
Patwari11breathing PDF
Patwari11breathing PDF
You might also like
- VMC Series Vertical Machining Centers: Operator'S ManualDocument176 pagesVMC Series Vertical Machining Centers: Operator'S Manualcafetux100% (2)
- Grammar Bank 3 1Document6 pagesGrammar Bank 3 1Anahit GalstyanNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- References ASEAN2Document3 pagesReferences ASEAN2M IrwaniNo ratings yet
- Implementation and Analysis of Respiration-Rate Estimation Using Impulse-Based UwbDocument7 pagesImplementation and Analysis of Respiration-Rate Estimation Using Impulse-Based UwbVikas MehraNo ratings yet
- Remote Monitoring of Human Vital Signs Using MM-WDocument11 pagesRemote Monitoring of Human Vital Signs Using MM-W1070038825No ratings yet
- Localization, Tracking, and Imaging of Targets in Wireless Sensor Networks: An Invited ReviewDocument4 pagesLocalization, Tracking, and Imaging of Targets in Wireless Sensor Networks: An Invited ReviewPraveen KrishnaNo ratings yet
- Design and Implementation of Monitoring System For Breathing and Heart Rate Pattern Using Wifi SignalsDocument7 pagesDesign and Implementation of Monitoring System For Breathing and Heart Rate Pattern Using Wifi Signalsroboteee71421No ratings yet
- Eddy Current Based Flexible Sensor For Contactless Measurement of BreathingDocument4 pagesEddy Current Based Flexible Sensor For Contactless Measurement of BreathingA047 prince KumarNo ratings yet
- Yang 2019Document4 pagesYang 2019Swarnadip SahaNo ratings yet
- Non invasiveRespirationRateMonitoringDocument12 pagesNon invasiveRespirationRateMonitoringWekesa RobinsonNo ratings yet
- A TOA Based Positioning Technique of Medical Implanted DevicesDocument5 pagesA TOA Based Positioning Technique of Medical Implanted DevicesHadi RadNo ratings yet
- Human Body As AntennaDocument11 pagesHuman Body As AntennaSaadat RehmanNo ratings yet
- Dalal 2017Document6 pagesDalal 2017yanivNo ratings yet
- 2009-01-Personalized Feedback Based On Automatic Activity Recognition From Mixed-Source Raw Sensor DataDocument2 pages2009-01-Personalized Feedback Based On Automatic Activity Recognition From Mixed-Source Raw Sensor DataHarm op den AkkerNo ratings yet
- MS RapidHRV Resubmission Clean V2Document28 pagesMS RapidHRV Resubmission Clean V2wmasyraf4No ratings yet
- Inner Bounds On Performance of Radar and Communications Co-ExistenceDocument11 pagesInner Bounds On Performance of Radar and Communications Co-ExistencerallabhandiSKNo ratings yet
- 2020 - On CSI-Based Vital Sign Monitoring Using Commodity WiFiDocument27 pages2020 - On CSI-Based Vital Sign Monitoring Using Commodity WiFisyed hasan alaviNo ratings yet
- LISTS ALGS Elnahrawy04limitsDocument9 pagesLISTS ALGS Elnahrawy04limitsLi XuanjiNo ratings yet
- Spectroscopy.: Applications of Auto CorrelationDocument3 pagesSpectroscopy.: Applications of Auto CorrelationAishwarya SumaNo ratings yet
- A 2.4Ghz Non-Contact Biosensor System For Continuous Monitoring of Vital-SignsDocument29 pagesA 2.4Ghz Non-Contact Biosensor System For Continuous Monitoring of Vital-SignsShankarPrasaiNo ratings yet
- Infrasound Source and Calibration Methods in Seismic InterpretationDocument7 pagesInfrasound Source and Calibration Methods in Seismic InterpretationIJAR JOURNALNo ratings yet
- Review Article: Ultrawideband Technology in Medicine: A SurveyDocument10 pagesReview Article: Ultrawideband Technology in Medicine: A SurveyNouralhuda A HasanNo ratings yet
