IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 12 Ver. VI (Dec. 2014), PP 83-86
www.iosrjournals.org
Gangrenous Sigmoid Volvulus A Case Report with review of
literature
Shekar Y Tati1, Ganapathi Puranik1, Chidananda KV1 Karthikeyan K2 Somdeep
Ghosh2, Harris Mohammed P2, Akshay Pai2 , Senthilnathan K2, Venkataramana
G2, Navya BN3
1Professor, 2Post graduate, department of general surgery. 3Assistant professor, department of pathology.KVG
Medical College & Hospital, Sullia- DK, Karnataka, India.
Abstract:
Sigmoid volvulus is a life threatening surgical emergency which demands early surgical
intervention. The condition is prevalent all over the world. Both sexes can be involved but more common in
males. Mostly it is a disease of elderly males but can occur in neonates to young individuals. The condition
presents in two distinct form gangrenous and non gangrenous sigmoid volvulus. Gangrenous volvulus is
associated with high morbidity.
Volvulus patient presents with pain, distension of abdomen and absolute constipation. Plain X-ray erect
abdomen will give us definite diagnosis. In doubtful cases double contrast barium enema will clinch the
diagnosis. In non gangrenous sigmoid volvulus sigmoidopexy either by endoscopic or open surgery is the
procedure of choice. Otherwise sigmoid resection with end to end anastomosis is a definite treatment of choice.
In gangrenous sigmoid volvulus, Hartmann procedure with end colostomy is the safe and life saving procedure.
We had a case of gangrenous sigmoid volvulus presented with pain, distension and absolute constipation with
toxic symptoms. After taking X-ray erect abdomen the case was diagnosed as volvulus sigmoid. Hartmanns
procedure was done after patient was resuscitated. Patient recovered well and discharged with a plan to close
the colostomy after two months. We wish to present this case because it is a life threatening condition, death is
certain if not treated early. We reviewed the literature regarding type of treatment since every surgeon is having
his own line of approach to the problem.
Key words: Colostomy, Digital rectal examination DRE, Gangrenous sigmoid, Hartmanns procedure and
Sigmoidopexy.
I.
Introduction
Sigmoid volvulus is a life threatening condition. It is one of the common surgical emergencies all over
the world. It accounts 7-10 % of all intestinal obstructions [1, 2, and 3]. The condition is most common in
African and Indian population, relatively rare in western population [3, 4]. Sigmoid volvulus is common in both
sexes, but generally it is a disease of elderly male but can present in young individuals including neonates since
congenitally long and narrowed mesentery is prime cause for volvulus [5].
Pain, distension of abdomen and absolute constipation is the hall mark of symptoms. The patient who
presents late may have complicated gangrenous sigmoid associated with high mortality [6, 7, and 8]. X-Ray
erect abdomen is diagnostic where it shows as bent inner tube sign or coffee bean sign. It presents in two
distinct forms non gangrenous and gangrenous sigmoid volvulus. Resection and primary end to end anastomois
is the treatment for non gangrenous sigmoid volvulus. Hartmanns procedure is the treatment of choice for
gangrenous sigmoid volvulus.
II.
Case report
45 year old male presented with constipation for three days, abdominal distension two days and pain
one day duration. No h/o vomiting. On examination abdomen was distended and distension was increasing in
size. Distension was more in the upper abdomen than the lower abdomen. Maximum tenderness was present
over left ileac fossa. No rigidity or guarding was present. Bowel sounds were sluggish. No free fluid was found
in the abdomen. No organomegaly. On DRE rectum was empty and was ballooned. Our provisional diagnosis
was volvulus sigmoid because of asymmetrical distension of abdomen and increasing distension. Diagnosis was
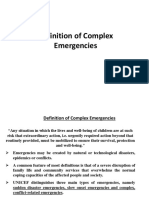
confirmed by plain X-ray erect abdomen was showing distended colonic loops present in the upper part of the
left hypochondrium with coffee bean bent inner tube appearance (fig.1). But usually the distended loops are
present in the right hypochondriem. We suspected gangrene since patient was presenting with toxic symptoms
like tachycardia, tachypnea and hypotension.
