
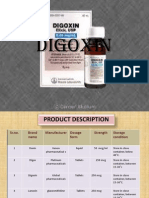
Drug Description: Reductions in Risk of CHD Mortality and Cardiovascular Events
Drug Description: Reductions in Risk of CHD Mortality and Cardiovascular Events
You might also like
- Maram File 2 - CalculationsDocument36 pagesMaram File 2 - CalculationsWhabbbNo ratings yet
- 50 Suspects 86 ChargesDocument3 pages50 Suspects 86 ChargesNewsWCYBDigitalNo ratings yet
- Clinical Calculations - MonashDocument5 pagesClinical Calculations - MonashSabrine ElkhodrNo ratings yet
- Pharmacy Project1Document52 pagesPharmacy Project1Tamiru Bekele100% (1)
- VASCORDocument2 pagesVASCORmoasrisNo ratings yet
- GLUCOPHAGE-metformin Hydrochloride Tablet, Film Coated GLUCOPHAGE XR - Metformin Hydrochloride Tablet, Extended Releas e Bris Tol-Myers Squibb CompanyDocument25 pagesGLUCOPHAGE-metformin Hydrochloride Tablet, Film Coated GLUCOPHAGE XR - Metformin Hydrochloride Tablet, Extended Releas e Bris Tol-Myers Squibb CompanyNadiaIsnainiNo ratings yet
- Valsartan + HydrochlorotiazideDocument17 pagesValsartan + Hydrochlorotiazideddandan_2No ratings yet
- Highlights of Prescribing InformationDocument0 pagesHighlights of Prescribing InformationFahmi HidayatNo ratings yet
- Digitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008Document18 pagesDigitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008LenyNo ratings yet
- Losartan Potassium 50mg Tablets - Summary of Product Characteristics (SMPC)Document16 pagesLosartan Potassium 50mg Tablets - Summary of Product Characteristics (SMPC)Pharmacist ipsNo ratings yet
- Drug Study On DigoxinDocument8 pagesDrug Study On DigoxinDonald BidenNo ratings yet
- Piroxicam Pharmacology 1Document16 pagesPiroxicam Pharmacology 1Shafira TamaraNo ratings yet
- Indications: Details With Side EffectsDocument5 pagesIndications: Details With Side EffectsJillian HernandezNo ratings yet
- Linezolid 600mg Film Coated Tablets SMPCDocument16 pagesLinezolid 600mg Film Coated Tablets SMPCAndi SuhriyanaNo ratings yet
- Summary of Product CharacteristicsDocument9 pagesSummary of Product Characteristicsddandan_2No ratings yet
- Dipyrone (Metamizole) : Pronunciation Brand Names: InternationalDocument9 pagesDipyrone (Metamizole) : Pronunciation Brand Names: InternationalRismaya AminiNo ratings yet
- Exjade: (Deferasirox)Document13 pagesExjade: (Deferasirox)athayafebNo ratings yet
- Pharma ProjectDocument9 pagesPharma Projectfarah.abd97No ratings yet
- Cataflam: (Diclofenac Potassium)Document10 pagesCataflam: (Diclofenac Potassium)ddandan_2No ratings yet
- DrugDocument13 pagesDrugkhesler BacallaNo ratings yet
- Etoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)Document1 pageEtoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)vikasjha12345No ratings yet
- Jardiance Epar Product Information - enDocument47 pagesJardiance Epar Product Information - enSaad MasoodNo ratings yet
- Interns ACEIsDocument62 pagesInterns ACEIsmohamedsharkawwy82No ratings yet
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- Name of The Medicinal Product: AdultsDocument9 pagesName of The Medicinal Product: Adultsddandan_2No ratings yet
- Prescribing Information: 1. Name of The Medicinal ProductDocument5 pagesPrescribing Information: 1. Name of The Medicinal Productddandan_20% (1)
- Hemofarm Vademekum Engleska Verzija Za 2013Document143 pagesHemofarm Vademekum Engleska Verzija Za 2013Svet MedicineNo ratings yet
