolution of Outcomes in Cardiothoracic Surgeryannisa statiraNo ratings yet
- Final Curriculum Guidelines Interventional CardiologyDocument47 pagesFinal Curriculum Guidelines Interventional Cardiologychase parksNo ratings yet
- New Way To ListenDocument2 pagesNew Way To ListenVITRIA NOVITA SARINo ratings yet
- ESC Heart Failure - 2022 - Zhang - Efficacy and Safety of Digital Therapeutics Based Cardiac Rehabilitation in Heart FailureDocument10 pagesESC Heart Failure - 2022 - Zhang - Efficacy and Safety of Digital Therapeutics Based Cardiac Rehabilitation in Heart FailurehimadootNo ratings yet
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocument3 pagesTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioNo ratings yet
- Perit Dial Int 2011 Blake 218 39Document22 pagesPerit Dial Int 2011 Blake 218 39Ika AgustinNo ratings yet
- Musculoskeletal Radiology Curriculum ForDocument27 pagesMusculoskeletal Radiology Curriculum ForHardik AgrawalNo ratings yet
- Artigo 10 Reabili.Document15 pagesArtigo 10 Reabili.Gabriela GhissardiNo ratings yet
- Care Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WereDocument10 pagesCare Nurse As Well As The Institute For Healthcare Improvement (IHI) Website WerenanikNo ratings yet
- Building A Clinical Cardiothoracic Surgical Program: A Multi-Institutional ModelDocument4 pagesBuilding A Clinical Cardiothoracic Surgical Program: A Multi-Institutional Modelnouha jhiderNo ratings yet
- Vandermolen CurrProbCadiol2022Document14 pagesVandermolen CurrProbCadiol2022doubaoheroNo ratings yet
- CPAxDocument9 pagesCPAxCarla CrivellaroNo ratings yet
- Basic Life SupportDocument15 pagesBasic Life Supportmiss betawiNo ratings yet
- Cardiac Point-of-Care Ultrasound: State of The Art in Medical School EducationDocument12 pagesCardiac Point-of-Care Ultrasound: State of The Art in Medical School Educationmariano villavicencioNo ratings yet
- CR QolDocument14 pagesCR Qollita PhDNo ratings yet
- National Clin Ed Guidelines 2011Document23 pagesNational Clin Ed Guidelines 2011Meet singhNo ratings yet
- A Cost-Consequence Analysis ofDocument10 pagesA Cost-Consequence Analysis ofviviana benavidesNo ratings yet
- Comments, Opinions, and Reviews: Recommendations For Advancing Development of Acute Stroke TherapiesDocument9 pagesComments, Opinions, and Reviews: Recommendations For Advancing Development of Acute Stroke TherapiesDaniela Paredes QuirozNo ratings yet
- Student Objectives - ACOGDocument164 pagesStudent Objectives - ACOGmango91286100% (1)
- Article 3Document11 pagesArticle 3Anonymous zXwP003No ratings yet
- IFOMPT Cervical Framework Final September 2020Document41 pagesIFOMPT Cervical Framework Final September 2020Maximiliano LabraNo ratings yet
- Clinical Services Roadmap Operational Plan For Clinical Work TeamDocument14 pagesClinical Services Roadmap Operational Plan For Clinical Work TeamAhmed M. RafatNo ratings yet
- Priorities For Physiotherapy Research in The UK: Topics Prioritised by The Cardiorespiratory Expert PanelDocument35 pagesPriorities For Physiotherapy Research in The UK: Topics Prioritised by The Cardiorespiratory Expert PaneljoshuagnanasekarNo ratings yet
- Oup Accepted Manuscript 2019Document26 pagesOup Accepted Manuscript 2019akusayang1029No ratings yet
- Competency Based Medical Education (CBME) : An Overview and Relevance To The Education of Future Surgical OncologistsDocument11 pagesCompetency Based Medical Education (CBME) : An Overview and Relevance To The Education of Future Surgical Oncologistsdeepak sharmaNo ratings yet
- Understanding Prehabilitation: General Anaesthesia Tutorial394Document5 pagesUnderstanding Prehabilitation: General Anaesthesia Tutorial394Abhishek LonikarNo ratings yet
- Case Study Weight Loss ClinicDocument11 pagesCase Study Weight Loss ClinicsambitdwivediNo ratings yet
- Separating Science From EconomicsDocument3 pagesSeparating Science From Economicsbenny christantoNo ratings yet
- Mcnichols 2012Document1 pageMcnichols 2012hugogrupononnaNo ratings yet
- ASE Reintro Statement FINALDocument14 pagesASE Reintro Statement FINALIrina Cabac-PogoreviciNo ratings yet
