
Re Plantation
Re Plantation
You might also like
- Final Exam NRNP-6531 Advanced PracticeDocument21 pagesFinal Exam NRNP-6531 Advanced PracticeGeorge Ekai100% (4)
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- Holiday Testing ProcedureDocument1 pageHoliday Testing ProcedureSyed Zakiuddin100% (2)
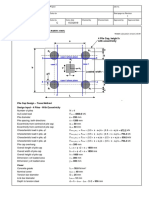
- 4 Piles Cap With Eccentricity ExampleDocument3 pages4 Piles Cap With Eccentricity ExampleSousei No Keroberos100% (1)
- Interface Converter Set: Special FeaturesDocument2 pagesInterface Converter Set: Special FeaturesLuis Fernando Peres GutierrezNo ratings yet
- Delayed Formation of Multiple Supernumerary TeethDocument6 pagesDelayed Formation of Multiple Supernumerary TeethsauriuaNo ratings yet
- Locating Broken NeedlesDocument3 pagesLocating Broken NeedlesmedicmayaNo ratings yet
- Intentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasDocument8 pagesIntentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasFlorin IonescuNo ratings yet
- Reimplantation of Avulsed Teeth After Dry Storage For One WeekDocument5 pagesReimplantation of Avulsed Teeth After Dry Storage For One WeekHesti RahayuNo ratings yet
- Sciencedirect: Specially Designed Tooth Supported Mandibular Overdenture With Enhanced RetentionDocument4 pagesSciencedirect: Specially Designed Tooth Supported Mandibular Overdenture With Enhanced Retentionannisa anindyaNo ratings yet
- Surgical and Endodontic Management of Large Cystic Lesion: AbstractDocument5 pagesSurgical and Endodontic Management of Large Cystic Lesion: AbstractanamaghfirohNo ratings yet
- A New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueDocument4 pagesA New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueKarin Noga VerhagenNo ratings yet
- Recovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystDocument5 pagesRecovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystmeryemeNo ratings yet
- Histologic Analysis of Pulpal Revascularization of Autotransplanted Immature Teeth After Removal of The Original Pulp TissueDocument7 pagesHistologic Analysis of Pulpal Revascularization of Autotransplanted Immature Teeth After Removal of The Original Pulp TissuePatricia BurbanoNo ratings yet
- Maxillary Lateral Incisor With Four Root CanalsDocument5 pagesMaxillary Lateral Incisor With Four Root Canalsdentace1No ratings yet
- Restoration Made Possible With Forced OrthodonticDocument3 pagesRestoration Made Possible With Forced OrthodonticLaura RuZeNo ratings yet
- ASE Eport: "Second Chance To Save Your Tooth"-A Case ReportDocument6 pagesASE Eport: "Second Chance To Save Your Tooth"-A Case ReportAnonymous UT3s7CNo ratings yet
- Immediate Natural Tooth Pontic - A Case ReportDocument3 pagesImmediate Natural Tooth Pontic - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Papilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportDocument8 pagesPapilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportsnkidNo ratings yet
- Eruptive AnomaliesDocument65 pagesEruptive AnomaliesBenet BabuNo ratings yet
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 pagesFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Endo024en (065 069) OarDocument5 pagesEndo024en (065 069) OarNadya PurwantyNo ratings yet
- Orthodontic Extrusion of Premolar Teeth - An Improved TechniqueDocument6 pagesOrthodontic Extrusion of Premolar Teeth - An Improved TechniquejorgeNo ratings yet
- The Use of PRF in Covering Exposed ImplantDocument6 pagesThe Use of PRF in Covering Exposed ImplantMohammad AkheelNo ratings yet
- Implicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoDocument9 pagesImplicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoAlfredo NovoaNo ratings yet