- VoltarenTablet May2019.SINv1 App110821Document13 pagesVoltarenTablet May2019.SINv1 App110821zahragubil95No ratings yet
- Summary of Product CharacteristicsDocument7 pagesSummary of Product Characteristicsanon_458167643No ratings yet
- Meds DiabetesDocument5 pagesMeds DiabetesAnjangsari 'aRie' WijayantiNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument39 pagesSee Full Prescribing Information For Complete Boxed WarningsadafNo ratings yet
- SPC - Ma807 04004Document20 pagesSPC - Ma807 04004farlaqaqcNo ratings yet
- 8 Drug StudyDocument19 pages8 Drug StudyLoyloy D ManNo ratings yet
- Diazoxide 50mg DatasheetDocument6 pagesDiazoxide 50mg DatasheetarifpharmjuNo ratings yet
- Older AdultsDocument13 pagesOlder AdultsSri Sri WahNo ratings yet
- CKD CmeDocument45 pagesCKD Cmeizatul farhanahNo ratings yet
- FenofibrateDocument7 pagesFenofibrateVikas Karande100% (1)
- Voltfast-Sep 2022.SIN-app260123 PDFDocument14 pagesVoltfast-Sep 2022.SIN-app260123 PDFChelang AbdulkareemNo ratings yet
- DM Emtyaz 3Document55 pagesDM Emtyaz 3Muhammed MuhsinNo ratings yet
- Chronic Kidney Disease: A Case Presentation OnDocument16 pagesChronic Kidney Disease: A Case Presentation OnSafoora RafeeqNo ratings yet
- Banocide and Banocide ForteDocument10 pagesBanocide and Banocide ForteJosephNo ratings yet
- Mefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysiaDocument1 pageMefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysianuruladyanisaifuzzamanNo ratings yet
- Hydroxyzine Orifarm Film-Coated Tablet ENG SMPC - 09001bee807a397dDocument11 pagesHydroxyzine Orifarm Film-Coated Tablet ENG SMPC - 09001bee807a397dmaroxgamingNo ratings yet
- AtorvastatinDocument23 pagesAtorvastatinanon_434656209No ratings yet
- Anti Hyper Lip I de MicsDocument7 pagesAnti Hyper Lip I de MicsAravinthNo ratings yet
- USPI - Med Guide - Feldene - Piroxicam - CapsulesDocument15 pagesUSPI - Med Guide - Feldene - Piroxicam - CapsulesDini FarhatunnabilahNo ratings yet
- Diclofenacsandoztab AdjustmentDocument14 pagesDiclofenacsandoztab AdjustmentShafira TamaraNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- Diuretics: Generic Name: FUROSEMIDEDocument12 pagesDiuretics: Generic Name: FUROSEMIDEJR BetonioNo ratings yet
- Famasi IIDocument6 pagesFamasi IIMerlyn AngelicaNo ratings yet
- ZyprexatabZyprexazydiswafer PDFDocument22 pagesZyprexatabZyprexazydiswafer PDFJan BularioNo ratings yet
- The Management of Gout: Much Has Changed: BackgroundDocument5 pagesThe Management of Gout: Much Has Changed: Backgroundtika_876267153No ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument13 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsNDung NDungNo ratings yet
- 2016 Article 420Document23 pages2016 Article 420Astri Arri FebriantiNo ratings yet
- Atacor SPCDocument9 pagesAtacor SPCRannia1No ratings yet
- Hyprlipdemia 2020 4th EditionDocument24 pagesHyprlipdemia 2020 4th EditionLillian KrazemNo ratings yet
- Zyprexatab ZyprexazydiswaferDocument22 pagesZyprexatab ZyprexazydiswaferAmin AhmedNo ratings yet
- Cyclosporin Final (1) - 1-EditDocument32 pagesCyclosporin Final (1) - 1-Editsky.blueNo ratings yet
- Levofloxacin-1Document31 pagesLevofloxacin-1Fallen AngelNo ratings yet
- CARVEDILOL Nursing ImplicationsDocument2 pagesCARVEDILOL Nursing Implicationsshiraz.aNo ratings yet
- A Dala Toro StabDocument17 pagesA Dala Toro StabNovriman LiviaNo ratings yet
- LercanidipineDocument8 pagesLercanidipineddandan_2No ratings yet