- Coronary Care Unit To Cardiac Intensive Care Unit: Acute Medical Cardiac Caredadapting With The TimesDocument3 pagesCoronary Care Unit To Cardiac Intensive Care Unit: Acute Medical Cardiac Caredadapting With The TimesBahtiar AfandiNo ratings yet
- Clinical Application DissertationDocument4 pagesClinical Application DissertationDoMyPaperForMoneyUK100% (1)
- Acutecarenurse Practitionersin Oncologiccritical Care:Thememorial Sloan-Kettering Cancercenter ExperienceDocument11 pagesAcutecarenurse Practitionersin Oncologiccritical Care:Thememorial Sloan-Kettering Cancercenter Experienceemanuel sibonike mwambonaNo ratings yet
- Emergent Vascular Access: A Guide for Healthcare ProfessionalsFrom EverandEmergent Vascular Access: A Guide for Healthcare ProfessionalsJames H. PaxtonNo ratings yet
- Essentials of PsychologyDocument519 pagesEssentials of PsychologyhodovskyNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- Elecrolysis Cell DrawingDocument2 pagesElecrolysis Cell DrawingRimaNo ratings yet
- Swc5-Ld: Specified PerformanceDocument1 pageSwc5-Ld: Specified PerformanceBenjamin MillerNo ratings yet
- Specifications Is 950-1980Document13 pagesSpecifications Is 950-1980anuavi93No ratings yet
- Week 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Document3 pagesWeek 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Rebecca Miller HorneNo ratings yet
- Anti-Drunk and Drugged Driving Act of 2013Document19 pagesAnti-Drunk and Drugged Driving Act of 2013Atoy Liby OjeñarNo ratings yet
- Thickening Time and Compressive Strength Correlations For Bentonitic-Class "G" Cement SlurriesDocument9 pagesThickening Time and Compressive Strength Correlations For Bentonitic-Class "G" Cement Slurriesصفاء رجبNo ratings yet
- Manejo de Suelos Salinos y SodicoDocument189 pagesManejo de Suelos Salinos y SodicoJean Marco Gozme AcostaNo ratings yet
- Surgical OrthodonticsDocument4 pagesSurgical OrthodonticsFernaz Behlim100% (2)
- Bir Form 1600Document9 pagesBir Form 1600Vincent De GuzmanNo ratings yet
- A Rasch Analysis On Collapsing Categories in Item - S Response Scales of Survey Questionnaire Maybe It - S Not One Size Fits All PDFDocument29 pagesA Rasch Analysis On Collapsing Categories in Item - S Response Scales of Survey Questionnaire Maybe It - S Not One Size Fits All PDFNancy NgNo ratings yet
- CL312: Computer Aided Process Equipment DesignDocument11 pagesCL312: Computer Aided Process Equipment DesignWilliam AdamsNo ratings yet
- NeidanDocument3 pagesNeidanRiccardo LautiziNo ratings yet
- Is QualityDocument14 pagesIs QualityArathy VikramNo ratings yet
- 24 Management of Facial FracturesDocument32 pages24 Management of Facial FracturesxienaistNo ratings yet
- Guantanamo BayDocument6 pagesGuantanamo Bayleddy101No ratings yet
- Entrepreneurship Business Plan: Group Ha Rufon 12 HUMSS - A DisiplinaDocument6 pagesEntrepreneurship Business Plan: Group Ha Rufon 12 HUMSS - A DisiplinaNathalie UbaNo ratings yet
- Week 7 - Rheumatoid ArthritisDocument1 pageWeek 7 - Rheumatoid ArthritisTuTitNo ratings yet
- Technical Datasheet of SBRDocument13 pagesTechnical Datasheet of SBRKSPCB KalaburagiNo ratings yet
- Overview of The Changing Family Pattern in Rural BangladeshDocument9 pagesOverview of The Changing Family Pattern in Rural BangladeshSadia Noor0% (1)
- Art 1Document6 pagesArt 1Cristina VladutaNo ratings yet
- CDS57006 Bosch LSU 4.9 Sensor PDFDocument4 pagesCDS57006 Bosch LSU 4.9 Sensor PDFAnonymous K3FaYFlNo ratings yet
- Fire Engine SpecsDocument432 pagesFire Engine SpecsDarin WateNo ratings yet
- 2.TECHNICAL PROPOSAL For Scope Study of Compensation For Survivors of Sexual and GBVDocument32 pages2.TECHNICAL PROPOSAL For Scope Study of Compensation For Survivors of Sexual and GBVTaufiq Us Samad TonmoyNo ratings yet
- MTC-100 Treasury FormDocument1 pageMTC-100 Treasury FormvijiNo ratings yet
- Whether Ordinance On Self-Denial of Nuclear Power Harmful To IndiaDocument55 pagesWhether Ordinance On Self-Denial of Nuclear Power Harmful To IndiabksubbaraoNo ratings yet
- Learning Challenges of Student Nurses in Virtual Learning QuestionnairesDocument8 pagesLearning Challenges of Student Nurses in Virtual Learning QuestionnairesJelaveil De VeraNo ratings yet