- A Suggested Butterfly Design For Mandibular Tori in Partially Edentulous Patient: Clinical CaseDocument18 pagesA Suggested Butterfly Design For Mandibular Tori in Partially Edentulous Patient: Clinical CasejenNo ratings yet
- Apexification 07.03.22Document10 pagesApexification 07.03.22Shreya KediaNo ratings yet
- Exostosis MandibularDocument6 pagesExostosis MandibularCOne Gomez LinarteNo ratings yet
- Conventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementDocument2 pagesConventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementErwin SutonoNo ratings yet
- Dramit007, Journal Manager, 13Document3 pagesDramit007, Journal Manager, 13KAREN VIVIANA ALVARADO HERNANDEZNo ratings yet
- Submerged Root TechniqueDocument5 pagesSubmerged Root TechniqueFrederick Alexander TrisnaNo ratings yet
- Gupta2011 PDFDocument5 pagesGupta2011 PDFAbdul Rahman AlmishhdanyNo ratings yet
- Rehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesDocument10 pagesRehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesIJAR JOURNALNo ratings yet
- Endodontic Treatment of Dens InvaginatusDocument7 pagesEndodontic Treatment of Dens InvaginatusParidhi GargNo ratings yet
- Ricucci 2014Document7 pagesRicucci 2014leiliromualdoNo ratings yet
- Periodontal Plastic SurgeryDocument5 pagesPeriodontal Plastic Surgeryudhai170819No ratings yet
- Telescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaDocument5 pagesTelescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaRani PutriNo ratings yet
- Nasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIDocument6 pagesNasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIHashem Motahir Ali Al-ShamiriNo ratings yet
- Oke 4Document3 pagesOke 4Maika RatriNo ratings yet
- Tooth-Support Over Dentures: An Approach To Preventive ProsthodonticsDocument5 pagesTooth-Support Over Dentures: An Approach To Preventive ProsthodonticsAdvanced Research PublicationsNo ratings yet
- Revascularization of Immature Permanent Incisors After Severe Extrusive Luxation InjuryDocument10 pagesRevascularization of Immature Permanent Incisors After Severe Extrusive Luxation InjuryEduardo CarrielNo ratings yet
- Labial Access For Lower TeethDocument3 pagesLabial Access For Lower TeethHarish ChowdaryNo ratings yet
- Loss of Anterior TissuesDocument5 pagesLoss of Anterior Tissuesjinny1_0No ratings yet
- CBCTDocument7 pagesCBCTPrevita NindaNo ratings yet
- 2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepDocument6 pages2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepTudor LupesNo ratings yet
- The Swing-Lock Denture - Its Use in Conventional Removable Partial Denture ProsthodonticsDocument3 pagesThe Swing-Lock Denture - Its Use in Conventional Removable Partial Denture ProsthodonticsElena Besliu100% (1)
- The Bio-Col TechniqueDocument9 pagesThe Bio-Col TechniquewnelsenNo ratings yet
- Bioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionDocument0 pagesBioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionTrinhTaNo ratings yet
- Patient Age Is No Contraindication To Endodontic TreatmentDocument3 pagesPatient Age Is No Contraindication To Endodontic TreatmentMelisa Agustine LeeNo ratings yet
- Clinical Response To A Vacant Post Space: Case ReportDocument7 pagesClinical Response To A Vacant Post Space: Case ReportVICTOR FERNANDO LAMAS LARANo ratings yet
- Severe Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportDocument5 pagesSevere Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportanjozzNo ratings yet
- Prosthodontic Management of Severely ResorbedDocument2 pagesProsthodontic Management of Severely ResorbedAamir BugtiNo ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- Restoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationDocument5 pagesRestoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationIntelligentiaNo ratings yet