- RosuvastatinDocument17 pagesRosuvastatinddandan_2No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Deflaming Supplements PDFDocument4 pagesDeflaming Supplements PDFDavidSeamanNo ratings yet
- Name of Pharmacy: ................................. CityDocument1 pageName of Pharmacy: ................................. Cityravi sheladiyaNo ratings yet
- Archana CVDocument2 pagesArchana CVRavi KantNo ratings yet
- Brief About GMPDocument2 pagesBrief About GMPAnand KulkarniNo ratings yet
- Antibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesDocument13 pagesAntibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesNishant ShresthaNo ratings yet
- FYP Proposal DraftDocument17 pagesFYP Proposal DraftKristen TeeNo ratings yet
- Abbott LaboratoriesDocument6 pagesAbbott LaboratoriesdineshkoriNo ratings yet
- Drug MenuDocument17 pagesDrug MenukathlynmangasiNo ratings yet
- 8th Sem SyllabusDocument32 pages8th Sem SyllabusDRx Ijajul HussainNo ratings yet
- Drug CalculationsDocument78 pagesDrug CalculationsNader Smadi100% (9)
- Max Dura PDFDocument3 pagesMax Dura PDFMillenium AyurvedaNo ratings yet
- H5773e PDFDocument83 pagesH5773e PDFPatrick PerezNo ratings yet
- Pharmaceutical Formulation: Principles and Dosage FormsDocument3 pagesPharmaceutical Formulation: Principles and Dosage FormsPharmacistBDNo ratings yet
- Registered Product List: Vega Pharmaceuticals (PVT.) LTDDocument12 pagesRegistered Product List: Vega Pharmaceuticals (PVT.) LTDWaheedullah AhmadiNo ratings yet
- Formulation Development and Release Studies of Indomethacin SuppositoriesDocument4 pagesFormulation Development and Release Studies of Indomethacin Suppositoriesmauran aurodNo ratings yet
- Ethiopian Plant For Covid-19 Potentailly Also PortulacaDocument40 pagesEthiopian Plant For Covid-19 Potentailly Also Portulacaharold jitschak bueno de mesquitaNo ratings yet
- Recommendations For Implementing Antimicrobial Stewardship Programs in Latin America and The Caribbean: Manual For Public Health Decision-MakersDocument144 pagesRecommendations For Implementing Antimicrobial Stewardship Programs in Latin America and The Caribbean: Manual For Public Health Decision-Makersalexandra sanchesNo ratings yet
- Compartment ModelsDocument67 pagesCompartment ModelsGhadeer M HassanNo ratings yet
- C-4 Dosage Form DesignDocument80 pagesC-4 Dosage Form DesignJhef ebuengaNo ratings yet
- India: Drug Regulatory Framework & New InitiativesDocument16 pagesIndia: Drug Regulatory Framework & New InitiativesRajesh RanganathanNo ratings yet
- The Impact of Implementation of ICH Guidelines in Non-ICH CountriesDocument35 pagesThe Impact of Implementation of ICH Guidelines in Non-ICH CountriesJonas SaldanhaNo ratings yet
- Pilot Study of The Short-Term Physico-Chemical Stability of Atenolol Tablets Stored in A Multi-Compartment Compliance AidDocument7 pagesPilot Study of The Short-Term Physico-Chemical Stability of Atenolol Tablets Stored in A Multi-Compartment Compliance AidPerli DuNo ratings yet
- Product ListDocument3 pagesProduct ListjagrutiNo ratings yet
- PHD211 - Ointment 2019Document147 pagesPHD211 - Ointment 2019honeylemon.co100% (2)
- Republic of The Philippines vs. Drugmakers G.R. No. 190837 March 5, 2014Document10 pagesRepublic of The Philippines vs. Drugmakers G.R. No. 190837 March 5, 2014herbs22225847No ratings yet