- Lifetime of Sensor NewtworkingDocument10 pagesLifetime of Sensor NewtworkingNaqiey LuluNo ratings yet
- RESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsDocument6 pagesRESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsMariana Córdoba HolguínNo ratings yet
- Estimation of Respiratory Rate Through Breathing AudioDocument12 pagesEstimation of Respiratory Rate Through Breathing AudioIJRASETPublicationsNo ratings yet
- SleepDocument15 pagesSleepgauravchauNo ratings yet
- RASS: A Real-Time, Accurate, and Scalable System For Tracking Transceiver-Free ObjectsDocument13 pagesRASS: A Real-Time, Accurate, and Scalable System For Tracking Transceiver-Free Objectscuong371992No ratings yet
- Deriving Heart Rate and Respiratory Rate From Pulse Oximetry DataDocument7 pagesDeriving Heart Rate and Respiratory Rate From Pulse Oximetry DataVelumani sNo ratings yet
- 10 1109@tbme 2012 2206591 PDFDocument7 pages10 1109@tbme 2012 2206591 PDFToàn LêNo ratings yet
- 00tmc00-Santagati-2561277.pdf - 7463487-AamDocument1 page00tmc00-Santagati-2561277.pdf - 7463487-AamGeneration GenerationNo ratings yet
- IEEE Paper On Wireless Sensing of Human Respiratory ParametersDocument11 pagesIEEE Paper On Wireless Sensing of Human Respiratory ParametersPrasanth YgNo ratings yet
- Final Complete VersionDocument17 pagesFinal Complete Versionviệt hưng trầnNo ratings yet
- 2023 CNN For The Real Time Monitoring of Vital S Based On IR UWB During SleepDocument15 pages2023 CNN For The Real Time Monitoring of Vital S Based On IR UWB During Sleepshireyoung717No ratings yet
- Ad Hoc Networks: Tal Marian, Osnat (Ossi) Mokryn, Yuval ShavittDocument11 pagesAd Hoc Networks: Tal Marian, Osnat (Ossi) Mokryn, Yuval ShavittJayraj SinghNo ratings yet
- Cognitive StressDocument6 pagesCognitive StressPallav DuttaNo ratings yet
- A Review On Different Technical Specifications of Respiratory Rate Monitors PDFDocument6 pagesA Review On Different Technical Specifications of Respiratory Rate Monitors PDFesatjournalsNo ratings yet
- Evaluating and Comparing Algorithms For Respiratory Motion PredictionDocument24 pagesEvaluating and Comparing Algorithms For Respiratory Motion PredictionPhil NovosadNo ratings yet
- A Wearable System For Tremor Monitoring and AnalysisDocument9 pagesA Wearable System For Tremor Monitoring and AnalysisZoran ConstantinescuNo ratings yet
- Event Sensing Dy Span 08Document12 pagesEvent Sensing Dy Span 08VigneshInfotechNo ratings yet
- Wireless System For Remote Monitoring of Oxygen Saturation and Heart RateDocument4 pagesWireless System For Remote Monitoring of Oxygen Saturation and Heart RatecfunnyxNo ratings yet
- Lumos: An Open-Source Device For Wearable Spectroscopy ResearchDocument24 pagesLumos: An Open-Source Device For Wearable Spectroscopy ResearchSamuele AltrudaNo ratings yet
- SVD 4Document13 pagesSVD 4myczhNo ratings yet
- Contactless Vital Sign Monitoring System For Heart and Respiratory Rate Measurements With Motion Compen (4487)Document21 pagesContactless Vital Sign Monitoring System For Heart and Respiratory Rate Measurements With Motion Compen (4487)Dania DoNo ratings yet
- Short-Range Vital Signs SensinDocument19 pagesShort-Range Vital Signs SensinyanivNo ratings yet
- Dynamic Fine-Grained Localization in Ad-Hoc Networks of SensorsDocument14 pagesDynamic Fine-Grained Localization in Ad-Hoc Networks of SensorsHarshNo ratings yet