- Hemisection of A Severely Decayed Mandibular Molar: A Case ReportDocument4 pagesHemisection of A Severely Decayed Mandibular Molar: A Case Reportkartika tiaraNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- 563421.v1 PerioDocument15 pages563421.v1 Perioikeuchi_ogawaNo ratings yet
- External Cervical Resorption JC FinalDocument46 pagesExternal Cervical Resorption JC FinalKomal JadhavNo ratings yet
- Think Before You Extract - A Case of Tooth AutotransplantationDocument5 pagesThink Before You Extract - A Case of Tooth AutotransplantationBoris ChapelletNo ratings yet
- Surgical Extraction of Mandibular Third Molar in Pterygomandibular Space: A Case ReportDocument4 pagesSurgical Extraction of Mandibular Third Molar in Pterygomandibular Space: A Case ReportadriandjoNo ratings yet
- Forced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case ReportDocument4 pagesForced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case Reportikeuchi_ogawaNo ratings yet
- Skeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical StudyDocument13 pagesSkeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical Studyaleja.b7815No ratings yet
- The Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsFrom EverandThe Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsNo ratings yet
- Published 1593 Published 1612 Published 1913 Published 1919 Published 1978Document4 pagesPublished 1593 Published 1612 Published 1913 Published 1919 Published 1978leeperlhan2000No ratings yet
- Journal Pone 0132958 s001Document11 pagesJournal Pone 0132958 s001leeperlhan2000No ratings yet
- Accelerated Repetitive Transcranial Magnetic Stimulation in The Treatment of DepressionDocument8 pagesAccelerated Repetitive Transcranial Magnetic Stimulation in The Treatment of Depressionleeperlhan2000No ratings yet
- MMRDocument6 pagesMMRleeperlhan2000No ratings yet
- Voxel-Based Morphometry With Unified SegmentationDocument65 pagesVoxel-Based Morphometry With Unified Segmentationleeperlhan2000No ratings yet
- Wise MindDocument1 pageWise Mindleeperlhan2000No ratings yet
- The Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's SyndromeDocument10 pagesThe Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's Syndromeleeperlhan2000No ratings yet
- Substance Abuse Among Young PeopleDocument57 pagesSubstance Abuse Among Young Peopleleeperlhan2000No ratings yet
- Assessing Quality of Life For Adolescents in Taiwan: Regular ArticleDocument8 pagesAssessing Quality of Life For Adolescents in Taiwan: Regular Articleleeperlhan2000No ratings yet
- Eagle's Syndrome in An 11-Year-Old PatientDocument4 pagesEagle's Syndrome in An 11-Year-Old Patientleeperlhan2000No ratings yet
- Treatment of Drug AddictionDocument34 pagesTreatment of Drug Addictionleeperlhan2000No ratings yet
- Methadone Treatment in The U.S.ADocument43 pagesMethadone Treatment in The U.S.Aleeperlhan2000No ratings yet
- Brief Psychosocial Interventions For Substance AbuseDocument41 pagesBrief Psychosocial Interventions For Substance Abuseleeperlhan2000No ratings yet
- Analysis of Royal Vale Heath's "Take A Number From 1 To 30"Document2 pagesAnalysis of Royal Vale Heath's "Take A Number From 1 To 30"leeperlhan2000No ratings yet
- 13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, RegardlessDocument5 pages13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, Regardlessleeperlhan2000No ratings yet
- Tadeu Magalhaes - 250 Gags & Jokes For Comedy MagiciansDocument19 pagesTadeu Magalhaes - 250 Gags & Jokes For Comedy Magiciansleeperlhan2000100% (4)
- Suicide Risk Management ProtocolDocument3 pagesSuicide Risk Management Protocolleeperlhan2000No ratings yet
- A New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of IllnessDocument19 pagesA New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of Illnessleeperlhan2000No ratings yet
