IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 1 Ver. VIII (Jan. 2015), PP 12-14
www.iosrjournals.org
Deep Infra Patellar Cyst in Osteoarthritis of Knee Joint
Dr.P.Anil Babu1, Dr.G.Vara Prasad2
1
,2
(Assistant Prof. of Orthopaedics, Guntur Medical College / GGH, Guntur ,AP, India)
(Associate Prof. of Orthopaedics, Guntur Medical College / GGH, Guntur ,AP, India)
Abstract: The bursa is a fluid filled sac which spans the area of friction between tendon and skin , and between
tendon and bone. The bursae are usually not seen, not felt on clinical examination unless there is more amount
of fluid collection, inflammatory collection which make them visible and palpable with local signs of
inflammation. Some burse communicate with a joint and contain the fluid collected in the joint space for various
responses coming in from the joint. We report a case of a cystic swelling over the antero inferior aspect of the
knee joint which developed with an insidious course in a patient having an acquired varus deformity of the knee
joint. The cystic swelling was communicating with the knee joint, in which the patient has painful limitation of
movements, joint line tenderness and varus deformity. Deep and superficial infra patellar bursae are prone for
showing a variety inflammatory and traumatic responses in a variety of conditions. In this case the cystic
swelling has occurred due to degenerative changes in the joint with which it is communicating.
Keywords: Deep infra patellar cyst, knee joint, osteoarthritis, varus deformity
I.
Introduction
The friction occurring between two soft tissue planes is prevented by bursae which are present at
various sites. They are present between the skin and tendons, tendons and bones to prevent friction. The bursae
are filled with synovial fluid and some of them communicate with adjacent joint. The most common swelling of
the bursae are due to trauma. They also respond with more amount of synovial fluid production and hypertrophy
of the sac in rheumatoid arthritis, gout, osteoarthritis. The clinical presentation of swelling of the bursa depends
on the underlying cause. The swellings may present with local inflammatory changes, translucency, reducible
swellings with the contents getting emptied into the joint cavity. But there are other soft tissues which present
like bursae with in the vicinity of the joint and should be dealt with a different set of investigations and
treatment plan. Arterio venous malformations, neural sheath tumours, ruptured cyst present with a different set
of clinical features. Infected bursae present with acute features of pain, swelling, temperature. We present a case
of cystic swelling in the antero inferior aspect of the knee joint.
II.
Case Report
A male patient of 65 years of age presented to the OPD with a chief complaint of a swelling in the
antero inferior aspect of the left knee joint. There is a single swelling. It started as a small swelling and grown to
the size of 15 x 8 cm insidiously. His other complaints were painful limitation of movements at the left knee for
the last five years. Patient used to a manual laborer working in agricultural fields with no tasks to kneel down
and work. The symptoms were also associated with a gradually increasing varus deformity at the left knee joint
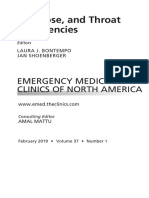
"Fig.1". His vital were with in normal limits.
On examination the swelling is uniform, extending from the knee joint line to proximal third of the leg
on the antero inferior aspect. There were no visible pulsations and scars or sinuses or marks of friction over the
skin. There is no local rise of temperature. Swelling is not attached to the skin. Muscle plane could not be
checked for involvement because of subcutaneous nature. Trans illumination was positive. The knee joint
showed tenderness over joint line and painful limitation of movements restricting the movements to flexion of
70 degrees. There is a varus deformity measuring 20 degrees, with lax medial aspect of the joint. The swelling
could be emptied with movements and valgus stress to the joint which are painful to the patient. The swelling
has become tense in the recent past for which the patient came for treatment. There were no distal neuro
vascular deficits and other joints are normal.
III.
