Download as pdf or txt
You might also like
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanKatherine 'Chingboo' Leonico Laud95% (21)
- NCP TesticularDocument8 pagesNCP TesticularPrincess Gutierrez Rosita50% (2)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- STL2C6 - Support The Health and Safety of Children and Young PeopleDocument3 pagesSTL2C6 - Support The Health and Safety of Children and Young PeopleMarcela Coid100% (1)
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- NCPs For ParotidectomyDocument12 pagesNCPs For ParotidectomyCarla Manaloto50% (2)
- NCP Acute PainDocument3 pagesNCP Acute PainSatchiko Riko SakuraNo ratings yet
- NCP CholeDocument8 pagesNCP CholeAndrewAlvinTemploNo ratings yet
- NCPDocument5 pagesNCProxybabes100% (3)
- Pathway Gagal Ginjal Kronik: Intoleransi AktivitasDocument1 pagePathway Gagal Ginjal Kronik: Intoleransi AktivitasReza ApriandiNo ratings yet
- Post Operative Acute PainDocument1 pagePost Operative Acute Painالأغا محمد زكارنةNo ratings yet
- Cholecystectomy Nursing Care Plan: Post-Operative Acute PainDocument2 pagesCholecystectomy Nursing Care Plan: Post-Operative Acute PainCherald Paul C AsuncionNo ratings yet
- Cholecystectomy Nursing Care Plan: Post-Operative Acute PainDocument2 pagesCholecystectomy Nursing Care Plan: Post-Operative Acute PainCharm TanyaNo ratings yet
- Anemia NCPDocument20 pagesAnemia NCPNursidar Pascual Mukattil80% (5)
- Acute Pain Related To InjuryDocument2 pagesAcute Pain Related To InjuryErickson Caisido GarciaNo ratings yet
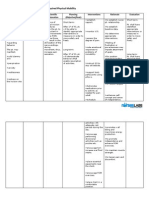
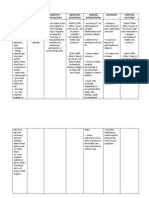
- Cholecystectomy Nursing Care Plan: Impaired Physical MobilityDocument2 pagesCholecystectomy Nursing Care Plan: Impaired Physical MobilityCharm TanyaNo ratings yet
- NCP Acute PainDocument1 pageNCP Acute PainJuan Carlo ViadoNo ratings yet
- Super Final NCPDocument16 pagesSuper Final NCPNessaly Jane PrestoNo ratings yet
- CS NCPDocument3 pagesCS NCPAllan VillanuevaNo ratings yet
- Acute Pain AGEDocument2 pagesAcute Pain AGEHarris AustriaNo ratings yet
- Impaired Physical Mobility CholecystectomyDocument2 pagesImpaired Physical Mobility CholecystectomyPrincess Danica Purcia100% (1)
- NCP Gouty ArthritisDocument21 pagesNCP Gouty ArthritisArianne Kamille Andes67% (3)
- Activity Intolerance CholecystectomyDocument2 pagesActivity Intolerance CholecystectomyPrincess Danica Purcia100% (3)
- #3 #3 Acute Pain (Preoperative)Document4 pages#3 #3 Acute Pain (Preoperative)joevi02No ratings yet
- Nursing Care PlansDocument6 pagesNursing Care PlansjessamariesabioNo ratings yet
- NURSING SCIENCE - Pre & Post Operative CareDocument61 pagesNURSING SCIENCE - Pre & Post Operative CareJiehah RudyNo ratings yet
- NCPs For ParotidectomyDocument8 pagesNCPs For ParotidectomyAcohCChao100% (1)
- 4 NCP's FinalDocument9 pages4 NCP's FinalZenel Yap100% (1)
- Nursing Management of CVA and NIDDMDocument12 pagesNursing Management of CVA and NIDDMKaloy KamaoNo ratings yet
- NCP AppendicitisDocument8 pagesNCP AppendicitisAaron_Kim_Vela_4636No ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentDocument4 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentJoseph Rodney de LeonNo ratings yet
- NCP CholehgxkDocument9 pagesNCP CholehgxkPrincess Gutierrez RositaNo ratings yet