- Shared Decision Making。: The Massachusetts General Hospital/Mclean Hospital: Residency Handbook Of PsychiatryDocument1 pageShared Decision Making。: The Massachusetts General Hospital/Mclean Hospital: Residency Handbook Of Psychiatryleeperlhan2000No ratings yet
- Chapter 30 LamotrigineDocument7 pagesChapter 30 Lamotrigineleeperlhan2000No ratings yet
- Chapter 14 BuspironeDocument10 pagesChapter 14 Buspironeleeperlhan2000No ratings yet
- Basic Offshore Safety Induction and Emergency Training: CtsiDocument72 pagesBasic Offshore Safety Induction and Emergency Training: Ctsiangel coazoNo ratings yet
- Between Japan & Germany Related To Dentistry 1Document9 pagesBetween Japan & Germany Related To Dentistry 1Dr Riktesh SrivastavaNo ratings yet
- Techinques Coloredpencils Basics2Document7 pagesTechinques Coloredpencils Basics2Roland CepedaNo ratings yet
- Microstrip Patch Antenna and Its ApplicationDocument20 pagesMicrostrip Patch Antenna and Its ApplicationBrhane DadsoNo ratings yet
- Magne ProvisionalsDocument10 pagesMagne Provisionalsdrdanielsan100% (1)
- People vs. Siao, G.R. No. 126021 March 3, 2000Document3 pagesPeople vs. Siao, G.R. No. 126021 March 3, 2000Ria Evita RevitaNo ratings yet
- AREVA T&D Product RangeDocument10 pagesAREVA T&D Product RangeEduardo SolanoNo ratings yet
- Violence Against WomenDocument81 pagesViolence Against WomenOxfamNo ratings yet
- Hidden Valley Deed RestrictionsDocument2 pagesHidden Valley Deed Restrictionsapi-4678260460% (1)
- Sanitation, Plumbing Design & Installation: G. Dry and Wet StandpipeDocument10 pagesSanitation, Plumbing Design & Installation: G. Dry and Wet StandpipeDwight Swayne AlegrosNo ratings yet
- Experiment 3 (Sublimation and Melting Point Determination)Document13 pagesExperiment 3 (Sublimation and Melting Point Determination)Cheng BauzonNo ratings yet
- Synopsis: Rajiv Gandhi University of Health Sciences Karnataka State, BangaloreDocument17 pagesSynopsis: Rajiv Gandhi University of Health Sciences Karnataka State, BangaloreSANANo ratings yet
- Disaster Nursing NotesDocument4 pagesDisaster Nursing NotesChannelG100% (1)
- Academy of Economic Studies of Moldova: Performed by Artur CatanoiDocument3 pagesAcademy of Economic Studies of Moldova: Performed by Artur CatanoiArtur CatanoiNo ratings yet
- Bio-Botany Vol-2 - EM PDFDocument216 pagesBio-Botany Vol-2 - EM PDFsudha1987No ratings yet
- KonectDocument2 pagesKonectHellen DuNo ratings yet
- H250 H250 H250 H250: Variable Area FlowmeterDocument88 pagesH250 H250 H250 H250: Variable Area Flowmetercedar1015No ratings yet
- Kirlian Photograpy and Energy TappingDocument7 pagesKirlian Photograpy and Energy Tappingnblack3335140No ratings yet
- Codex Standard For Whey Cheeses: CODEX STAN A-7-1971, Rev. 2-2006Document3 pagesCodex Standard For Whey Cheeses: CODEX STAN A-7-1971, Rev. 2-2006hoda hassanNo ratings yet
- Act Critical Skills List Aug 20Document3 pagesAct Critical Skills List Aug 20RobertNo ratings yet
- 8 Sacred Secrets - Keys To Unlock Your Womb PDFDocument6 pages8 Sacred Secrets - Keys To Unlock Your Womb PDFDaniela IlieNo ratings yet
- Criminal Justice Reform ActDocument5 pagesCriminal Justice Reform ActDNAinfoNewYork100% (1)
- AAP Guia Practica Liquidos IVDocument12 pagesAAP Guia Practica Liquidos IVMiroslaba Avila DiazNo ratings yet
- Overview of Citric Acid Production From Aspergillus NigerDocument14 pagesOverview of Citric Acid Production From Aspergillus NigerPetru AstefanoaieNo ratings yet
- Exam - DRRRDocument3 pagesExam - DRRRmycah hagadNo ratings yet
- Fire Alarm Control (IFC 640)Document84 pagesFire Alarm Control (IFC 640)thephuocNo ratings yet













































































































Download as pdf or txt
You might also like