Evaluation
The patient has been taken for evaluation with routine blood investigations, radiographs and ultra
sound examination of the swelling. The blood investigations ruled out the possibilities of infective,
inflammatory and metabolic causes of the swelling. The radiographs of the knee joint "Fig.2" showed changes
of osteoarthritis with grossly decreased medial joint space , multiple osteophytes, loose bodies and varus
deformity. The ultra sound scan revealed a swelling of uniform thickness, because of fluid collection and
extension under the patella under infra patellar fat pad. The patient is counseled about the gross degenerative
DOI: 10.9790/0853-14181214
www.iosrjournals.org
12 | Page
Deep Infra patellar cyst in Osteoarthritis of Knee joint
changes and pain free improvement of movements with joint replacement. The present complaint of tense cystic
swelling has been the prime concern to the patient and opted for treatment for the swelling. Patient was prepared
for the surgery to excise the swelling to give relief from the tense swelling causing painful limitation of
movements.
IV.
Treatment
The swelling has been taken up for excision with a parapatellar incision. The selling has been carefully
isolated from the surrounding soft tissues on the antero inferior aspect "Fig.3". On further dissection posteriorly
it is observed that the swelling is communicating with the knee joint under the patella and below the patellar fat
pad which presented the usual communication of deep infra patellar bursa. . The cyst has been excised with a
sufficient stalk to close the communication with the joint cavity "Fig.4".Perfect haemostasis is achieved and
wound is closed in layers and dressed with compression bandage. The specimen is sent for histopathology
examination which ruled out any inflammatory changes and infections. The patient is allowed to weight bear on
suture removal on tenth post operative day with improvement.
V.
Figures
Fig.1 : Clinical photograph with swelling and deformity
Fig.2 : Radiographs of the Knee joint.
Fig.3 : Swelling in the antero inferior aspect of Knee joint.
DOI: 10.9790/0853-14181214
www.iosrjournals.org
13 | Page
Deep Infra patellar cyst in Osteoarthritis of Knee joint
Fig.4 : Communication with the Knee joint.
VI.
Discussion
An ultra sound examination included in the evaluation of the swelling around a joint helps in arriving
at a possibility when a variety of conditions mimic a cystic selling which may pose a risk in performing
surgery[1]. The possible conditions like arterio venous malformations, nueral sheath tumors, synovial
proliferations can be easily ruled out with reliability. In case with acute presentations like a ruptured cyst or
deep vein thrombosis a clear protocol should be followed avoid morbidity associated with acute cases [2].it is
important to include ultra sound examination to evaluate the swelling to know the extent and nature of the
covering and content of the swelling[3].inflammatory and infective conditions also present like cystic swellings
around the knee joint , making it to include them in the differential diagnosis[4]. Even when there are no signs
of inflammation or infections swellings can occur in the peri articular soft tissues. The ultra sound scan can rule
out the extension into the joint or an entirely pathological conditions out side the joint[5]. Knee bursitis is a
common condition in manual laborers working with lot of friction at the knee surfaces and may not be
associated with joint pathology[6]. Acute exacerbations of a chronic condition may occur due to trivial trauma
triggering synovial effusion and present with bursitis as cystic swelling[7].Cases with non traumatic conditions
presenting with acute features need to evaluated for infections and gout which present with local rise of
temperature, fever and swelling[8]. Paediatric cases may present with infra patellar bursitis in juvenile
rheumatoid arthritis with cystic swellings involving the infra patellar bursa which needs to be consider4ed for
knee joint pain in paediatric age group[9].
VII.
Conclusion
A bursa communicating with the joint responds to the various pathologies occurring in the joint
including the inflammations, infections, metabolic disorders, degenerative disorders etc,. In the case we reported
the deep infra patellar bursa with its communication to the knee joint has accommodated the increased synovial
fluid collected because of degenerative osteoarthritis of the knee joint. The other possible conditions affecting
the peri articular soft tissues are ruled out in the evaluation by subjecting the patient to the radiographs and ultra
sound scans. The necessary evaluation has ruled out both acutely occurring and chronic conditions with acute
exacerbations.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
Bevers K, Zweers MC, van den Ende CH, Martens HA, Mahler E, Bijlsma JW, Wakefield RJ, van den Hoogen FH, den Broeder
AA. Ultrasonographic analysis in knee osteoarthritis: evaluation of inter-observer reliability.Clin Exp Rheumatol. 2012 SepOct;30(5):673-8. Epub 2012 Oct 17.