- Energy Efficient and Scheduling Techniques For Increasing Life Time in Wireless Sensor NetworksDocument8 pagesEnergy Efficient and Scheduling Techniques For Increasing Life Time in Wireless Sensor NetworksIAEME PublicationNo ratings yet
- Boe 10 11 5940Document12 pagesBoe 10 11 5940puma flyerNo ratings yet
- ElectronicsLetters1 27 2008Document3 pagesElectronicsLetters1 27 2008mohamad hajimirzaieNo ratings yet
- Sensors: Dual-Frequency Piezoelectric Transducers For Contrast Enhanced Ultrasound ImagingDocument18 pagesSensors: Dual-Frequency Piezoelectric Transducers For Contrast Enhanced Ultrasound ImagingTung ManhNo ratings yet
- Wu 2016Document9 pagesWu 2016yanivNo ratings yet
- Broadband Discrete-Level Excitations For Improved Extraction of Information in Bioimpedance MeasurementsDocument15 pagesBroadband Discrete-Level Excitations For Improved Extraction of Information in Bioimpedance MeasurementsThành PhạmNo ratings yet
- Heart Rate Detection From Impedance PlethysmographDocument7 pagesHeart Rate Detection From Impedance PlethysmographIsabel A. Morales L.No ratings yet
- Basic Principle and Practical Implementation of Near-Infrared Spectroscopy (NIRS)Document22 pagesBasic Principle and Practical Implementation of Near-Infrared Spectroscopy (NIRS)Calvin Yuri PietersNo ratings yet
- A Framework On The Performance Analysis of Cooperative WBANsDocument37 pagesA Framework On The Performance Analysis of Cooperative WBANsMohammed AliNo ratings yet
- Non-Invasive RF Sensing For Detecting Breathing Abnormalities Using Software Defined RadiosDocument8 pagesNon-Invasive RF Sensing For Detecting Breathing Abnormalities Using Software Defined RadiosvithenNo ratings yet
- A Weighted Moving Average-Based Approach For Cleaning Sensor DataDocument25 pagesA Weighted Moving Average-Based Approach For Cleaning Sensor DataSvastitsNo ratings yet
- Time-Frequency Analysis of Long Range UltrasonicDocument8 pagesTime-Frequency Analysis of Long Range UltrasonicNguyễn Tường MinhNo ratings yet
- Opnea Sleep DetectionDocument12 pagesOpnea Sleep DetectionLohith MNo ratings yet
- Probabilistic Estimation of The Number of Frequency-Hopping TransmittersDocument9 pagesProbabilistic Estimation of The Number of Frequency-Hopping TransmittersTung Thanh LeNo ratings yet
- Railway Security Through The Use of Wireless Sensor Networks Based On Fuzzy LogicDocument11 pagesRailway Security Through The Use of Wireless Sensor Networks Based On Fuzzy LogicMehanathan Maggie MikeyNo ratings yet
- Cancellation of Unwanted Doppler Radar Sensor Motion Using Empirical Mode DecompositionDocument8 pagesCancellation of Unwanted Doppler Radar Sensor Motion Using Empirical Mode DecompositionJeong-geun KimNo ratings yet
- VLSI LAB Manual 2014 PDFDocument67 pagesVLSI LAB Manual 2014 PDFraghvendrmNo ratings yet
- Wrestling PDFDocument1 pageWrestling PDFraghvendrmNo ratings yet
- Calender 2014-15 Odd Sem - Final PDFDocument1 pageCalender 2014-15 Odd Sem - Final PDFraghvendrmNo ratings yet
- CommunicationDocument62 pagesCommunicationraghvendrmNo ratings yet
- ECE 4110 - Sequential Logic Design Lecture #15: AgendaDocument7 pagesECE 4110 - Sequential Logic Design Lecture #15: AgendaraghvendrmNo ratings yet
- Multiple Choice QuestionsDocument11 pagesMultiple Choice QuestionsraghvendrmNo ratings yet
- Malaria: Jonathan Kidd Jennifer Koehl Heather Louch Edwin Wong Penelope WorthingtonDocument10 pagesMalaria: Jonathan Kidd Jennifer Koehl Heather Louch Edwin Wong Penelope WorthingtonraghvendrmNo ratings yet