- Final Exam NRNP-6531 Advanced PracticeDocument21 pagesFinal Exam NRNP-6531 Advanced PracticeGeorge Ekai100% (4)
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- Holiday Testing ProcedureDocument1 pageHoliday Testing ProcedureSyed Zakiuddin100% (2)
- 4 Piles Cap With Eccentricity ExampleDocument3 pages4 Piles Cap With Eccentricity ExampleSousei No Keroberos100% (1)
- Interface Converter Set: Special FeaturesDocument2 pagesInterface Converter Set: Special FeaturesLuis Fernando Peres GutierrezNo ratings yet
- Delayed Formation of Multiple Supernumerary TeethDocument6 pagesDelayed Formation of Multiple Supernumerary TeethsauriuaNo ratings yet
- Locating Broken NeedlesDocument3 pagesLocating Broken NeedlesmedicmayaNo ratings yet
- Intentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasDocument8 pagesIntentional Replantation - A Last Resort Treatment or A Conventional Treatment Procedure Nine CasFlorin IonescuNo ratings yet
- Reimplantation of Avulsed Teeth After Dry Storage For One WeekDocument5 pagesReimplantation of Avulsed Teeth After Dry Storage For One WeekHesti RahayuNo ratings yet
- Sciencedirect: Specially Designed Tooth Supported Mandibular Overdenture With Enhanced RetentionDocument4 pagesSciencedirect: Specially Designed Tooth Supported Mandibular Overdenture With Enhanced Retentionannisa anindyaNo ratings yet
- Surgical and Endodontic Management of Large Cystic Lesion: AbstractDocument5 pagesSurgical and Endodontic Management of Large Cystic Lesion: AbstractanamaghfirohNo ratings yet
- A New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueDocument4 pagesA New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueKarin Noga VerhagenNo ratings yet
- Recovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystDocument5 pagesRecovery of Pulp Sensibility After The Surgical Management of A Large Radicular CystmeryemeNo ratings yet
- Histologic Analysis of Pulpal Revascularization of Autotransplanted Immature Teeth After Removal of The Original Pulp TissueDocument7 pagesHistologic Analysis of Pulpal Revascularization of Autotransplanted Immature Teeth After Removal of The Original Pulp TissuePatricia BurbanoNo ratings yet
- Maxillary Lateral Incisor With Four Root CanalsDocument5 pagesMaxillary Lateral Incisor With Four Root Canalsdentace1No ratings yet
- Restoration Made Possible With Forced OrthodonticDocument3 pagesRestoration Made Possible With Forced OrthodonticLaura RuZeNo ratings yet
- ASE Eport: "Second Chance To Save Your Tooth"-A Case ReportDocument6 pagesASE Eport: "Second Chance To Save Your Tooth"-A Case ReportAnonymous UT3s7CNo ratings yet
- Immediate Natural Tooth Pontic - A Case ReportDocument3 pagesImmediate Natural Tooth Pontic - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Papilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportDocument8 pagesPapilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportsnkidNo ratings yet
- Eruptive AnomaliesDocument65 pagesEruptive AnomaliesBenet BabuNo ratings yet
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 pagesFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Endo024en (065 069) OarDocument5 pagesEndo024en (065 069) OarNadya PurwantyNo ratings yet
- Orthodontic Extrusion of Premolar Teeth - An Improved TechniqueDocument6 pagesOrthodontic Extrusion of Premolar Teeth - An Improved TechniquejorgeNo ratings yet
- The Use of PRF in Covering Exposed ImplantDocument6 pagesThe Use of PRF in Covering Exposed ImplantMohammad AkheelNo ratings yet
- Implicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoDocument9 pagesImplicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoAlfredo NovoaNo ratings yet
- A Suggested Butterfly Design For Mandibular Tori in Partially Edentulous Patient: Clinical CaseDocument18 pagesA Suggested Butterfly Design For Mandibular Tori in Partially Edentulous Patient: Clinical CasejenNo ratings yet