- Manual Dispensing (Lengkap)Document14 pagesManual Dispensing (Lengkap)zayNo ratings yet
























































































Download as doc, pdf, or txt
You might also like
- Maram File 2 - CalculationsDocument36 pagesMaram File 2 - CalculationsWhabbbNo ratings yet
- 50 Suspects 86 ChargesDocument3 pages50 Suspects 86 ChargesNewsWCYBDigitalNo ratings yet
- Clinical Calculations - MonashDocument5 pagesClinical Calculations - MonashSabrine ElkhodrNo ratings yet
- Pharmacy Project1Document52 pagesPharmacy Project1Tamiru Bekele100% (1)
- VASCORDocument2 pagesVASCORmoasrisNo ratings yet
- GLUCOPHAGE-metformin Hydrochloride Tablet, Film Coated GLUCOPHAGE XR - Metformin Hydrochloride Tablet, Extended Releas e Bris Tol-Myers Squibb CompanyDocument25 pagesGLUCOPHAGE-metformin Hydrochloride Tablet, Film Coated GLUCOPHAGE XR - Metformin Hydrochloride Tablet, Extended Releas e Bris Tol-Myers Squibb CompanyNadiaIsnainiNo ratings yet
- Valsartan + HydrochlorotiazideDocument17 pagesValsartan + Hydrochlorotiazideddandan_2No ratings yet
- Highlights of Prescribing InformationDocument0 pagesHighlights of Prescribing InformationFahmi HidayatNo ratings yet
- Digitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008Document18 pagesDigitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008LenyNo ratings yet
- Losartan Potassium 50mg Tablets - Summary of Product Characteristics (SMPC)Document16 pagesLosartan Potassium 50mg Tablets - Summary of Product Characteristics (SMPC)Pharmacist ipsNo ratings yet
- Drug Study On DigoxinDocument8 pagesDrug Study On DigoxinDonald BidenNo ratings yet
- Piroxicam Pharmacology 1Document16 pagesPiroxicam Pharmacology 1Shafira TamaraNo ratings yet
- Indications: Details With Side EffectsDocument5 pagesIndications: Details With Side EffectsJillian HernandezNo ratings yet
- Linezolid 600mg Film Coated Tablets SMPCDocument16 pagesLinezolid 600mg Film Coated Tablets SMPCAndi SuhriyanaNo ratings yet
- Summary of Product CharacteristicsDocument9 pagesSummary of Product Characteristicsddandan_2No ratings yet
- Dipyrone (Metamizole) : Pronunciation Brand Names: InternationalDocument9 pagesDipyrone (Metamizole) : Pronunciation Brand Names: InternationalRismaya AminiNo ratings yet
- Exjade: (Deferasirox)Document13 pagesExjade: (Deferasirox)athayafebNo ratings yet
- Pharma ProjectDocument9 pagesPharma Projectfarah.abd97No ratings yet
- Cataflam: (Diclofenac Potassium)Document10 pagesCataflam: (Diclofenac Potassium)ddandan_2No ratings yet
- DrugDocument13 pagesDrugkhesler BacallaNo ratings yet
- Etoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)Document1 pageEtoricoxib 120 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)vikasjha12345No ratings yet
- Jardiance Epar Product Information - enDocument47 pagesJardiance Epar Product Information - enSaad MasoodNo ratings yet
- Interns ACEIsDocument62 pagesInterns ACEIsmohamedsharkawwy82No ratings yet
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- Name of The Medicinal Product: AdultsDocument9 pagesName of The Medicinal Product: Adultsddandan_2No ratings yet
- Prescribing Information: 1. Name of The Medicinal ProductDocument5 pagesPrescribing Information: 1. Name of The Medicinal Productddandan_20% (1)
- Hemofarm Vademekum Engleska Verzija Za 2013Document143 pagesHemofarm Vademekum Engleska Verzija Za 2013Svet MedicineNo ratings yet