DOI: 10.9790/0853-131268386
www.iosrjournals.org
83 | Page
Gangrenous Sigmoid Volvulus A Case Report with review of literature
Figure 1 Erect abdomen X-ray showing distended loops of large bowel aggregated in left hypochondrium with
some of the loops showing a coffee been appearance
After resuscitation under general anaesthesia abdomen was opened by midline incision. Huge dilated
bluish black sigmoid colon was protruding out through the incision (fig.2). Twisted sigmoid was delivered out
of abdomen and it was untwisted. Sigmoid colon was having narrow mesocolon and twisted on its narrow
mesentery. Sigmoid was still bluish black in colour with thrombosed non pulsating vessels (fig.3).
Sigmoidectomy was done (Hartmanns operation) with proximal end colostomy, primary end to end
anastomosis was differed since sigmoid was gangrenous.
Figure 2 Distended gangrenous sigmoid colon coming out of the incision.
Figure 3. Showing narrow mesentery with thrombosed vessels.
III.
Discussion
Sigmoid volvulus is a life threatening condition accounts 5-7% of all intestinal obstruction. Sigmoid
volvulus is third most common cause of large bowel obstruction and common all over the world but more
common in Africa, India and east European countries [3, 4]. Generally it is disease of elderly male but females
can have sigmoid volvulus as well as young individuals and neonates can get effected [5, 6, 7, and 8]. It
DOI: 10.9790/0853-131268386
www.iosrjournals.org
84 | Page
Gangrenous Sigmoid Volvulus A Case Report with review of literature
associates high mortality 20-30%. Mortality depends on time of onset and arrival to hospital. Mortality is much
higher if patient presenting with gangrene of the sigmoid [6]. Mortality is still high if patient presents with
perforation. Death is certain if not intervened in time.
Exact aetiology is not known. Most of the authors claim that it is an acquired condition but per
operatively there is long sigmoid mesocolon with proximal narrowing which gives us a concept of congenital
problem. The narrowest portion of sigmoid mesocolon is the site of torsion. The second precipitating cause is
loaded sigmoid with fecal matter which encourages the segment to twist on its mesentery which gives us a
concept of acquired condition. Clinically more number of patients is elderly, which supports the concept of
acquired condition, but it is also seen in young individuals, infants and neonates [7, 8] which are in favour of
congenital condition. Patient gives h/o chronic constipation and high residue diet encourages constipation.
Congenital long mesocolon and acquired constipation seems to be cause for sigmoid vovulus in India rather than
psychiatric problems. Long mesocolon also delays the faecal evacuation which leads to chronic constipation.
Patient presents with pain and distension of the abdomen with absolute constipation. Pain is in the
lower abdomen more towards the left iliac fossa. Pain is localised, continuous and agonising. Pain can also be a
colicky type from distended sigmoid. Distension is more on upper abdomen than the lower and it is a
characteristic feature of sigmoid volvulus. Tenderness is present all over the abdomen but more in the left ileac
fossa. Resonance note is present more on upper abdomen on percussion. Bowel sounds are high pitched but as
time passes on bowel sounds are usually sluggish. Patient presents with toxic symptoms such as tachycardia,
tachypnea with elevated temperature if sigmoid colon presents with gangrene.
Plain X-ray erect abdomen is diagnostic as it shows pneumatic distended loops of large bowel mostly
on right upper quadrant or in left upper quadrant. In our case dilated loops were located in left upper quadrant.
Loss of haustrational foldings of colon is seen. There is inner tube bent sign or coffee bean sign present on
plain x-ray and it is diagnostic.
Before surgery patient is resuscitated well, dehydration and serum electrolytes are corrected. Blood
grouping and Rh typing is carried out since patient may require blood transfusion after bowel excision. Upper
GI tract is decompressed with nasogastric tube. Foleys catheter is passed to assess the urine output.
