Download as pdf or txt
You might also like
- 10 DOH ProgramsDocument28 pages10 DOH ProgramsDhonnalyn Amene Caballero100% (6)
- Analysis of The Rate of Infant Mortality From I Month To I YearDocument62 pagesAnalysis of The Rate of Infant Mortality From I Month To I YearChukwuma NdubuisiNo ratings yet
- Research Proposal On Prevalence of PneumoniaDocument26 pagesResearch Proposal On Prevalence of Pneumoniasolomon demissew62% (13)
- Critique PaperDocument2 pagesCritique PaperJeanne Kamille Evangelista Pinili100% (4)
- The Strategy Behind Taiwan's COVID-19 Immunization Program National Security and Global SolidarityDocument18 pagesThe Strategy Behind Taiwan's COVID-19 Immunization Program National Security and Global Solidarity林冠年No ratings yet
- Samuel CHAPTER 1 CorrectionDocument10 pagesSamuel CHAPTER 1 CorrectionNaomi AkinwumiNo ratings yet
- Civ 028Document9 pagesCiv 028Deah RisbaNo ratings yet
- The Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataDocument12 pagesThe Effect of The COVID-19 Vaccine On Daily Cases and Deaths Based On Global Vaccine DataCorneliu PaschanuNo ratings yet
- Surveillance of Healthcare-Associated Infections in A Neonatal Intensive Care Unit in Italy During 2006 - 2010Document8 pagesSurveillance of Healthcare-Associated Infections in A Neonatal Intensive Care Unit in Italy During 2006 - 2010Refy Dwi Maltha PratiwiNo ratings yet
- Expanded Program On Immunization: Source: Weekly Epidemiological Record, WHO: No.46,2011,86.509-520)Document6 pagesExpanded Program On Immunization: Source: Weekly Epidemiological Record, WHO: No.46,2011,86.509-520)Abeer AguamNo ratings yet
- Expanded Program On Immunization: Source: Weekly Epidemiological Record, WHO: No.46,2011,86.509-520)Document6 pagesExpanded Program On Immunization: Source: Weekly Epidemiological Record, WHO: No.46,2011,86.509-520)Abeer AguamNo ratings yet
- 933-Article Text-3081-1-10-20221107Document5 pages933-Article Text-3081-1-10-20221107Andri Tri KuncoroNo ratings yet
- Guidelines For The Management of Suspected and Confirmed Bacterial Meningitis inDocument18 pagesGuidelines For The Management of Suspected and Confirmed Bacterial Meningitis inswr88kv5p2No ratings yet
- An Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsDocument15 pagesAn Analysis of Taiwan's Vaccination Services and Applications For Vaccine Injury CompensationsAnonymous FNZ3uR2AHsNo ratings yet
- Persevere in The Dynamic COVID-Zero Strategy in China To Gain A Precious Time Window For The FutureDocument2 pagesPersevere in The Dynamic COVID-Zero Strategy in China To Gain A Precious Time Window For The FutureBillNo ratings yet
- Expanded Program On ImmunizationDocument6 pagesExpanded Program On ImmunizationAiza Oronce100% (1)
- Journal Article PDFDocument10 pagesJournal Article PDFAlyssa marieNo ratings yet
- Surveillance and Outbreak Investigation StudentDocument11 pagesSurveillance and Outbreak Investigation Studentnura meccaNo ratings yet
- Influenza Vaccination Among Infection Control Teams A EUCIC Surve - 2020 - VaccDocument5 pagesInfluenza Vaccination Among Infection Control Teams A EUCIC Surve - 2020 - VaccSavaNo ratings yet
- Department of Health - Expanded Program On Immunization - 2012-05-16Document7 pagesDepartment of Health - Expanded Program On Immunization - 2012-05-16MasterclassNo ratings yet
