Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- IntelliVue Information Center HL7 Programmer S Guide PDFDocument210 pagesIntelliVue Information Center HL7 Programmer S Guide PDFhugutuxNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cervical CADocument32 pagesCervical CAEvangel Padua100% (2)
- Ic ManualDocument416 pagesIc ManualEvangel PaduaNo ratings yet
- CrutchesDocument9 pagesCrutchesEvangel PaduaNo ratings yet
- C 10Document344 pagesC 10Anonymous yxFeWtNo ratings yet
- SupppDocument1 pageSupppEvangel PaduaNo ratings yet
- Pathophysiology: Predi Sposi NG Facto Rs Age (5 Mont HS)Document7 pagesPathophysiology: Predi Sposi NG Facto Rs Age (5 Mont HS)Evangel PaduaNo ratings yet
- Evangel Padua Psychopathology PrintDocument1 pageEvangel Padua Psychopathology PrintEvangel PaduaNo ratings yet
- August 19, 2014: Mr. Nicomedes O. Palafox, JR., Man, RNDocument1 pageAugust 19, 2014: Mr. Nicomedes O. Palafox, JR., Man, RNEvangel PaduaNo ratings yet
- Russel&Shang Psychopathology PrintDocument1 pageRussel&Shang Psychopathology PrintEvangel PaduaNo ratings yet
- Nikki PsychophatologyDocument1 pageNikki PsychophatologyEvangel PaduaNo ratings yet
- Pathophysiology: Steptococcus PneumoniaeDocument2 pagesPathophysiology: Steptococcus PneumoniaeEvangel PaduaNo ratings yet
- RED. PhysicalDocument5 pagesRED. PhysicalEvangel PaduaNo ratings yet
- 3 Factors RellitDocument1 page3 Factors RellitEvangel PaduaNo ratings yet
- Republic of The Philippines Araullo University - Pen Brgy. Bitas, Cabanatuan City College of NursingDocument8 pagesRepublic of The Philippines Araullo University - Pen Brgy. Bitas, Cabanatuan City College of NursingEvangel PaduaNo ratings yet
- CASESTUDY Pott's DiseaseDocument27 pagesCASESTUDY Pott's Diseasemae_kel100% (45)
- Positive and Negative Face: Stephen Levinson Politeness FaceDocument1 pagePositive and Negative Face: Stephen Levinson Politeness FaceEvangel PaduaNo ratings yet
- Raullo Niversity: Teaching PlanDocument1 pageRaullo Niversity: Teaching PlanEvangel PaduaNo ratings yet
- Herniated Disk (Princess)Document4 pagesHerniated Disk (Princess)Evangel PaduaNo ratings yet
- Abegail A. Rimando 3BSN-1 Pott's DiseaseDocument2 pagesAbegail A. Rimando 3BSN-1 Pott's DiseaseEvangel PaduaNo ratings yet
- I Love You Like A Love Song Baby!Document1 pageI Love You Like A Love Song Baby!Evangel PaduaNo ratings yet
- TCS iON Digital Learning Hub: Learn, Share, CollaborateDocument24 pagesTCS iON Digital Learning Hub: Learn, Share, CollaborateganeshsunnyNo ratings yet
- National War Memorial - Urban DesignDocument15 pagesNational War Memorial - Urban DesignRoopendraKumarNo ratings yet
- Byzantine ArmyDocument7 pagesByzantine ArmyDimitris Mavridis100% (1)
- Policy - Task 2 ContentDocument6 pagesPolicy - Task 2 ContentJadhav AmitNo ratings yet
- Hizon, Czarina May CVDocument3 pagesHizon, Czarina May CVnotapernota101No ratings yet
- General Characteristics of Fungi. Details AbcdefDocument9 pagesGeneral Characteristics of Fungi. Details Abcdefabdul hadiNo ratings yet
- Sample Assignment 1-1Document20 pagesSample Assignment 1-1Nir IslamNo ratings yet
- Media Richness TheoryDocument10 pagesMedia Richness Theoryestefania sofea zahara100% (2)
- Weather ChangesDocument34 pagesWeather ChangesEmina PodicNo ratings yet
- Japanese Suite: Gustav HolstDocument55 pagesJapanese Suite: Gustav HolstLaTonya Hutchison 101No ratings yet
- Assembly of PartsDocument29 pagesAssembly of PartsthirumalaikumaranNo ratings yet
- The Seven Types of Yellow Sapphire and Their Stability To Light PDFDocument10 pagesThe Seven Types of Yellow Sapphire and Their Stability To Light PDFdebjeet royNo ratings yet
- SM-Personal Finance-Unit1to3Document176 pagesSM-Personal Finance-Unit1to3Priyanshu BhattNo ratings yet
- Evaluation of Antimicrobial and Antioxidant Activity of Crude Methanol Extract and Its Fractions of Mussaenda Philippica LeavesDocument14 pagesEvaluation of Antimicrobial and Antioxidant Activity of Crude Methanol Extract and Its Fractions of Mussaenda Philippica Leavesiaset123No ratings yet
- Main Hydraulic System M315CDocument8 pagesMain Hydraulic System M315CMEULEYENo ratings yet
- Oodp Project 1Document14 pagesOodp Project 1dikshaNo ratings yet
- Textile Internship - Usha YarnsDocument49 pagesTextile Internship - Usha YarnsROHAN GIREESHNo ratings yet
- Oxygen Scavenger Boiler Water TreatmentDocument6 pagesOxygen Scavenger Boiler Water TreatmentDarius DsouzaNo ratings yet
- Cambridge University Thesis SearchDocument5 pagesCambridge University Thesis Searchfc2fqg8j100% (2)
- HB 2016 - 2nd - Edition - 13 - 01 - 17Document293 pagesHB 2016 - 2nd - Edition - 13 - 01 - 17Vaidya NurNo ratings yet
- BIO Genetics Eukaryote TranscriptionDocument23 pagesBIO Genetics Eukaryote TranscriptionAnonymous SVy8sOsvJDNo ratings yet
- Makeshift Arsenal by LoweryDocument37 pagesMakeshift Arsenal by LoweryD50% (2)
- CVPDocument20 pagesCVPThomas K. AddaiNo ratings yet
- Preterm Prelabor Rupture of Membranes - Clinical Manifestations and Diagnosis - UpToDateDocument26 pagesPreterm Prelabor Rupture of Membranes - Clinical Manifestations and Diagnosis - UpToDateCristinaCaprosNo ratings yet
- 1672298032245-ICE CE-29 - RevisionDocument86 pages1672298032245-ICE CE-29 - RevisionSoumyaranjan NayakNo ratings yet
- Cyber SOCDocument9 pagesCyber SOCTrần Trung HiếuNo ratings yet
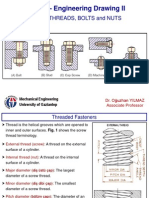
- SCREW THREADS, BOLTS and NUTS PDFDocument10 pagesSCREW THREADS, BOLTS and NUTS PDFhrhgk50% (2)
- Fruit Juice IndustryDocument11 pagesFruit Juice IndustryArlene GutierrezNo ratings yet