- Apexification 07.03.22Document10 pagesApexification 07.03.22Shreya KediaNo ratings yet
- Exostosis MandibularDocument6 pagesExostosis MandibularCOne Gomez LinarteNo ratings yet
- Conventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementDocument2 pagesConventional Implant With Orthodontic Treatment For Anterior Missing Tooth ManagementErwin SutonoNo ratings yet
- Dramit007, Journal Manager, 13Document3 pagesDramit007, Journal Manager, 13KAREN VIVIANA ALVARADO HERNANDEZNo ratings yet
- Submerged Root TechniqueDocument5 pagesSubmerged Root TechniqueFrederick Alexander TrisnaNo ratings yet
- Gupta2011 PDFDocument5 pagesGupta2011 PDFAbdul Rahman AlmishhdanyNo ratings yet
- Rehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesDocument10 pagesRehabilitation of Maxillary Defects in Partial and Complete Edentulous Arches With Definitive Obturators-A Case SeriesIJAR JOURNALNo ratings yet
- Endodontic Treatment of Dens InvaginatusDocument7 pagesEndodontic Treatment of Dens InvaginatusParidhi GargNo ratings yet
- Ricucci 2014Document7 pagesRicucci 2014leiliromualdoNo ratings yet
- Periodontal Plastic SurgeryDocument5 pagesPeriodontal Plastic Surgeryudhai170819No ratings yet
- Telescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaDocument5 pagesTelescopic Overdenture: A Case Report: C. S. Shruthi, R. Poojya, Swati Ram, AnupamaRani PutriNo ratings yet
- Nasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIDocument6 pagesNasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIHashem Motahir Ali Al-ShamiriNo ratings yet
- Oke 4Document3 pagesOke 4Maika RatriNo ratings yet
- Tooth-Support Over Dentures: An Approach To Preventive ProsthodonticsDocument5 pagesTooth-Support Over Dentures: An Approach To Preventive ProsthodonticsAdvanced Research PublicationsNo ratings yet
- Revascularization of Immature Permanent Incisors After Severe Extrusive Luxation InjuryDocument10 pagesRevascularization of Immature Permanent Incisors After Severe Extrusive Luxation InjuryEduardo CarrielNo ratings yet
- Labial Access For Lower TeethDocument3 pagesLabial Access For Lower TeethHarish ChowdaryNo ratings yet
- Loss of Anterior TissuesDocument5 pagesLoss of Anterior Tissuesjinny1_0No ratings yet
- CBCTDocument7 pagesCBCTPrevita NindaNo ratings yet
- 2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepDocument6 pages2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepTudor LupesNo ratings yet
- The Swing-Lock Denture - Its Use in Conventional Removable Partial Denture ProsthodonticsDocument3 pagesThe Swing-Lock Denture - Its Use in Conventional Removable Partial Denture ProsthodonticsElena Besliu100% (1)
- The Bio-Col TechniqueDocument9 pagesThe Bio-Col TechniquewnelsenNo ratings yet
- Bioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionDocument0 pagesBioabsorbable Root Analogue For Closure of Oroantral Comm After Tooth ExtractionTrinhTaNo ratings yet
- Patient Age Is No Contraindication To Endodontic TreatmentDocument3 pagesPatient Age Is No Contraindication To Endodontic TreatmentMelisa Agustine LeeNo ratings yet
- Clinical Response To A Vacant Post Space: Case ReportDocument7 pagesClinical Response To A Vacant Post Space: Case ReportVICTOR FERNANDO LAMAS LARANo ratings yet
- Severe Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportDocument5 pagesSevere Gingival Recession Caused by Orthodontic Rubber Band: A Case ReportanjozzNo ratings yet
- Prosthodontic Management of Severely ResorbedDocument2 pagesProsthodontic Management of Severely ResorbedAamir BugtiNo ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- Restoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationDocument5 pagesRestoration of The Severely Decayed Tooth Using Crown Lengthening With Simultaneous Tooth-PreparationIntelligentiaNo ratings yet