- The Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Document11 pagesThe Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Satriya WibawaNo ratings yet
- OpenSAFELY. Effectiveness of COVID-19 vaccination in children and adolescentsDocument29 pagesOpenSAFELY. Effectiveness of COVID-19 vaccination in children and adolescentsPABLO HONDUVILLANo ratings yet
- The Impact of Rotavirus Mass Vaccination On Hospitalization Rates, Nosocomial Rotavirus Gastroenteritis and Secondary Blood Stream InfectionsDocument10 pagesThe Impact of Rotavirus Mass Vaccination On Hospitalization Rates, Nosocomial Rotavirus Gastroenteritis and Secondary Blood Stream InfectionsKollar RolandNo ratings yet
- HHS Public Access: A Comparison of Post-Elimination Measles Epidemiology in The United States, 2009 2014 Versus 2001 2008Document20 pagesHHS Public Access: A Comparison of Post-Elimination Measles Epidemiology in The United States, 2009 2014 Versus 2001 2008Titania YuliskaNo ratings yet
- Meningitis in Children Under Five Year of Age.: DR Farrukh Iqbal Roll Number 06Document23 pagesMeningitis in Children Under Five Year of Age.: DR Farrukh Iqbal Roll Number 06dr_hammadNo ratings yet
- Vaccines 11 00306Document10 pagesVaccines 11 00306Mr SoehartoNo ratings yet
- SceirdDocument9 pagesSceirdGiaWay HsuNo ratings yet
- Zamora-Ledezma Et Al. - 2020 - Biomedical Science To Tackle The COVID-19 PandemicDocument48 pagesZamora-Ledezma Et Al. - 2020 - Biomedical Science To Tackle The COVID-19 PandemicEli Díaz de ZamoraNo ratings yet
- M1.U2 Measuring and Comparing Disease Frequency - StudentDocument6 pagesM1.U2 Measuring and Comparing Disease Frequency - StudentHusni MubarakNo ratings yet
- National HIV Action Plan 2017-2025: Tallinn 2017Document31 pagesNational HIV Action Plan 2017-2025: Tallinn 2017MeriAndaniSiahaanNo ratings yet
- Changes in Childhood Vaccination During The Coronavirus Disease 2 - 2021 - VacciDocument7 pagesChanges in Childhood Vaccination During The Coronavirus Disease 2 - 2021 - VacciProfessor BiologiaNo ratings yet
- Ca Covid 19 Delta VariantDocument42 pagesCa Covid 19 Delta VariantKristine Joy Vivero BillonesNo ratings yet
- 32Document10 pages32María Jesús Maass OleaNo ratings yet
- Impact of COVID19 On Routine Immunization: A Cross-Sectional Study in SenegalDocument6 pagesImpact of COVID19 On Routine Immunization: A Cross-Sectional Study in SenegalAjeng SuparwiNo ratings yet
- Article Covid-19 Children ReviewDocument12 pagesArticle Covid-19 Children ReviewAlexRázuri100% (1)
- Measles Study PDFDocument8 pagesMeasles Study PDFWebster The-TechGuy LunguNo ratings yet
- Effectiveness of Vaccination Against Varicella in Children Under 5 Years in Puglia Italy 2006 2012Document7 pagesEffectiveness of Vaccination Against Varicella in Children Under 5 Years in Puglia Italy 2006 2012NurulAlviFauzianaNo ratings yet
- Varicella in Pediatric Oncology Patients in The Post-Vaccine Era-Analysis of Routine Hospital Data From Bavaria (Germany), 2005-2011Document13 pagesVaricella in Pediatric Oncology Patients in The Post-Vaccine Era-Analysis of Routine Hospital Data From Bavaria (Germany), 2005-2011Hizam ZulfhiNo ratings yet