- NCPDocument10 pagesNCPbabycheska08No ratings yet
- Case Study NCP - Forcep BirthDocument4 pagesCase Study NCP - Forcep BirthKent CruzNo ratings yet
- NCP Sicu!Document6 pagesNCP Sicu!joanne190No ratings yet
- IUFDDocument13 pagesIUFDChristopher Lontoc0% (1)
- Cue Problem Scientific Explanation Planning Interventions Rationale EvaluationDocument5 pagesCue Problem Scientific Explanation Planning Interventions Rationale EvaluationJanyn Abella ReyesNo ratings yet
- NCPDocument6 pagesNCPAngelaTrinidadNo ratings yet
- SCR 270 L & D Care PlanDocument5 pagesSCR 270 L & D Care PlanRenzo MarcosNo ratings yet
- NCPDocument12 pagesNCPJonathan Liscano100% (3)
- NCP N SOPIEDocument9 pagesNCP N SOPIEDonna DavidNo ratings yet
- NCP Pain - ArthroDocument6 pagesNCP Pain - ArthroKDnurseboyNo ratings yet
- Appendicitis Management and Nursing Care PlanDocument37 pagesAppendicitis Management and Nursing Care PlanAlva AlfaNo ratings yet
- NCP AppendectomyDocument6 pagesNCP AppendectomyDaryl Valerio Francisco100% (1)
- Independent:: Surgical Nursing, 7 TH Ed. by Black, Joyce M.Andjane Hokan Son Hawkspg.443)Document4 pagesIndependent:: Surgical Nursing, 7 TH Ed. by Black, Joyce M.Andjane Hokan Son Hawkspg.443)KenPedreso100% (1)
- PYOMYOSITISDocument12 pagesPYOMYOSITISPaolo VillaNo ratings yet
- NCP TahbsoDocument18 pagesNCP TahbsoKe EjieNo ratings yet
- Appendicitis NCPDocument3 pagesAppendicitis NCPMayaed BicolNo ratings yet
- NCP FinalDocument7 pagesNCP FinalRuss RussNo ratings yet
- 2 Acute Pain Chronic Renal Failure Nursing Care PlansDocument5 pages2 Acute Pain Chronic Renal Failure Nursing Care Plansjustin_saneNo ratings yet
- PENSAYO. NCP For Chole&myomaDocument10 pagesPENSAYO. NCP For Chole&myomaPensayo, Stephanie Keith V.No ratings yet
- Vii. Nursing Care Plan: Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesVii. Nursing Care Plan: Assessment Nursing Diagnosis Inference Planning Intervention Rationale Evaluation SubjectiveMezil NazarenoNo ratings yet
- CP AmoebaDocument3 pagesCP AmoebaJoy G. NomilNo ratings yet
- NCP TonsilitisDocument11 pagesNCP TonsilitisGra Cie50% (6)
- Intervention EdwardsDocument19 pagesIntervention EdwardsChamCham AquinoNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Holistic Pain Relief: How to ease muscles, joints and other painful conditionsFrom EverandHolistic Pain Relief: How to ease muscles, joints and other painful conditionsNo ratings yet
- 8883-Article Text-39942-1-10-20210325Document13 pages8883-Article Text-39942-1-10-20210325مالك مناصرةNo ratings yet
- Improvement of Patient Satisfaction Through Enhancement of RN Communication Skills: A Quality Improvement ProjectDocument46 pagesImprovement of Patient Satisfaction Through Enhancement of RN Communication Skills: A Quality Improvement Projectمالك مناصرةNo ratings yet
- An-Najah National University: Prepared By:-1 - Bilal Mwas 2 - Omar Abureesh 3 - Yahia AbusafiDocument47 pagesAn-Najah National University: Prepared By:-1 - Bilal Mwas 2 - Omar Abureesh 3 - Yahia Abusafiمالك مناصرةNo ratings yet
- LRDocument22 pagesLRمالك مناصرةNo ratings yet
- Survey of Skin-to-Skin Contact With Obstetrics and Pediatric NursesDocument9 pagesSurvey of Skin-to-Skin Contact With Obstetrics and Pediatric Nursesمالك مناصرةNo ratings yet