Hoffmann R, Brunner U.Imitation of acute, deep venous thrombosis of the lower leg by a ruptured Baker's cyst.
Vasa. 1989;18(1):74-7.
Bevers K, Bijlsma JW, Vriezekolk JE, van den Ende CH, den Broeder AA. Ultrasonographic features in symptomatic osteoarthritis
of the knee and relation with pain. Rheumatology (Oxford). 2014 Sep;53(9):1625-9. doi: 10.1093/rheumatology/keu030. Epub 2014
Apr
Leth S, Jensen-Fangel S. Infrapatellar bursitis with Mycobacterium malmoense related to immune reconstitution inflammatory
syndrome in an HIV-positive patient.BMJ Case Rep. 2012 Nov 27;2012. pii: bcr2012007459. doi: 10.1136/bcr-2012-007459.
Iagnocco A1, Vavala C, Scirocco C, Rutigliano IM, Gattamelata A, Valesini G. Unilateral painful, swollen and erythematosus knee.
Case report.Med Ultrason. 2012 Sep;14(3):251-3.
Le Manac'h AP1, Ha C, Descatha A, Imbernon E, Roquelaure Y. Prevalence of knee bursitis in the workforce. Occup Med
(Lond). 2012 Dec;62(8):658-60. doi: 10.1093/occmed/kqs113. Epub 2012 Jul 9.
Een S, Akarrmak U, Aydn FY, Unalan H. Clinical evaluation during the acute exacerbation of knee osteoarthritis: the impact of
diagnostic ultrasonography. Rheumatol Int. 2013 Mar;33(3):711-7. doi: 10.1007/s00296-012-2441-1. Epub 2012 May 5.
Reed MJ1, Carachi A. Eur J Emerg Med. Management of the nontraumatic hot swollen joint.2012 Apr;19(2):103-7. doi:
10.1097/MEJ.0b013e328348d8f8.
Alqanatish JT1, Petty RE, Houghton KM, Guzman J, Tucker LB, Cabral DA, Cairns RA. Clin Rheumatol. Infrapatellar bursitis in
children with juvenile idiopathic arthritis: a case series.2011 Feb;30(2):263-7. doi: 10.1007/s10067-010-1620-2. Epub 2010 Nov 19.
DOI: 10.9790/0853-14181214
www.iosrjournals.org
14 | Page
You might also like
- Solution For Introduction To Environmental Engineering 5th Edition by Mackenzie L DavisDocument41 pagesSolution For Introduction To Environmental Engineering 5th Edition by Mackenzie L DavisVISHAL VERMA86% (7)
- Case Study 2Document7 pagesCase Study 2desdav100% (1)
- Pharmacology Usmle Step 1Document5 pagesPharmacology Usmle Step 1raj_1041100% (16)
- Bursitis - An Overview of Clinical Manifestations, Diagnosis, and Management - UpToDateDocument16 pagesBursitis - An Overview of Clinical Manifestations, Diagnosis, and Management - UpToDateDannyGutierrezNo ratings yet
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemFrom EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNo ratings yet
- Overview of Geriatric Rehabilitation - Program Components and Settings For RehabilitationDocument37 pagesOverview of Geriatric Rehabilitation - Program Components and Settings For RehabilitationWasemBhat0% (1)
- Introduction:-: Case Report - Pigmented Villonodular Synovitis Great ToeDocument6 pagesIntroduction:-: Case Report - Pigmented Villonodular Synovitis Great ToeJeffrey GillespieNo ratings yet
- Baker 11Document3 pagesBaker 11Ramadhan Maulana RizalNo ratings yet
- Septic Arthritis UpgradedDocument47 pagesSeptic Arthritis UpgradedVishva Randhara AllesNo ratings yet
- Ledderhose Disease: Pathophysiology Diagnosis and ManagementDocument3 pagesLedderhose Disease: Pathophysiology Diagnosis and ManagementLeandro PolancoNo ratings yet
- Knee Tuberculosis: Dr. Riama Noveria SianturiDocument17 pagesKnee Tuberculosis: Dr. Riama Noveria SianturiSyane KristinaNo ratings yet
- Knee PainDocument34 pagesKnee Painmanoj ramlal kandoi100% (1)
- Synovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsDocument18 pagesSynovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsEka JuliantaraNo ratings yet
- Hip and Pelvic Injections PDFDocument12 pagesHip and Pelvic Injections PDFVijay Kumar100% (1)
- Joint DiseaseDocument5 pagesJoint DiseaseKimrose TampusNo ratings yet
- Synovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: AuthorsDocument18 pagesSynovial Knee Disease: MRI Differential Diagnosis: Poster No.: Congress: Type: Authorsjuny138No ratings yet
- PIIS2212628721001900Document6 pagesPIIS2212628721001900ANDRES DURANNo ratings yet
- Bone Infections: OsteomyelitisDocument6 pagesBone Infections: OsteomyelitisMarius Clifford BilledoNo ratings yet
- ArtosDocument22 pagesArtosRia Rahmadiyani IINo ratings yet
- Achilles Tendon Injuries: Signs and SymptomsDocument23 pagesAchilles Tendon Injuries: Signs and SymptomsahmadNo ratings yet
- General OrthopaedicsDocument50 pagesGeneral Orthopaedicsضبيان فرحانNo ratings yet
- Tuberculosis Ofintramuscular Hematoma Post Acl Reconstruction: A Case ReportDocument3 pagesTuberculosis Ofintramuscular Hematoma Post Acl Reconstruction: A Case ReportIJAR JOURNALNo ratings yet
- Septicarthritis 110426090729 Phpapp02Document21 pagesSepticarthritis 110426090729 Phpapp02Diana MayasariNo ratings yet
- OsteomyelitisDocument8 pagesOsteomyelitisMargarette Lopez0% (1)
- Terapia OcupacionalDocument7 pagesTerapia OcupacionalMiguelangel AlemánNo ratings yet
- Laporan Pemicu 4 DK 9Document53 pagesLaporan Pemicu 4 DK 9Ade Cahyo IslamiNo ratings yet
- Clinical Anatomy of The Knee PDFDocument7 pagesClinical Anatomy of The Knee PDFJuan Victor Briceno OrtizNo ratings yet
- Osteomyelitis Report Orthopedic NursingDocument15 pagesOsteomyelitis Report Orthopedic NursingSienaNo ratings yet
- Septic Arthritis NAC OSCEDocument11 pagesSeptic Arthritis NAC OSCEngoc nhan nguyen thiNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Osteomyelitis: Oleh Ira Suarilah Dept - Kep.Medikal-Bedah Psik-Fk UnairDocument13 pagesAsuhan Keperawatan Pada Klien Dengan Osteomyelitis: Oleh Ira Suarilah Dept - Kep.Medikal-Bedah Psik-Fk UnairNikmaNo ratings yet
- Clinicas de Endocrino. Pie Diabetico - Dic 2013Document15 pagesClinicas de Endocrino. Pie Diabetico - Dic 2013Betzabeth RodriguezNo ratings yet
- Kuliah Kelainan PeriartikulerDocument20 pagesKuliah Kelainan PeriartikulerRoby KieranNo ratings yet
- Etiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisDocument42 pagesEtiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisNoe-pal DynmNo ratings yet
- MKSAP 15 RheumatologyDocument177 pagesMKSAP 15 Rheumatologyfelipepatagon100% (2)
- Notas - Artículo BursitisDocument4 pagesNotas - Artículo BursitisDaniel_Trujillo_DNo ratings yet
- Multidisciplinary Approach To Scheduling Surgery For Diabetic Foot: A Case ReportDocument6 pagesMultidisciplinary Approach To Scheduling Surgery For Diabetic Foot: A Case ReportLuciano JuniorNo ratings yet
- Askep OsteomielitisDocument13 pagesAskep Osteomielitisuciha_herhyNo ratings yet
- Osteomyelitis of Maxilla - A Rare Presentation CasDocument7 pagesOsteomyelitis of Maxilla - A Rare Presentation Casshehla khanNo ratings yet
- Radiographic Features: Pes Anserinus BursitisDocument4 pagesRadiographic Features: Pes Anserinus BursitisPutri OktoviaNo ratings yet