- Acute Flaccid Paralysis Field Manual: For Communicable Diseases Surveillance StaffDocument29 pagesAcute Flaccid Paralysis Field Manual: For Communicable Diseases Surveillance StaffAuliyaa RahmahNo ratings yet
- Dengue Net Flyer 2006Document1 pageDengue Net Flyer 2006Neha SameerNo ratings yet
- Telehealth For Global Emergencies: Implications For Coronavirus Disease 2019 (COVID-19)Document6 pagesTelehealth For Global Emergencies: Implications For Coronavirus Disease 2019 (COVID-19)Niki Pratiwi WijayaNo ratings yet
- Directly Observed Treatment Short-Course (DOTS) For Tuberculosis Control Program in Gambella Regional State, Ethiopia: Ten Years ExperienceDocument8 pagesDirectly Observed Treatment Short-Course (DOTS) For Tuberculosis Control Program in Gambella Regional State, Ethiopia: Ten Years ExperienceTammy Utami DewiNo ratings yet
- Out 123Document8 pagesOut 123Ilvita MayasariNo ratings yet
- Acceptance of A COVID-19 VacciDocument12 pagesAcceptance of A COVID-19 VacciahmadNo ratings yet
- MeningitisDocument62 pagesMeningitisDaniela Ramírez DavilaNo ratings yet
- The First Ever Confirmed Case of COVID-19 in Australia Was On January 25, 2020. The Patient Came From Wuhan and Flew To Melbourne On January 19Document6 pagesThe First Ever Confirmed Case of COVID-19 in Australia Was On January 25, 2020. The Patient Came From Wuhan and Flew To Melbourne On January 19Rastie CruzNo ratings yet
- Invasive Pneumococcal Disease - Canada - Ca 2000-2011Document12 pagesInvasive Pneumococcal Disease - Canada - Ca 2000-2011Regina EnggelineNo ratings yet
- Dept. Expanded Program On ImmunizationDocument6 pagesDept. Expanded Program On ImmunizationknotstmNo ratings yet
- 10 1016@j Jiac 2017 02 014Document12 pages10 1016@j Jiac 2017 02 014Achmad YunusNo ratings yet
- Asia Covid EstrategiasDocument10 pagesAsia Covid EstrategiasJonell SanchezNo ratings yet
- Safety Monitoring of COVID-19 Vaccines in Hong KongDocument19 pagesSafety Monitoring of COVID-19 Vaccines in Hong KongCarrie ChanNo ratings yet
- Covid 19Document16 pagesCovid 19Mazia MansoorNo ratings yet
- Outside The Window by David Naga (Essay)Document5 pagesOutside The Window by David Naga (Essay)David NagaNo ratings yet
- Cost-Effectiveness Evidence - A Case Study: How To Use This DocumentDocument3 pagesCost-Effectiveness Evidence - A Case Study: How To Use This DocumentPragnesh ChauhanNo ratings yet
- 1331907497-Montasseretal 2011BJMMR1038Document12 pages1331907497-Montasseretal 2011BJMMR1038puppyhandaNo ratings yet
- Expanded Program On ImmunizationDocument4 pagesExpanded Program On ImmunizationKrizle AdazaNo ratings yet
- Chapter OneDocument8 pagesChapter OneHOPENo ratings yet
- Prognostic Factors and OutcomesDocument7 pagesPrognostic Factors and Outcomesyikeberabebaw123No ratings yet
- Long Covid RevDocument9 pagesLong Covid RevJorge Dávila GonzálezNo ratings yet
- Vaccine: SciencedirectDocument10 pagesVaccine: SciencedirectNenqx Inthandt C'bunqxzu TheaNo ratings yet
- Dr. Eaton DeclarationDocument47 pagesDr. Eaton DeclarationJonece DuniganNo ratings yet
- FundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014Document94 pagesFundingModel TBAndHIVConceptNote Final Ethiopia Oct15 2014tokumaNo ratings yet
- Beyond One Health: From Recognition to ResultsFrom EverandBeyond One Health: From Recognition to ResultsJohn A. HerrmannNo ratings yet