There are few surgical options are available for volvulus sigmoid like resection and primary
anastomosis, Hartmanns procedure, mesosigmoidopexy and endoscopic sigmoidopexy. Surgical option
depends on whether the sigmoid volvulus is simple volvulus without gangrene or volvulus with gangrene.
Resection with primary anastomois is the treatment in non gangrenous sigmoid volvulus. It demands on
table preparation of colon since colon is loaded with faecal matter. On table preparation contaminate the
peritoneal cavity as spillage is present which leads to wound sepsis sometime peritonitis. There can be a chance
of anastomotic leak due to incomplete on table preperation of colon [9]. Anastomotic leak leads to faecal
peritonitis with increased morbidity and mortality. Patient has to be kept nil per oral for prolonged period.
Another procedure is detorsion followed by sigmoidopexy particularly when surgeon is inexperienced.
It can be done by endoscopy or by open methods [10].This avoids peritoneal soiling and patient life is secured.
But it is not a treatment of the problem rather it is relief of the problem since it is not removing the cause [11].
Treatment is differed for gangrenous sigmoid volvulus since it associates with high mortality
accounting 10-40% [7, 8]. Excision and end to end anastomosis is not entertained because it is difficult to assess
normal viable bowel. If viable, wall is edematous due to accumulation of inflammatory fluid leaving more
chance of stomal leakage. General condition of the patient is already in jeopardy. Keeping all these factors in
view Hartmann operation is the procedure of choice i.e. resection of sigmoid volvulus with proximal loop end
colostomy and distal loop is closed and left in the pelvis.
What we feel, detorsion and sigmoidopexy is not the solution for the problem. Patient is left for another
surgery since volvulus invariably recurs after sometime. If resection is attempted proximal dysfunctiong
colostomy is mandate since anastomotic leak associate with high morbidity and mortality. Hartmanns
procedure is golden option for gangrenous sigmoid volvulus.
IV.
Conclusion
Volvulus sigmoid is relatively common surgical emergency. It is common from neonate to elderly
people. It is diagnosed clinically and can be confirmed by plain radiograph. Few treatment options are available.
Detorsion and primary excision of sigmoid and end to end anastomosis is the treatment of choice in non
gangrenous sigmoid volvulus. Yet chance of leak is high in primary anastomosis since colon is not prepared.
Hartmann procedure is golden option in gangrenous volvulus of the sigmoid.
Reference
[1].
[2].
Udezue N. Sigmoid volvulus in Kaduna, Nigeria. Diseases of the Colon and Rectum. 1990; 33:647 649. [PubMed: 2376220]
SchagenVanLeeuwen J. Sigmoid volvulus in a West African population. Diseases of the Colon and Rectum. 1985; 28:712 716.
[PubMed: 4053876]
DOI: 10.9790/0853-131268386
www.iosrjournals.org
85 | Page
Gangrenous Sigmoid Volvulus A Case Report with review of literature
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
Lal S, Morgenstern R, Vinjirayer E, Matin A. Sigmoid volvulus an update. Gastrointestinal endoscopy clinics of North America.
2006; 16:175187. [PubMed: 16546032]
Ballantyne G, Brandner M, Beart R, Ilstrup D. Volvulus of the colon. Incidence and mortality. Annals of Surgery. 1985; 202:83
91. [PubMed: 4015215]
Valentine Pastore, Angela Basile, Raffaella Cocomazzi, Marlena Pastore, Fabio Bartoli. Sigmoid volvulus in a neonate: Case report
and review of literature; African J ournal of paediatric surgery Oct/Decm 2013 (10) issue 4; 390-392.
Raveenthiran V. Restorative resection of unprepared left-colon in gangrenous versus viable sigmoid volvulus. International Journal
of Colorectal Diseases. 2004; 19:258263.
Grossmann EM, Longo WE, Stratton MD, et al. Sigmoid volvulus in Department of Veterans Affairs Medical Centers. Dis Colon
Rectum 2000; 43:4148.
Connolly S, Brannigan AE, Heffeman E, Hyland JM. Sigmoid volvulus: a 10-year-audit. Ir J Med Sci 2002; 171:2167.