- Hemisection of A Severely Decayed Mandibular Molar: A Case ReportDocument4 pagesHemisection of A Severely Decayed Mandibular Molar: A Case Reportkartika tiaraNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- 563421.v1 PerioDocument15 pages563421.v1 Perioikeuchi_ogawaNo ratings yet
- External Cervical Resorption JC FinalDocument46 pagesExternal Cervical Resorption JC FinalKomal JadhavNo ratings yet
- Think Before You Extract - A Case of Tooth AutotransplantationDocument5 pagesThink Before You Extract - A Case of Tooth AutotransplantationBoris ChapelletNo ratings yet
- Surgical Extraction of Mandibular Third Molar in Pterygomandibular Space: A Case ReportDocument4 pagesSurgical Extraction of Mandibular Third Molar in Pterygomandibular Space: A Case ReportadriandjoNo ratings yet
- Forced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case ReportDocument4 pagesForced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case Reportikeuchi_ogawaNo ratings yet
- Skeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical StudyDocument13 pagesSkeletal Anchorage Augmentation in Extraction/Nonextraction Orthodontic Treatment: A Randomized Clinical Studyaleja.b7815No ratings yet
- The Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsFrom EverandThe Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsNo ratings yet
- Published 1593 Published 1612 Published 1913 Published 1919 Published 1978Document4 pagesPublished 1593 Published 1612 Published 1913 Published 1919 Published 1978leeperlhan2000No ratings yet
- Journal Pone 0132958 s001Document11 pagesJournal Pone 0132958 s001leeperlhan2000No ratings yet
- Accelerated Repetitive Transcranial Magnetic Stimulation in The Treatment of DepressionDocument8 pagesAccelerated Repetitive Transcranial Magnetic Stimulation in The Treatment of Depressionleeperlhan2000No ratings yet
- MMRDocument6 pagesMMRleeperlhan2000No ratings yet
- Voxel-Based Morphometry With Unified SegmentationDocument65 pagesVoxel-Based Morphometry With Unified Segmentationleeperlhan2000No ratings yet
- Wise MindDocument1 pageWise Mindleeperlhan2000No ratings yet
- The Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's SyndromeDocument10 pagesThe Use of Cone Beam CT (CBCT) in Di of True From Mimicking Eagle's Syndromeleeperlhan2000No ratings yet
- Substance Abuse Among Young PeopleDocument57 pagesSubstance Abuse Among Young Peopleleeperlhan2000No ratings yet
- Assessing Quality of Life For Adolescents in Taiwan: Regular ArticleDocument8 pagesAssessing Quality of Life For Adolescents in Taiwan: Regular Articleleeperlhan2000No ratings yet
- Eagle's Syndrome in An 11-Year-Old PatientDocument4 pagesEagle's Syndrome in An 11-Year-Old Patientleeperlhan2000No ratings yet
- Treatment of Drug AddictionDocument34 pagesTreatment of Drug Addictionleeperlhan2000No ratings yet
- Methadone Treatment in The U.S.ADocument43 pagesMethadone Treatment in The U.S.Aleeperlhan2000No ratings yet
- Brief Psychosocial Interventions For Substance AbuseDocument41 pagesBrief Psychosocial Interventions For Substance Abuseleeperlhan2000No ratings yet
- Analysis of Royal Vale Heath's "Take A Number From 1 To 30"Document2 pagesAnalysis of Royal Vale Heath's "Take A Number From 1 To 30"leeperlhan2000No ratings yet
- 13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, RegardlessDocument5 pages13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, Regardlessleeperlhan2000No ratings yet
- Tadeu Magalhaes - 250 Gags & Jokes For Comedy MagiciansDocument19 pagesTadeu Magalhaes - 250 Gags & Jokes For Comedy Magiciansleeperlhan2000100% (4)
- Suicide Risk Management ProtocolDocument3 pagesSuicide Risk Management Protocolleeperlhan2000No ratings yet
