Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- My SMART Goal UK - Big Life JournalDocument6 pagesMy SMART Goal UK - Big Life Journalacmc100% (2)
- Microwave Oven: User'S ManualDocument20 pagesMicrowave Oven: User'S ManualRuiPereiraNo ratings yet
- Welcome To: Tupi Fundamental Baptist ChurchDocument36 pagesWelcome To: Tupi Fundamental Baptist ChurchJaireh CardamaNo ratings yet
- Thespaceofk Ahler Metrics: Brief Introduction To The Classical Problems in K Ahler GeometryDocument46 pagesThespaceofk Ahler Metrics: Brief Introduction To The Classical Problems in K Ahler GeometryEliacim VelezNo ratings yet
- 30 Data SheetDocument3 pages30 Data SheetGermán AndrésNo ratings yet
- Patrol GR: GI MA EM LC EC FE CL MT Automatic Transmission AT TF PD FA RA BR ST RS BT HA EL IDXDocument2 pagesPatrol GR: GI MA EM LC EC FE CL MT Automatic Transmission AT TF PD FA RA BR ST RS BT HA EL IDXAttila SomorjaiNo ratings yet
- Programming Guide MSP 3dmj-230327-020747Document17 pagesProgramming Guide MSP 3dmj-230327-020747Pierfrancesco LucenteNo ratings yet
- Junior Agronomist - On Contract: Gujarat State Fertilizers and Chemicals LTDDocument2 pagesJunior Agronomist - On Contract: Gujarat State Fertilizers and Chemicals LTDZayn AliNo ratings yet
- Mn003557a01-Ag Enus Slr1000 Bsim NagDocument311 pagesMn003557a01-Ag Enus Slr1000 Bsim NagOscar EscobarNo ratings yet
- Election Law CasesDocument155 pagesElection Law CasesJa VillaromanNo ratings yet
- Teaching Guide 2 1 4Document58 pagesTeaching Guide 2 1 4Anu KhanNo ratings yet
- Organizational Behavior: Robbins & JudgeDocument18 pagesOrganizational Behavior: Robbins & JudgeYandex PrithuNo ratings yet
- Analysis: Is Science Killing Sport?Document3 pagesAnalysis: Is Science Killing Sport?Raunak Chakraborty (Rio)No ratings yet
- Untitled: Pandas PD OsDocument55 pagesUntitled: Pandas PD OsGustavo Cano GallegosNo ratings yet
- Code SwitchingDocument6 pagesCode SwitchingMarion Shanne Pastor CorpuzNo ratings yet
- Plumb Conc.Document28 pagesPlumb Conc.Muhammad AwaisNo ratings yet
- ECSS U AS 10C Rev.1 (3december2019)Document8 pagesECSS U AS 10C Rev.1 (3december2019)Mansoor ShahNo ratings yet
- Dynamic Memory Allocation-1Document38 pagesDynamic Memory Allocation-1Muskan AgarwalNo ratings yet
- ICT-Pedagogy Integration in MathematicsDocument11 pagesICT-Pedagogy Integration in MathematicsKaren Faye LagundayNo ratings yet
- Love of Radhe-KrishnaDocument3 pagesLove of Radhe-KrishnaavncntnNo ratings yet
- Citra Log - Txt.oldDocument57 pagesCitra Log - Txt.oldEmmanuel PeraltaNo ratings yet
- Quick Charge Device ListDocument16 pagesQuick Charge Device Listlimited0% (1)
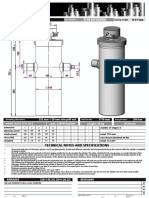
- Cilindro Penta Hydraulic PowerDocument1 pageCilindro Penta Hydraulic PowerUniversity FilesNo ratings yet
- The Union of Concerned ScientistsDocument13 pagesThe Union of Concerned ScientistsIlser ReineNo ratings yet
- Pile Load Test MethodologyDocument4 pagesPile Load Test MethodologyAkhilesh Dwivedi100% (1)
- Price List Djuragan FrozenDocument34 pagesPrice List Djuragan FrozenIsrainiNo ratings yet
- On The Roll With The Environment: June 7, 20213 Min ReadDocument3 pagesOn The Roll With The Environment: June 7, 20213 Min Readkyzel colNo ratings yet
- Ansi Asa S3.1 1999 R2008Document27 pagesAnsi Asa S3.1 1999 R2008fco2312100% (1)
- KPK fsc2 ch02 - NotesDocument33 pagesKPK fsc2 ch02 - NotesShujahatNo ratings yet
- Ebook 7 Tutorials - Cake Craft SchoolDocument45 pagesEbook 7 Tutorials - Cake Craft SchoolmariaNo ratings yet