Atamanalp SS, Yildirgan MI, Basoglu M, et al. Sigmoid colon volvulus in children: review of 19 cases. Pediatr Surg Int 2004;
20:4925.
Muyco A, Kushner A, Mvula C. Management of sigmoid volvulus at a tertiary care hospital in Africa. East and Central African
Journal of Surgery. 2005; 10:105.
Northeast AD, Dennison AR, Lee EG. Sigmoid volvulus: new thoughts on the epidemiology. Dis Colon Rectum 1984; 27:2601.
DOI: 10.9790/0853-131268386
www.iosrjournals.org
86 | Page
You might also like
- Self-I-Dentity Through Ho'oponoponoDocument5 pagesSelf-I-Dentity Through Ho'oponoponoTanya McCracken100% (1)
- Disposition of Wyoming Wild Horses PDFDocument44 pagesDisposition of Wyoming Wild Horses PDFfreewildhorsesNo ratings yet
- Surgical Posting - Testicular TumoursDocument16 pagesSurgical Posting - Testicular TumoursDiyana ZatyNo ratings yet
- Diseases of The Peritoneal CavityDocument19 pagesDiseases of The Peritoneal CavityJoanna BisNo ratings yet
- Open Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective StudyDocument3 pagesOpen Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective Study'Adil MuhammadNo ratings yet
- Testicular TumorDocument56 pagesTesticular TumorMuhammad MakkiNo ratings yet
- VOLVULUS PathoDocument2 pagesVOLVULUS Pathochelle_asenjoNo ratings yet
- Idiopathic Non Neoplastic Salivary Gland DiseasesDocument33 pagesIdiopathic Non Neoplastic Salivary Gland Diseasesgud4nothingNo ratings yet
- Current Concepts in Hemorrhagic ShockDocument12 pagesCurrent Concepts in Hemorrhagic ShockktorooNo ratings yet
- Synchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaDocument6 pagesSynchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaKhaled MonazeaNo ratings yet
- Tension-Free Repair Versus Bassini Technique For SDocument5 pagesTension-Free Repair Versus Bassini Technique For STomus ClaudiuNo ratings yet
- Testicular Tumours 2020Document55 pagesTesticular Tumours 2020Ramesh ReddyNo ratings yet
- Groin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYDocument39 pagesGroin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYMuhammad Waqar UlfatNo ratings yet
- 7 Adverse Reactions To TransfusionDocument8 pages7 Adverse Reactions To Transfusioncryztelle2720027476No ratings yet
- Retro Peritoneal TumorDocument37 pagesRetro Peritoneal TumorHafizur RashidNo ratings yet
- Ulcerative Colitis NclexDocument33 pagesUlcerative Colitis NclexKrishna SapkotaNo ratings yet
- Hernia - Hernioplasty With Bilayer Polypropylene Mesh PDFDocument4 pagesHernia - Hernioplasty With Bilayer Polypropylene Mesh PDFAnonymous YLmmme4XX0No ratings yet
- Blood Transfusion ReactionsDocument3 pagesBlood Transfusion ReactionsANDREW MWITINo ratings yet
- Testicular Tumours: Vinod JainDocument13 pagesTesticular Tumours: Vinod JainChanel Van Der WesthuizenNo ratings yet
- OP Sliding & Strangulated Hernia & OrchiectomyDocument8 pagesOP Sliding & Strangulated Hernia & OrchiectomyDeepika ChaudharyNo ratings yet
- Treatment: Bassini RepairDocument5 pagesTreatment: Bassini RepairziehonkNo ratings yet
- What Is Oxygen TheraphyDocument4 pagesWhat Is Oxygen TheraphyitsmekringNo ratings yet
- Retroperitoneal MassDocument22 pagesRetroperitoneal Massapi-434838777No ratings yet
- 04 Esophageal TumorsDocument36 pages04 Esophageal TumorsDetty NoviantyNo ratings yet
- Metabolic Response in InjuryDocument27 pagesMetabolic Response in InjuryAhmed Kh. Abu Warda100% (1)
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Energy Devices in Surgery: Surg LT CDR K S PatelDocument32 pagesEnergy Devices in Surgery: Surg LT CDR K S PatelMuhammad ShahidNo ratings yet
- Subtotal ThyroidectomyDocument26 pagesSubtotal ThyroidectomyJimmyNo ratings yet
- Prosthetic Material in Inguinal Hernia RepairDocument23 pagesProsthetic Material in Inguinal Hernia RepairAnca NicaNo ratings yet