- VoltarenTablet May2019.SINv1 App110821Document13 pagesVoltarenTablet May2019.SINv1 App110821zahragubil95No ratings yet
- Summary of Product CharacteristicsDocument7 pagesSummary of Product Characteristicsanon_458167643No ratings yet
- Meds DiabetesDocument5 pagesMeds DiabetesAnjangsari 'aRie' WijayantiNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument39 pagesSee Full Prescribing Information For Complete Boxed WarningsadafNo ratings yet
- SPC - Ma807 04004Document20 pagesSPC - Ma807 04004farlaqaqcNo ratings yet
- 8 Drug StudyDocument19 pages8 Drug StudyLoyloy D ManNo ratings yet
- Diazoxide 50mg DatasheetDocument6 pagesDiazoxide 50mg DatasheetarifpharmjuNo ratings yet
- Older AdultsDocument13 pagesOlder AdultsSri Sri WahNo ratings yet
- CKD CmeDocument45 pagesCKD Cmeizatul farhanahNo ratings yet
- FenofibrateDocument7 pagesFenofibrateVikas Karande100% (1)
- Voltfast-Sep 2022.SIN-app260123 PDFDocument14 pagesVoltfast-Sep 2022.SIN-app260123 PDFChelang AbdulkareemNo ratings yet
- DM Emtyaz 3Document55 pagesDM Emtyaz 3Muhammed MuhsinNo ratings yet
- Chronic Kidney Disease: A Case Presentation OnDocument16 pagesChronic Kidney Disease: A Case Presentation OnSafoora RafeeqNo ratings yet
- Banocide and Banocide ForteDocument10 pagesBanocide and Banocide ForteJosephNo ratings yet
- Mefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysiaDocument1 pageMefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysianuruladyanisaifuzzamanNo ratings yet
- Hydroxyzine Orifarm Film-Coated Tablet ENG SMPC - 09001bee807a397dDocument11 pagesHydroxyzine Orifarm Film-Coated Tablet ENG SMPC - 09001bee807a397dmaroxgamingNo ratings yet
- AtorvastatinDocument23 pagesAtorvastatinanon_434656209No ratings yet
- Anti Hyper Lip I de MicsDocument7 pagesAnti Hyper Lip I de MicsAravinthNo ratings yet
- USPI - Med Guide - Feldene - Piroxicam - CapsulesDocument15 pagesUSPI - Med Guide - Feldene - Piroxicam - CapsulesDini FarhatunnabilahNo ratings yet
- Diclofenacsandoztab AdjustmentDocument14 pagesDiclofenacsandoztab AdjustmentShafira TamaraNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- Diuretics: Generic Name: FUROSEMIDEDocument12 pagesDiuretics: Generic Name: FUROSEMIDEJR BetonioNo ratings yet
- Famasi IIDocument6 pagesFamasi IIMerlyn AngelicaNo ratings yet
- ZyprexatabZyprexazydiswafer PDFDocument22 pagesZyprexatabZyprexazydiswafer PDFJan BularioNo ratings yet
- The Management of Gout: Much Has Changed: BackgroundDocument5 pagesThe Management of Gout: Much Has Changed: Backgroundtika_876267153No ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument13 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsNDung NDungNo ratings yet
- 2016 Article 420Document23 pages2016 Article 420Astri Arri FebriantiNo ratings yet
- Atacor SPCDocument9 pagesAtacor SPCRannia1No ratings yet
- Hyprlipdemia 2020 4th EditionDocument24 pagesHyprlipdemia 2020 4th EditionLillian KrazemNo ratings yet
- Zyprexatab ZyprexazydiswaferDocument22 pagesZyprexatab ZyprexazydiswaferAmin AhmedNo ratings yet
- Cyclosporin Final (1) - 1-EditDocument32 pagesCyclosporin Final (1) - 1-Editsky.blueNo ratings yet
- Levofloxacin-1Document31 pagesLevofloxacin-1Fallen AngelNo ratings yet
- CARVEDILOL Nursing ImplicationsDocument2 pagesCARVEDILOL Nursing Implicationsshiraz.aNo ratings yet
- A Dala Toro StabDocument17 pagesA Dala Toro StabNovriman LiviaNo ratings yet
- LercanidipineDocument8 pagesLercanidipineddandan_2No ratings yet