- Dog BiteDocument24 pagesDog BitekranthichokkakulaNo ratings yet
- Health Check Consent FormDocument4 pagesHealth Check Consent Formaxenic04No ratings yet
- Polio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemDocument13 pagesPolio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemPrabhakaran Aranganathan100% (3)
- Cough and Colds, Fever, Asthma Topical: Headache, Skin Diseases Diuretics Anti - FungalDocument7 pagesCough and Colds, Fever, Asthma Topical: Headache, Skin Diseases Diuretics Anti - FungalElpijong Mijares JugalbotNo ratings yet
- Standardized Health Messages Book (With Bookmarked Headings) PDFDocument350 pagesStandardized Health Messages Book (With Bookmarked Headings) PDFKyaw Zaw HeinNo ratings yet
- Tetanus 2014Document32 pagesTetanus 2014Vanya Tri WindisariNo ratings yet
- Splenectomy: DisclaimerDocument5 pagesSplenectomy: DisclaimerMimi FatinNo ratings yet
- Framework of National Cancer Control Program in IndonesiaDocument20 pagesFramework of National Cancer Control Program in IndonesiaIndonesian Journal of Cancer100% (3)
- Final Pmmvy (Faq) Bookelt PDFDocument18 pagesFinal Pmmvy (Faq) Bookelt PDFrajat jainNo ratings yet
- What Is Polio?: SymptomsDocument2 pagesWhat Is Polio?: SymptomsJP LandagoraNo ratings yet
- Bill Gates Bio & History: Who Is Bill Gates?Document12 pagesBill Gates Bio & History: Who Is Bill Gates?ChristCarrieMeNo ratings yet
- ABC's of Primary Health Care...Document24 pagesABC's of Primary Health Care...rhenier_ilado100% (7)
- "Expanded Program On Immunization": Angeles University FoundationDocument12 pages"Expanded Program On Immunization": Angeles University FoundationJaillah Reigne CuraNo ratings yet
- Acs Ca3 BookDocument69 pagesAcs Ca3 BookchrisNo ratings yet
- 085 The Crab Tales 29 April To 12 MayDocument20 pages085 The Crab Tales 29 April To 12 MayElizabeth KingNo ratings yet
- Landasan Teori Tetanus GeneralisataDocument22 pagesLandasan Teori Tetanus GeneralisataadityaNo ratings yet
- Anti Fungal Susceptibility TestingDocument13 pagesAnti Fungal Susceptibility TestingMohamed75% (4)
- Generic Risk Assessment New and Expectant MothersDocument10 pagesGeneric Risk Assessment New and Expectant MothersBga ArmyNo ratings yet
- Health INDICATORSDocument30 pagesHealth INDICATORSYeontan Kim100% (1)
- 06SMARTeZ Drug Stability Table Non USDocument2 pages06SMARTeZ Drug Stability Table Non USJessica Blaine BrumfieldNo ratings yet
- CDC Healthcare Personnel Vaccination RecommendationsDocument1 pageCDC Healthcare Personnel Vaccination RecommendationsdocktpNo ratings yet
- Moving Target Vaccines Thimerosol and AutismDocument25 pagesMoving Target Vaccines Thimerosol and AutismcirclestretchNo ratings yet
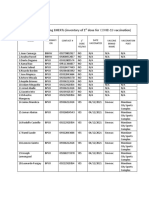
- Barangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Document1 pageBarangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Barangay CentroNo ratings yet
- Unit 10 Under My SkinDocument26 pagesUnit 10 Under My SkinYanz MuhamadNo ratings yet
- CPM17th RabiesDocument15 pagesCPM17th RabiesMae DoctoleroNo ratings yet
- Amniocentesis HindiDocument6 pagesAmniocentesis HindiRohit KumarNo ratings yet
- Surgical Prophylaxis: Prepared By: Gerard-IanDocument10 pagesSurgical Prophylaxis: Prepared By: Gerard-IanGerard-Ian de VeraNo ratings yet