- Amit Murli Patel. Physical Therapy Management of Tuberculous Arthritis of The Elbow SRJI Vol - 2, Issue - 1, Year - 2013Document10 pagesAmit Murli Patel. Physical Therapy Management of Tuberculous Arthritis of The Elbow SRJI Vol - 2, Issue - 1, Year - 2013Dr. Krishna N. SharmaNo ratings yet
- Case Report TB of The KneeDocument4 pagesCase Report TB of The KneeBima Saphien AlpanaceaNo ratings yet
- Sport Traumatology-III Knee Complex-9Document28 pagesSport Traumatology-III Knee Complex-9kamran aliNo ratings yet
- Pathological Unstable Dislocation of Shoulder S 2024 International Journal oDocument5 pagesPathological Unstable Dislocation of Shoulder S 2024 International Journal oRonald QuezadaNo ratings yet
- Rheumatoid ArthritisDocument18 pagesRheumatoid Arthritismanoj ramlal kandoiNo ratings yet
- Hasenstein2019 PDFDocument16 pagesHasenstein2019 PDFArthur TeixeiraNo ratings yet
- Presentation 1Document120 pagesPresentation 1Khurram ChauhanNo ratings yet
- I. Definition of Disease: Start in The Teens and 20sDocument4 pagesI. Definition of Disease: Start in The Teens and 20sAriaNo ratings yet
- BPJ65 Ingrown ToenailsDocument8 pagesBPJ65 Ingrown ToenailsDrHariom Keshari100% (1)
- BURSITISDocument18 pagesBURSITISmonapurwitasariNo ratings yet
- Pe of The Joint - GoutDocument50 pagesPe of The Joint - GoutCharisse Ann GasatayaNo ratings yet
- Clinical Review: Management and Referral For Trigger Finger/thumbDocument4 pagesClinical Review: Management and Referral For Trigger Finger/thumbRipka_uliNo ratings yet
- Ki 1.1 Rotator Cuff Any 2 ASDocument29 pagesKi 1.1 Rotator Cuff Any 2 ASAgus TianyNo ratings yet
- OSTEOMYELITISDocument48 pagesOSTEOMYELITISTom BetsonNo ratings yet
- Osteoarthritis of The Hip: Clinical PracticeDocument9 pagesOsteoarthritis of The Hip: Clinical PracticeMarina Tomasenco - DaniciNo ratings yet
- Bovine Digit Surgical TechniqueDocument16 pagesBovine Digit Surgical TechniqueWendyNo ratings yet
- Ishida 2018Document3 pagesIshida 2018mascoNo ratings yet
- MOR 2152 SiapDocument11 pagesMOR 2152 SiapMohamad RaisNo ratings yet
- Compound Plamar GanglionDocument4 pagesCompound Plamar Ganglionchinmayghaisas100% (2)
- Bursitis TrocanterDocument18 pagesBursitis TrocanterAngie Paola RodriguezNo ratings yet
- Hypertrophic Osteoarthropathy: An Unusual Cause of Knee Pain and Recurrent EffusionDocument3 pagesHypertrophic Osteoarthropathy: An Unusual Cause of Knee Pain and Recurrent EffusionWami FadelNo ratings yet
- A Current Concept Review: Tuberculosis of HipDocument10 pagesA Current Concept Review: Tuberculosis of HipAnonymous gvVAzlNo ratings yet
- Comprehensive Insights into Achilles Tendinitis: Unveiling Pathways to Recovery and PreventionFrom EverandComprehensive Insights into Achilles Tendinitis: Unveiling Pathways to Recovery and PreventionNo ratings yet
- Stop Knee Bursitis Pain: The Ultimate Knee Bursitis GuideFrom EverandStop Knee Bursitis Pain: The Ultimate Knee Bursitis GuideNo ratings yet
- Necessary Evils of Private Tuition: A Case StudyDocument6 pagesNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)No ratings yet
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocument10 pagesEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocument5 pagesYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocument2 pagesComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)No ratings yet