- Chapter - 5 Multiprocessors and Thread-Level Parallelism: A Taxonomy of Parallel ArchitecturesDocument41 pagesChapter - 5 Multiprocessors and Thread-Level Parallelism: A Taxonomy of Parallel ArchitecturesraghvendrmNo ratings yet
- Keil Tutorial v2Document12 pagesKeil Tutorial v2raghvendrmNo ratings yet
- 01.MSP430 Workshop RegistrationDocument2 pages01.MSP430 Workshop RegistrationraghvendrmNo ratings yet
- Mechanism For DiffractionDocument13 pagesMechanism For DiffractionraghvendrmNo ratings yet
- Lecture 1Document42 pagesLecture 1raghvendrmNo ratings yet
- WBUT - Applied Electronics & Instrumentation Engineering Syllabus OldDocument36 pagesWBUT - Applied Electronics & Instrumentation Engineering Syllabus Oldrubel_here2000100% (1)
- Mahesh Marikatti: AddressDocument4 pagesMahesh Marikatti: AddressraghvendrmNo ratings yet
- 6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryDocument5 pages6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryParameswaran ManiNo ratings yet
- Msds UreaDocument5 pagesMsds UreaHunterlan Register FilanNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- VIPER22ADocument21 pagesVIPER22AanawintaNo ratings yet
- Yangon Thanlyin Bridge 4Document50 pagesYangon Thanlyin Bridge 4ကိုနေဝင်း100% (4)
- GR8313 GrenergyDocument9 pagesGR8313 GrenergyAngel Luis Aquino GonzalezNo ratings yet
- Introduction To Privatisation and Liberalisation in India: by Anmol SharmaDocument10 pagesIntroduction To Privatisation and Liberalisation in India: by Anmol SharmaAnmol SharmaNo ratings yet
- PersonificationDocument33 pagesPersonificationShane Pineda100% (2)
- C21 - Curriculum Diploma in Mechanical EngineeringDocument118 pagesC21 - Curriculum Diploma in Mechanical EngineeringsathishkandulaNo ratings yet
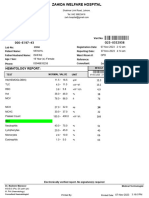
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- Australian Standard: Roof TilesDocument10 pagesAustralian Standard: Roof TilesVeetoau Joseph100% (1)
- Product Range: Trelleborg Se Aling SolutionsDocument39 pagesProduct Range: Trelleborg Se Aling SolutionssandeepNo ratings yet
- Chapter No.1 Meat CookeryDocument15 pagesChapter No.1 Meat CookeryKrishna Chaudhary0% (1)
- Construction Method (PICC)Document2 pagesConstruction Method (PICC)rheymar diwaNo ratings yet
- Bernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeDocument14 pagesBernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeSaravanan MathiNo ratings yet
- AB 14 para Tranzystorow DarlingtonaDocument23 pagesAB 14 para Tranzystorow DarlingtonavengalamahenderNo ratings yet
- Code & EthicsDocument9 pagesCode & EthicsEjaz AhmedNo ratings yet
- Generalized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsDocument4 pagesGeneralized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsMohaimen UzzamanNo ratings yet
- E BookDocument64 pagesE BookWaqar HassanNo ratings yet
- Lucas Generator and Control Box TestsDocument28 pagesLucas Generator and Control Box TestssunhuynhNo ratings yet
- Yaesu FT-1802 Operating ManualDocument88 pagesYaesu FT-1802 Operating ManualYayok S. AnggoroNo ratings yet
- National Green Tech PolicyDocument3 pagesNational Green Tech Policyalexcus1539100% (1)
- Womb World Mandala Reflections of The BuDocument11 pagesWomb World Mandala Reflections of The BuLenka MladenovićNo ratings yet
- 1st Year Chemistry Sc1 ChemistryDocument896 pages1st Year Chemistry Sc1 Chemistrybiranchi satapathyNo ratings yet
- Manual Spare Parts DB540!72!07Document124 pagesManual Spare Parts DB540!72!07Gustavo CarvalhoNo ratings yet






































































