- Mgolozeli Midwives 2018Document13 pagesMgolozeli Midwives 2018مالك مناصرةNo ratings yet
- Assess The Knowledge Among Staff NursesDocument9 pagesAssess The Knowledge Among Staff Nursesمالك مناصرةNo ratings yet
- Chapter OneDocument73 pagesChapter Oneمالك مناصرةNo ratings yet
- Assessment of Nurses' Knowledge and Practice Regarding To Kangaroo Care at Neonatal Intensive Care Unit (NICU)Document11 pagesAssessment of Nurses' Knowledge and Practice Regarding To Kangaroo Care at Neonatal Intensive Care Unit (NICU)مالك مناصرةNo ratings yet
- Experience of Diabetic Patient After Amputation: Amer Saleli & Baher Ebedat, Hosam Al-Esaa & Ameen Abu HaniaDocument78 pagesExperience of Diabetic Patient After Amputation: Amer Saleli & Baher Ebedat, Hosam Al-Esaa & Ameen Abu Haniaمالك مناصرةNo ratings yet
- Theme Sub ThemesDocument9 pagesTheme Sub Themesمالك مناصرةNo ratings yet
- Table 9.1. Comparison of Freudian and Eriksonian Stages ofDocument2 pagesTable 9.1. Comparison of Freudian and Eriksonian Stages ofمالك مناصرةNo ratings yet
- AbstractDocument2 pagesAbstractمالك مناصرةNo ratings yet
- Themselves, As Opposed To The Counsellor Being AnDocument31 pagesThemselves, As Opposed To The Counsellor Being Anمالك مناصرةNo ratings yet
- Introduction and BackgroundDocument50 pagesIntroduction and Backgroundمالك مناصرة100% (1)
- Humanistic Approaches in Counselling andDocument6 pagesHumanistic Approaches in Counselling andمالك مناصرةNo ratings yet
- Informatics 07 00041 v2Document10 pagesInformatics 07 00041 v2مالك مناصرةNo ratings yet
- Effects of Occupational Stressors On Nurses' Safety Performance and Well-Being: A Within-Individual StudyDocument125 pagesEffects of Occupational Stressors On Nurses' Safety Performance and Well-Being: A Within-Individual Studyمالك مناصرةNo ratings yet
- Appendix B: Study Survey Baseline SurveyDocument5 pagesAppendix B: Study Survey Baseline Surveyمالك مناصرةNo ratings yet
- Humanistic Therapies Versus Other PsychoDocument19 pagesHumanistic Therapies Versus Other Psychoمالك مناصرةNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument18 pagesRajiv Gandhi University of Health Sciences Bangalore, Karnatakaمالك مناصرةNo ratings yet
- The Impact of Nurse Work Environment On Nurse Outcomes, Nurse-Perceived Quality of Care and Patient Safety in Saudi ArabiaDocument148 pagesThe Impact of Nurse Work Environment On Nurse Outcomes, Nurse-Perceived Quality of Care and Patient Safety in Saudi Arabiaمالك مناصرةNo ratings yet
- Structures and Functions of Urinary SystemDocument6 pagesStructures and Functions of Urinary Systemمالك مناصرةNo ratings yet
- Qureshi, SadeemDocument176 pagesQureshi, Sadeemمالك مناصرةNo ratings yet
- The Impact of Electronic Health Records On The Duration of Patients' Visits: Time and Motion StudyDocument9 pagesThe Impact of Electronic Health Records On The Duration of Patients' Visits: Time and Motion Studyمالك مناصرةNo ratings yet
- Measuring Workload of ICU Nurses With A QuestionnaDocument23 pagesMeasuring Workload of ICU Nurses With A Questionnaمالك مناصرةNo ratings yet
- Physiological Changes During PregnancyDocument6 pagesPhysiological Changes During Pregnancyمالك مناصرةNo ratings yet