- A New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of IllnessDocument19 pagesA New Empirical Definition of Major Depressive Episode Recovery and Its Positive Impact On Future Course of Illnessleeperlhan2000No ratings yet
- Shared Decision Making。: The Massachusetts General Hospital/Mclean Hospital: Residency Handbook Of PsychiatryDocument1 pageShared Decision Making。: The Massachusetts General Hospital/Mclean Hospital: Residency Handbook Of Psychiatryleeperlhan2000No ratings yet
- Chapter 30 LamotrigineDocument7 pagesChapter 30 Lamotrigineleeperlhan2000No ratings yet
- Chapter 14 BuspironeDocument10 pagesChapter 14 Buspironeleeperlhan2000No ratings yet
- Basic Offshore Safety Induction and Emergency Training: CtsiDocument72 pagesBasic Offshore Safety Induction and Emergency Training: Ctsiangel coazoNo ratings yet
- Between Japan & Germany Related To Dentistry 1Document9 pagesBetween Japan & Germany Related To Dentistry 1Dr Riktesh SrivastavaNo ratings yet
- Techinques Coloredpencils Basics2Document7 pagesTechinques Coloredpencils Basics2Roland CepedaNo ratings yet
- Microstrip Patch Antenna and Its ApplicationDocument20 pagesMicrostrip Patch Antenna and Its ApplicationBrhane DadsoNo ratings yet
- Magne ProvisionalsDocument10 pagesMagne Provisionalsdrdanielsan100% (1)
- People vs. Siao, G.R. No. 126021 March 3, 2000Document3 pagesPeople vs. Siao, G.R. No. 126021 March 3, 2000Ria Evita RevitaNo ratings yet
- AREVA T&D Product RangeDocument10 pagesAREVA T&D Product RangeEduardo SolanoNo ratings yet
- Violence Against WomenDocument81 pagesViolence Against WomenOxfamNo ratings yet
- Hidden Valley Deed RestrictionsDocument2 pagesHidden Valley Deed Restrictionsapi-4678260460% (1)
- Sanitation, Plumbing Design & Installation: G. Dry and Wet StandpipeDocument10 pagesSanitation, Plumbing Design & Installation: G. Dry and Wet StandpipeDwight Swayne AlegrosNo ratings yet
- Experiment 3 (Sublimation and Melting Point Determination)Document13 pagesExperiment 3 (Sublimation and Melting Point Determination)Cheng BauzonNo ratings yet
- Synopsis: Rajiv Gandhi University of Health Sciences Karnataka State, BangaloreDocument17 pagesSynopsis: Rajiv Gandhi University of Health Sciences Karnataka State, BangaloreSANANo ratings yet
- Disaster Nursing NotesDocument4 pagesDisaster Nursing NotesChannelG100% (1)
- Academy of Economic Studies of Moldova: Performed by Artur CatanoiDocument3 pagesAcademy of Economic Studies of Moldova: Performed by Artur CatanoiArtur CatanoiNo ratings yet
- Bio-Botany Vol-2 - EM PDFDocument216 pagesBio-Botany Vol-2 - EM PDFsudha1987No ratings yet
- KonectDocument2 pagesKonectHellen DuNo ratings yet
- H250 H250 H250 H250: Variable Area FlowmeterDocument88 pagesH250 H250 H250 H250: Variable Area Flowmetercedar1015No ratings yet
- Kirlian Photograpy and Energy TappingDocument7 pagesKirlian Photograpy and Energy Tappingnblack3335140No ratings yet
- Codex Standard For Whey Cheeses: CODEX STAN A-7-1971, Rev. 2-2006Document3 pagesCodex Standard For Whey Cheeses: CODEX STAN A-7-1971, Rev. 2-2006hoda hassanNo ratings yet
- Act Critical Skills List Aug 20Document3 pagesAct Critical Skills List Aug 20RobertNo ratings yet
- 8 Sacred Secrets - Keys To Unlock Your Womb PDFDocument6 pages8 Sacred Secrets - Keys To Unlock Your Womb PDFDaniela IlieNo ratings yet
- Criminal Justice Reform ActDocument5 pagesCriminal Justice Reform ActDNAinfoNewYork100% (1)
- AAP Guia Practica Liquidos IVDocument12 pagesAAP Guia Practica Liquidos IVMiroslaba Avila DiazNo ratings yet
- Overview of Citric Acid Production From Aspergillus NigerDocument14 pagesOverview of Citric Acid Production From Aspergillus NigerPetru AstefanoaieNo ratings yet
- Exam - DRRRDocument3 pagesExam - DRRRmycah hagadNo ratings yet
- Fire Alarm Control (IFC 640)Document84 pagesFire Alarm Control (IFC 640)thephuocNo ratings yet