- RosuvastatinDocument17 pagesRosuvastatinddandan_2No ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Deflaming Supplements PDFDocument4 pagesDeflaming Supplements PDFDavidSeamanNo ratings yet
- Name of Pharmacy: ................................. CityDocument1 pageName of Pharmacy: ................................. Cityravi sheladiyaNo ratings yet
- Archana CVDocument2 pagesArchana CVRavi KantNo ratings yet
- Brief About GMPDocument2 pagesBrief About GMPAnand KulkarniNo ratings yet
- Antibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesDocument13 pagesAntibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesNishant ShresthaNo ratings yet
- FYP Proposal DraftDocument17 pagesFYP Proposal DraftKristen TeeNo ratings yet
- Abbott LaboratoriesDocument6 pagesAbbott LaboratoriesdineshkoriNo ratings yet
- Drug MenuDocument17 pagesDrug MenukathlynmangasiNo ratings yet
- 8th Sem SyllabusDocument32 pages8th Sem SyllabusDRx Ijajul HussainNo ratings yet
- Drug CalculationsDocument78 pagesDrug CalculationsNader Smadi100% (9)
- Max Dura PDFDocument3 pagesMax Dura PDFMillenium AyurvedaNo ratings yet
- H5773e PDFDocument83 pagesH5773e PDFPatrick PerezNo ratings yet
- Pharmaceutical Formulation: Principles and Dosage FormsDocument3 pagesPharmaceutical Formulation: Principles and Dosage FormsPharmacistBDNo ratings yet
- Registered Product List: Vega Pharmaceuticals (PVT.) LTDDocument12 pagesRegistered Product List: Vega Pharmaceuticals (PVT.) LTDWaheedullah AhmadiNo ratings yet
- Formulation Development and Release Studies of Indomethacin SuppositoriesDocument4 pagesFormulation Development and Release Studies of Indomethacin Suppositoriesmauran aurodNo ratings yet
- Ethiopian Plant For Covid-19 Potentailly Also PortulacaDocument40 pagesEthiopian Plant For Covid-19 Potentailly Also Portulacaharold jitschak bueno de mesquitaNo ratings yet
- Recommendations For Implementing Antimicrobial Stewardship Programs in Latin America and The Caribbean: Manual For Public Health Decision-MakersDocument144 pagesRecommendations For Implementing Antimicrobial Stewardship Programs in Latin America and The Caribbean: Manual For Public Health Decision-Makersalexandra sanchesNo ratings yet
- Compartment ModelsDocument67 pagesCompartment ModelsGhadeer M HassanNo ratings yet
- C-4 Dosage Form DesignDocument80 pagesC-4 Dosage Form DesignJhef ebuengaNo ratings yet
- India: Drug Regulatory Framework & New InitiativesDocument16 pagesIndia: Drug Regulatory Framework & New InitiativesRajesh RanganathanNo ratings yet
- The Impact of Implementation of ICH Guidelines in Non-ICH CountriesDocument35 pagesThe Impact of Implementation of ICH Guidelines in Non-ICH CountriesJonas SaldanhaNo ratings yet
- Pilot Study of The Short-Term Physico-Chemical Stability of Atenolol Tablets Stored in A Multi-Compartment Compliance AidDocument7 pagesPilot Study of The Short-Term Physico-Chemical Stability of Atenolol Tablets Stored in A Multi-Compartment Compliance AidPerli DuNo ratings yet
- Product ListDocument3 pagesProduct ListjagrutiNo ratings yet
- PHD211 - Ointment 2019Document147 pagesPHD211 - Ointment 2019honeylemon.co100% (2)
- Republic of The Philippines vs. Drugmakers G.R. No. 190837 March 5, 2014Document10 pagesRepublic of The Philippines vs. Drugmakers G.R. No. 190837 March 5, 2014herbs22225847No ratings yet
- Manual Dispensing (Lengkap)Document14 pagesManual Dispensing (Lengkap)zayNo ratings yet