Download as pdf or txt
You might also like
- VMC Series Vertical Machining Centers: Operator'S ManualDocument176 pagesVMC Series Vertical Machining Centers: Operator'S Manualcafetux100% (2)
- Grammar Bank 3 1Document6 pagesGrammar Bank 3 1Anahit GalstyanNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- References ASEAN2Document3 pagesReferences ASEAN2M IrwaniNo ratings yet
- Implementation and Analysis of Respiration-Rate Estimation Using Impulse-Based UwbDocument7 pagesImplementation and Analysis of Respiration-Rate Estimation Using Impulse-Based UwbVikas MehraNo ratings yet
- Remote Monitoring of Human Vital Signs Using MM-WDocument11 pagesRemote Monitoring of Human Vital Signs Using MM-W1070038825No ratings yet
- Localization, Tracking, and Imaging of Targets in Wireless Sensor Networks: An Invited ReviewDocument4 pagesLocalization, Tracking, and Imaging of Targets in Wireless Sensor Networks: An Invited ReviewPraveen KrishnaNo ratings yet
- Design and Implementation of Monitoring System For Breathing and Heart Rate Pattern Using Wifi SignalsDocument7 pagesDesign and Implementation of Monitoring System For Breathing and Heart Rate Pattern Using Wifi Signalsroboteee71421No ratings yet
- Eddy Current Based Flexible Sensor For Contactless Measurement of BreathingDocument4 pagesEddy Current Based Flexible Sensor For Contactless Measurement of BreathingA047 prince KumarNo ratings yet
- Yang 2019Document4 pagesYang 2019Swarnadip SahaNo ratings yet
- Non invasiveRespirationRateMonitoringDocument12 pagesNon invasiveRespirationRateMonitoringWekesa RobinsonNo ratings yet
- A TOA Based Positioning Technique of Medical Implanted DevicesDocument5 pagesA TOA Based Positioning Technique of Medical Implanted DevicesHadi RadNo ratings yet
- Human Body As AntennaDocument11 pagesHuman Body As AntennaSaadat RehmanNo ratings yet
- Dalal 2017Document6 pagesDalal 2017yanivNo ratings yet
- 2009-01-Personalized Feedback Based On Automatic Activity Recognition From Mixed-Source Raw Sensor DataDocument2 pages2009-01-Personalized Feedback Based On Automatic Activity Recognition From Mixed-Source Raw Sensor DataHarm op den AkkerNo ratings yet
- MS RapidHRV Resubmission Clean V2Document28 pagesMS RapidHRV Resubmission Clean V2wmasyraf4No ratings yet
- Inner Bounds On Performance of Radar and Communications Co-ExistenceDocument11 pagesInner Bounds On Performance of Radar and Communications Co-ExistencerallabhandiSKNo ratings yet
- 2020 - On CSI-Based Vital Sign Monitoring Using Commodity WiFiDocument27 pages2020 - On CSI-Based Vital Sign Monitoring Using Commodity WiFisyed hasan alaviNo ratings yet
- LISTS ALGS Elnahrawy04limitsDocument9 pagesLISTS ALGS Elnahrawy04limitsLi XuanjiNo ratings yet
- Spectroscopy.: Applications of Auto CorrelationDocument3 pagesSpectroscopy.: Applications of Auto CorrelationAishwarya SumaNo ratings yet
- A 2.4Ghz Non-Contact Biosensor System For Continuous Monitoring of Vital-SignsDocument29 pagesA 2.4Ghz Non-Contact Biosensor System For Continuous Monitoring of Vital-SignsShankarPrasaiNo ratings yet
- Infrasound Source and Calibration Methods in Seismic InterpretationDocument7 pagesInfrasound Source and Calibration Methods in Seismic InterpretationIJAR JOURNALNo ratings yet
- Review Article: Ultrawideband Technology in Medicine: A SurveyDocument10 pagesReview Article: Ultrawideband Technology in Medicine: A SurveyNouralhuda A HasanNo ratings yet