- Factors Affecting Success of Construction ProjectDocument10 pagesFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameDocument9 pagesDesign and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactDocument11 pagesDesign and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactInternational Organization of Scientific Research (IOSR)No ratings yet
- Fatigue Analysis of A Piston Ring by Using Finite Element AnalysisDocument4 pagesFatigue Analysis of A Piston Ring by Using Finite Element AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Crigler-Najjar Syndrome - UpToDateDocument31 pagesCrigler-Najjar Syndrome - UpToDateMihaela Alexandra RepeziNo ratings yet
- 1 s2.0 S0197455617300424 MainDocument9 pages1 s2.0 S0197455617300424 MainJulia LinzenboldNo ratings yet
- The Blood Sugar Solution 2012Document306 pagesThe Blood Sugar Solution 2012Waqar Ahmed Awan100% (7)
- Your Physical Constitution PrakrutiDocument2 pagesYour Physical Constitution PrakrutiDhanwantari JhaNo ratings yet
- Fitness Manual IFADocument128 pagesFitness Manual IFAAlejandro BalcazarNo ratings yet
- Processing of MilkDocument7 pagesProcessing of MilkMari Liz0% (1)
- 5 Integrated AquacultureDocument14 pages5 Integrated AquacultureGezim BytyqiNo ratings yet
- How To Become A College Drug KingpinDocument17 pagesHow To Become A College Drug KingpinConn8895100% (1)
- Ebp Head Up 30Document9 pagesEbp Head Up 30La fazaNo ratings yet
- Internet AddictionDocument13 pagesInternet AddictionGerardo DamianNo ratings yet
- Current Opinion Hematol RR AML 2019Document8 pagesCurrent Opinion Hematol RR AML 2019Ernesto PiconNo ratings yet
- Anatomi Dan Fisiologi: The Cardiovascular SystemDocument8 pagesAnatomi Dan Fisiologi: The Cardiovascular SystemAzrin MohayaddinNo ratings yet
- Introduction To Vet MedDocument26 pagesIntroduction To Vet MedAhmed Raza33% (3)
- Emergencias Orl PDFDocument150 pagesEmergencias Orl PDFFabian Camelo OtorrinoNo ratings yet
- Chapter 59 Nursing PharmacyDocument7 pagesChapter 59 Nursing PharmacyMisty WiseNo ratings yet
- Ganga Sadbhavana Yatra PDFDocument95 pagesGanga Sadbhavana Yatra PDFsri_vas4uNo ratings yet
- Thailand BABE GuidelineDocument27 pagesThailand BABE GuidelineDianeNo ratings yet
- Medical Leave of Absence (Mloa) Treatment Provider Report: SECTION I: To Be Completed by The StudentDocument4 pagesMedical Leave of Absence (Mloa) Treatment Provider Report: SECTION I: To Be Completed by The StudentShubho DasNo ratings yet
- Prilosec (Omeprazole) MoreDocument3 pagesPrilosec (Omeprazole) MoreLuis Arturo Andrade CoronadoNo ratings yet
- News&Notes 17 March 2012Document21 pagesNews&Notes 17 March 2012Aravind KaliamoorthyNo ratings yet
- Anti-Malerials MaterialsDocument13 pagesAnti-Malerials Materialsraj royelNo ratings yet
- Assessment of Waste Water Plant ReportDocument18 pagesAssessment of Waste Water Plant ReportRichard Dablah0% (1)
- Teaching Plan: General Santos Doctors' Medical School Foundation IncDocument12 pagesTeaching Plan: General Santos Doctors' Medical School Foundation Incjay kusainNo ratings yet
- Complications in Dentoalveolar Surgery PDFDocument37 pagesComplications in Dentoalveolar Surgery PDFmirfanulhaqNo ratings yet
- Geriatric NursingDocument6 pagesGeriatric NursingKarl JoseNo ratings yet
- Checklist 200806 Medicolegal Checklist PhysiciansDocument4 pagesChecklist 200806 Medicolegal Checklist PhysiciansIkhsan El-SonadorNo ratings yet
- ConclusionDocument2 pagesConclusionrichardiaNo ratings yet