- Amputation in Lower LimbsDocument35 pagesAmputation in Lower LimbsSamNo ratings yet
- Bowel AnastomosisDocument30 pagesBowel AnastomosismrashaiedehNo ratings yet
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDocument36 pagesColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Electrosurgery & Principles of Diathermy: DR Nilay Biswas Postgraduate ResidentDocument15 pagesElectrosurgery & Principles of Diathermy: DR Nilay Biswas Postgraduate ResidentRajarshi KumarNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- HerniaDocument16 pagesHerniaVetrivel TamizhNo ratings yet
- Back To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopDocument43 pagesBack To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopBima Achmad100% (1)
- Varicose Veins CaseDocument16 pagesVaricose Veins Casebenak shivalingappaNo ratings yet
- Inguinal Hernia Surgery OverviewDocument15 pagesInguinal Hernia Surgery OverviewWarda BajwaNo ratings yet
- Premalignant & Malignant Disease of CervixDocument64 pagesPremalignant & Malignant Disease of CervixDegefaw BikoyNo ratings yet
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDocument43 pagesHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseNo ratings yet
- I Flat Meshes For Inguinal and Ventral Hernias V 2Document30 pagesI Flat Meshes For Inguinal and Ventral Hernias V 2bogdanoti100% (1)
- What Is The Differential Diagnosis For The Breast Mass in An Adolescent?Document4 pagesWhat Is The Differential Diagnosis For The Breast Mass in An Adolescent?theodore_estradaNo ratings yet
- Comparative Study of Endovenous Laser AblationDocument3 pagesComparative Study of Endovenous Laser AblationabdulNo ratings yet
- Precancerous Conditions of Oral CavityDocument80 pagesPrecancerous Conditions of Oral Cavitylarisabrinza12No ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- EAU Guidelines On: Testicular CancerDocument62 pagesEAU Guidelines On: Testicular CancerFaheem AfridiNo ratings yet
- Achalasia - AHNDocument31 pagesAchalasia - AHNZimran SalimNo ratings yet
- New Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSDocument21 pagesNew Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSArturo Javier FuentesNo ratings yet
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- The Surgical Anatomy of The Nerve Laryngeal RecurrensDocument2 pagesThe Surgical Anatomy of The Nerve Laryngeal RecurrensvaNo ratings yet
- Reconstruction in Fournier GangreneDocument40 pagesReconstruction in Fournier GangreneAnggie MutmainnahNo ratings yet
- CA EsophagusDocument37 pagesCA EsophagusElandha PutriNo ratings yet
- Abdominal LumpDocument19 pagesAbdominal LumpDeepak AnNo ratings yet
- Recent Advances in Laser TechnologyDocument5 pagesRecent Advances in Laser TechnologyIOSRjournalNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- Anastomosis IntestinalDocument3 pagesAnastomosis IntestinalWaqas ChaudhryNo ratings yet
- Thyroidectomy Morbidities:: Preventions & InterventionsDocument52 pagesThyroidectomy Morbidities:: Preventions & InterventionsAlfonso DanacNo ratings yet
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionDocument8 pagesSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GNo ratings yet
- Early Experiences of a First Generation Jewish South AfricanFrom EverandEarly Experiences of a First Generation Jewish South AfricanNo ratings yet
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocument10 pagesEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Necessary Evils of Private Tuition: A Case StudyDocument6 pagesNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)No ratings yet
- Factors Affecting Success of Construction ProjectDocument10 pagesFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)No ratings yet