- Lifetime of Sensor NewtworkingDocument10 pagesLifetime of Sensor NewtworkingNaqiey LuluNo ratings yet
- RESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsDocument6 pagesRESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsMariana Córdoba HolguínNo ratings yet
- Estimation of Respiratory Rate Through Breathing AudioDocument12 pagesEstimation of Respiratory Rate Through Breathing AudioIJRASETPublicationsNo ratings yet
- SleepDocument15 pagesSleepgauravchauNo ratings yet
- RASS: A Real-Time, Accurate, and Scalable System For Tracking Transceiver-Free ObjectsDocument13 pagesRASS: A Real-Time, Accurate, and Scalable System For Tracking Transceiver-Free Objectscuong371992No ratings yet
- Deriving Heart Rate and Respiratory Rate From Pulse Oximetry DataDocument7 pagesDeriving Heart Rate and Respiratory Rate From Pulse Oximetry DataVelumani sNo ratings yet
- 10 1109@tbme 2012 2206591 PDFDocument7 pages10 1109@tbme 2012 2206591 PDFToàn LêNo ratings yet
- 00tmc00-Santagati-2561277.pdf - 7463487-AamDocument1 page00tmc00-Santagati-2561277.pdf - 7463487-AamGeneration GenerationNo ratings yet
- IEEE Paper On Wireless Sensing of Human Respiratory ParametersDocument11 pagesIEEE Paper On Wireless Sensing of Human Respiratory ParametersPrasanth YgNo ratings yet
- Final Complete VersionDocument17 pagesFinal Complete Versionviệt hưng trầnNo ratings yet
- 2023 CNN For The Real Time Monitoring of Vital S Based On IR UWB During SleepDocument15 pages2023 CNN For The Real Time Monitoring of Vital S Based On IR UWB During Sleepshireyoung717No ratings yet
- Ad Hoc Networks: Tal Marian, Osnat (Ossi) Mokryn, Yuval ShavittDocument11 pagesAd Hoc Networks: Tal Marian, Osnat (Ossi) Mokryn, Yuval ShavittJayraj SinghNo ratings yet
- Cognitive StressDocument6 pagesCognitive StressPallav DuttaNo ratings yet
- A Review On Different Technical Specifications of Respiratory Rate Monitors PDFDocument6 pagesA Review On Different Technical Specifications of Respiratory Rate Monitors PDFesatjournalsNo ratings yet
- Evaluating and Comparing Algorithms For Respiratory Motion PredictionDocument24 pagesEvaluating and Comparing Algorithms For Respiratory Motion PredictionPhil NovosadNo ratings yet
- A Wearable System For Tremor Monitoring and AnalysisDocument9 pagesA Wearable System For Tremor Monitoring and AnalysisZoran ConstantinescuNo ratings yet
- Event Sensing Dy Span 08Document12 pagesEvent Sensing Dy Span 08VigneshInfotechNo ratings yet
- Wireless System For Remote Monitoring of Oxygen Saturation and Heart RateDocument4 pagesWireless System For Remote Monitoring of Oxygen Saturation and Heart RatecfunnyxNo ratings yet
- Lumos: An Open-Source Device For Wearable Spectroscopy ResearchDocument24 pagesLumos: An Open-Source Device For Wearable Spectroscopy ResearchSamuele AltrudaNo ratings yet
- SVD 4Document13 pagesSVD 4myczhNo ratings yet
- Contactless Vital Sign Monitoring System For Heart and Respiratory Rate Measurements With Motion Compen (4487)Document21 pagesContactless Vital Sign Monitoring System For Heart and Respiratory Rate Measurements With Motion Compen (4487)Dania DoNo ratings yet
- Short-Range Vital Signs SensinDocument19 pagesShort-Range Vital Signs SensinyanivNo ratings yet
- Dynamic Fine-Grained Localization in Ad-Hoc Networks of SensorsDocument14 pagesDynamic Fine-Grained Localization in Ad-Hoc Networks of SensorsHarshNo ratings yet