- CDC, FDA Faked Covid' Testing Protocol by Using Human Cells Mixed With Common Cold Virus FragmentsDocument13 pagesCDC, FDA Faked Covid' Testing Protocol by Using Human Cells Mixed With Common Cold Virus FragmentsZamfirMarian100% (1)
- 14-Improving SVM Performance For Type II Diabetes Prediction With An Improved Non-Linear Kernel Insights From The PIMA DatasetDocument9 pages14-Improving SVM Performance For Type II Diabetes Prediction With An Improved Non-Linear Kernel Insights From The PIMA Datasetbeefypixel761No ratings yet
- The Guardian (2020.11.27) PDFDocument72 pagesThe Guardian (2020.11.27) PDFCristi CoroamaNo ratings yet
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument20 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordNurwahidah Moh WahiNo ratings yet
- NCA2Document9 pagesNCA2Ley BeltranNo ratings yet
- Afrostainfarmtech.: Onion and Garlic Production GuideDocument3 pagesAfrostainfarmtech.: Onion and Garlic Production Guidewalter mombeNo ratings yet
- Nursing Bullets Fundamentals of Nursing Reviewer Part IDocument10 pagesNursing Bullets Fundamentals of Nursing Reviewer Part IAlyanna Mabelle Peñosa MonteposoNo ratings yet
- NCP Pain DiverticulitisDocument1 pageNCP Pain DiverticulitisAdhaNo ratings yet
- Emergency Drugs Drug StudyDocument15 pagesEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- 02 Nuclear Chemistry (Part 2)Document67 pages02 Nuclear Chemistry (Part 2)Aladha SorianoNo ratings yet
- Beneficial and Effective Microorganisms (Em) : Their Applications in Sustainable AgricultureDocument17 pagesBeneficial and Effective Microorganisms (Em) : Their Applications in Sustainable Agricultureboite_testeNo ratings yet
- Expert SystemsDocument19 pagesExpert SystemsMarianneNo ratings yet
- Sudden Infant Death SyndromeDocument2 pagesSudden Infant Death Syndromeboxed juiceNo ratings yet
- Pain Management Us PharmacistDocument78 pagesPain Management Us PharmacistMarfu'ah Mar'ah100% (1)
- TaariniDocument19 pagesTaariniRuma GuptaNo ratings yet
- The Price of SilenceDocument9 pagesThe Price of Silencewamu885100% (1)
- Guidelines For Sparsh Leprosy Awareness Campaign, 2018Document2 pagesGuidelines For Sparsh Leprosy Awareness Campaign, 2018TanishNo ratings yet
- Goat LO1Document105 pagesGoat LO1Elma Acuzar50% (2)
- Global Catastrophic RiskDocument16 pagesGlobal Catastrophic RiskSajjad WarsiNo ratings yet
- S32063 Covidtempl Chandra Kanth 180521201543Document1 pageS32063 Covidtempl Chandra Kanth 180521201543Chandrakanth KhannaNo ratings yet
- Updated IDSA GuidelinesDocument47 pagesUpdated IDSA GuidelinesAhmed EzzatNo ratings yet
- Personal Data Form (VBS)Document2 pagesPersonal Data Form (VBS)odhiambopaul139No ratings yet
- ANS PharmacologyDocument24 pagesANS PharmacologySOMOSCONo ratings yet
- Word Formation Easy ExerciseDocument44 pagesWord Formation Easy ExerciseKhoa DangNo ratings yet
- Anthony v. GMD Airline Serv., 1st Cir. (1994)Document22 pagesAnthony v. GMD Airline Serv., 1st Cir. (1994)Scribd Government DocsNo ratings yet
- Kalium KloratDocument6 pagesKalium KloratAnnisa Nur JNo ratings yet
- Science Investigatory Project: Universidad de ManilaDocument7 pagesScience Investigatory Project: Universidad de ManilaCassandra AgustinNo ratings yet
- B I DDocument8 pagesB I DHisabu MohammedNo ratings yet