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocument5 pagesYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocument2 pagesComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameDocument9 pagesDesign and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactDocument11 pagesDesign and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactInternational Organization of Scientific Research (IOSR)No ratings yet
- Fatigue Analysis of A Piston Ring by Using Finite Element AnalysisDocument4 pagesFatigue Analysis of A Piston Ring by Using Finite Element AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- TNPSC Science Model Question Paper PDF Download PDFDocument11 pagesTNPSC Science Model Question Paper PDF Download PDFTamizh IniyanNo ratings yet
- Plag Test-Cardio PDFDocument10 pagesPlag Test-Cardio PDFAsmit UpadhyayNo ratings yet
- KMIslam ELISADocument9 pagesKMIslam ELISADlstmxkakwldrl VousmevoyezNo ratings yet
- "Robodoc". The New Era of The Medical World.Document18 pages"Robodoc". The New Era of The Medical World.Merey SabdenaliyevaNo ratings yet
- Research Question: Does The Increasing Concentration of Natural Food Color Crocin (In Saffron)Document15 pagesResearch Question: Does The Increasing Concentration of Natural Food Color Crocin (In Saffron)RitikaFandaNo ratings yet
- Case Study Beauty Health and Wellness IndustryDocument31 pagesCase Study Beauty Health and Wellness IndustrySimran JainNo ratings yet
- Chilli ReportDocument12 pagesChilli ReportEba AliNo ratings yet
- E3 QuestionsDocument5 pagesE3 Questionsshodhan shettyNo ratings yet
- Demam Berdarah Dengue Pada Anak: MustaringDocument70 pagesDemam Berdarah Dengue Pada Anak: MustaringpipitNo ratings yet
- Genetics TodayDocument342 pagesGenetics TodayJaqueline OdairNo ratings yet
- Gendent - jf19 - de Oliveira S IDocument5 pagesGendent - jf19 - de Oliveira S IAndreea RoxanaNo ratings yet
- Robie Harris Sell SheetDocument2 pagesRobie Harris Sell SheetCandlewick PressNo ratings yet
- Algeria Country PaperDocument9 pagesAlgeria Country PaperSandeep MahantaNo ratings yet
- Nail Bed InjuryDocument17 pagesNail Bed InjuryGunjan UpadhyayNo ratings yet
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- Artaud, Theatre & The PlagueDocument9 pagesArtaud, Theatre & The PlagueTR119No ratings yet
- Urban Design and 3 Kinds of Space-Related Epidemic DiseasesDocument6 pagesUrban Design and 3 Kinds of Space-Related Epidemic DiseasesMiguel R MoNo ratings yet
- Case Report: Immune Thrombocytopenic PurpuraDocument34 pagesCase Report: Immune Thrombocytopenic PurpuraFelinNo ratings yet
- Vasomotor Center: Abu Ahmed 2019Document19 pagesVasomotor Center: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- Clinical Diagnoses Following Zipf'S LawDocument11 pagesClinical Diagnoses Following Zipf'S LawNicolas DemidovNo ratings yet
- Leukemia in Children 15 April 2020 PDFDocument44 pagesLeukemia in Children 15 April 2020 PDFChandan KumarNo ratings yet
- Q1 - Science - LessonDocument23 pagesQ1 - Science - LessonHF ManigbasNo ratings yet
- Midterm Topics Hema 1 LecDocument37 pagesMidterm Topics Hema 1 Lec4jzbxz64kqNo ratings yet
- Chung 2016 Stop Bang QuestionnaireDocument8 pagesChung 2016 Stop Bang QuestionnaireDicka adhitya kamilNo ratings yet
- Dermatological Disorder Detection Using Machine LearningDocument4 pagesDermatological Disorder Detection Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Complex EmergenciesDocument4 pagesComplex EmergenciesPraveen Kumar JhaNo ratings yet
- SCIED3.CIERVO - Bsed Sci1-A.laboratory 3 - The Body's FrameworkDocument6 pagesSCIED3.CIERVO - Bsed Sci1-A.laboratory 3 - The Body's FrameworkIrica Mae CiervoNo ratings yet
- Research PaperDocument6 pagesResearch PaperJenny' PinedaNo ratings yet