- Energy Efficient and Scheduling Techniques For Increasing Life Time in Wireless Sensor NetworksDocument8 pagesEnergy Efficient and Scheduling Techniques For Increasing Life Time in Wireless Sensor NetworksIAEME PublicationNo ratings yet
- Boe 10 11 5940Document12 pagesBoe 10 11 5940puma flyerNo ratings yet
- ElectronicsLetters1 27 2008Document3 pagesElectronicsLetters1 27 2008mohamad hajimirzaieNo ratings yet
- Sensors: Dual-Frequency Piezoelectric Transducers For Contrast Enhanced Ultrasound ImagingDocument18 pagesSensors: Dual-Frequency Piezoelectric Transducers For Contrast Enhanced Ultrasound ImagingTung ManhNo ratings yet
- Wu 2016Document9 pagesWu 2016yanivNo ratings yet
- Broadband Discrete-Level Excitations For Improved Extraction of Information in Bioimpedance MeasurementsDocument15 pagesBroadband Discrete-Level Excitations For Improved Extraction of Information in Bioimpedance MeasurementsThành PhạmNo ratings yet
- Heart Rate Detection From Impedance PlethysmographDocument7 pagesHeart Rate Detection From Impedance PlethysmographIsabel A. Morales L.No ratings yet
- Basic Principle and Practical Implementation of Near-Infrared Spectroscopy (NIRS)Document22 pagesBasic Principle and Practical Implementation of Near-Infrared Spectroscopy (NIRS)Calvin Yuri PietersNo ratings yet
- A Framework On The Performance Analysis of Cooperative WBANsDocument37 pagesA Framework On The Performance Analysis of Cooperative WBANsMohammed AliNo ratings yet
- Non-Invasive RF Sensing For Detecting Breathing Abnormalities Using Software Defined RadiosDocument8 pagesNon-Invasive RF Sensing For Detecting Breathing Abnormalities Using Software Defined RadiosvithenNo ratings yet
- A Weighted Moving Average-Based Approach For Cleaning Sensor DataDocument25 pagesA Weighted Moving Average-Based Approach For Cleaning Sensor DataSvastitsNo ratings yet
- Time-Frequency Analysis of Long Range UltrasonicDocument8 pagesTime-Frequency Analysis of Long Range UltrasonicNguyễn Tường MinhNo ratings yet
- Opnea Sleep DetectionDocument12 pagesOpnea Sleep DetectionLohith MNo ratings yet
- Probabilistic Estimation of The Number of Frequency-Hopping TransmittersDocument9 pagesProbabilistic Estimation of The Number of Frequency-Hopping TransmittersTung Thanh LeNo ratings yet
- Railway Security Through The Use of Wireless Sensor Networks Based On Fuzzy LogicDocument11 pagesRailway Security Through The Use of Wireless Sensor Networks Based On Fuzzy LogicMehanathan Maggie MikeyNo ratings yet
- Cancellation of Unwanted Doppler Radar Sensor Motion Using Empirical Mode DecompositionDocument8 pagesCancellation of Unwanted Doppler Radar Sensor Motion Using Empirical Mode DecompositionJeong-geun KimNo ratings yet
- VLSI LAB Manual 2014 PDFDocument67 pagesVLSI LAB Manual 2014 PDFraghvendrmNo ratings yet
- Wrestling PDFDocument1 pageWrestling PDFraghvendrmNo ratings yet
- Calender 2014-15 Odd Sem - Final PDFDocument1 pageCalender 2014-15 Odd Sem - Final PDFraghvendrmNo ratings yet
- CommunicationDocument62 pagesCommunicationraghvendrmNo ratings yet
- ECE 4110 - Sequential Logic Design Lecture #15: AgendaDocument7 pagesECE 4110 - Sequential Logic Design Lecture #15: AgendaraghvendrmNo ratings yet
- Multiple Choice QuestionsDocument11 pagesMultiple Choice QuestionsraghvendrmNo ratings yet
- Malaria: Jonathan Kidd Jennifer Koehl Heather Louch Edwin Wong Penelope WorthingtonDocument10 pagesMalaria: Jonathan Kidd Jennifer Koehl Heather Louch Edwin Wong Penelope WorthingtonraghvendrmNo ratings yet
- Chapter - 5 Multiprocessors and Thread-Level Parallelism: A Taxonomy of Parallel ArchitecturesDocument41 pagesChapter - 5 Multiprocessors and Thread-Level Parallelism: A Taxonomy of Parallel ArchitecturesraghvendrmNo ratings yet
- Keil Tutorial v2Document12 pagesKeil Tutorial v2raghvendrmNo ratings yet
- 01.MSP430 Workshop RegistrationDocument2 pages01.MSP430 Workshop RegistrationraghvendrmNo ratings yet
- Mechanism For DiffractionDocument13 pagesMechanism For DiffractionraghvendrmNo ratings yet
- Lecture 1Document42 pagesLecture 1raghvendrmNo ratings yet
- WBUT - Applied Electronics & Instrumentation Engineering Syllabus OldDocument36 pagesWBUT - Applied Electronics & Instrumentation Engineering Syllabus Oldrubel_here2000100% (1)
- Mahesh Marikatti: AddressDocument4 pagesMahesh Marikatti: AddressraghvendrmNo ratings yet
- 6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryDocument5 pages6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryParameswaran ManiNo ratings yet
- Msds UreaDocument5 pagesMsds UreaHunterlan Register FilanNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- VIPER22ADocument21 pagesVIPER22AanawintaNo ratings yet
- Yangon Thanlyin Bridge 4Document50 pagesYangon Thanlyin Bridge 4ကိုနေဝင်း100% (4)
- GR8313 GrenergyDocument9 pagesGR8313 GrenergyAngel Luis Aquino GonzalezNo ratings yet
- Introduction To Privatisation and Liberalisation in India: by Anmol SharmaDocument10 pagesIntroduction To Privatisation and Liberalisation in India: by Anmol SharmaAnmol SharmaNo ratings yet
- PersonificationDocument33 pagesPersonificationShane Pineda100% (2)
- C21 - Curriculum Diploma in Mechanical EngineeringDocument118 pagesC21 - Curriculum Diploma in Mechanical EngineeringsathishkandulaNo ratings yet
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- Australian Standard: Roof TilesDocument10 pagesAustralian Standard: Roof TilesVeetoau Joseph100% (1)
- Product Range: Trelleborg Se Aling SolutionsDocument39 pagesProduct Range: Trelleborg Se Aling SolutionssandeepNo ratings yet
- Chapter No.1 Meat CookeryDocument15 pagesChapter No.1 Meat CookeryKrishna Chaudhary0% (1)
- Construction Method (PICC)Document2 pagesConstruction Method (PICC)rheymar diwaNo ratings yet
- Bernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeDocument14 pagesBernoulli's Principle: Exert Less Force On Surfaces They Are Flowing Along. Little Did HeSaravanan MathiNo ratings yet
- AB 14 para Tranzystorow DarlingtonaDocument23 pagesAB 14 para Tranzystorow DarlingtonavengalamahenderNo ratings yet
- Code & EthicsDocument9 pagesCode & EthicsEjaz AhmedNo ratings yet
- Generalized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsDocument4 pagesGeneralized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsMohaimen UzzamanNo ratings yet
- E BookDocument64 pagesE BookWaqar HassanNo ratings yet
- Lucas Generator and Control Box TestsDocument28 pagesLucas Generator and Control Box TestssunhuynhNo ratings yet
- Yaesu FT-1802 Operating ManualDocument88 pagesYaesu FT-1802 Operating ManualYayok S. AnggoroNo ratings yet
- National Green Tech PolicyDocument3 pagesNational Green Tech Policyalexcus1539100% (1)
- Womb World Mandala Reflections of The BuDocument11 pagesWomb World Mandala Reflections of The BuLenka MladenovićNo ratings yet
- 1st Year Chemistry Sc1 ChemistryDocument896 pages1st Year Chemistry Sc1 Chemistrybiranchi satapathyNo ratings yet
- Manual Spare Parts DB540!72!07Document124 pagesManual Spare Parts DB540!72!07Gustavo CarvalhoNo ratings yet