Download as docx, pdf, or txt
You might also like
- RADIOLOGY - Clinical Radiology - The Essentials 4E (2014) (PDF) (UnitedVRG)Document562 pagesRADIOLOGY - Clinical Radiology - The Essentials 4E (2014) (PDF) (UnitedVRG)Andi Firmansyah90% (29)
- Affidavit of Surviving SpouseDocument1 pageAffidavit of Surviving SpouseAnonymous 75TDy2y50% (2)
- Funda Lecture SG #3Document9 pagesFunda Lecture SG #3Zsyd GelladugaNo ratings yet
- Contractors List of USADocument21 pagesContractors List of USAjerry 121100% (2)
- Core Network Services-High Level Design TemplateDocument15 pagesCore Network Services-High Level Design TemplateBryan Gavigan100% (1)
- Florence NightingaleDocument5 pagesFlorence NightingaleKristopher JacintosNo ratings yet
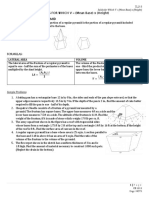
- SOLIDS FOR WHICH V (Mean Base) X (Height) Frustum of A Regular PyramidDocument4 pagesSOLIDS FOR WHICH V (Mean Base) X (Height) Frustum of A Regular PyramidGil John Awisen0% (1)
- Hildegard Peplau: Interpersonal Relationship TheoryDocument10 pagesHildegard Peplau: Interpersonal Relationship TheoryMariel Yanes GarciaNo ratings yet
- History of Nursing Law in The Philippines EditedDocument12 pagesHistory of Nursing Law in The Philippines Editedjandipot_kurikuripotNo ratings yet
- History of Nursing in The PhilippinesDocument2 pagesHistory of Nursing in The PhilippinesMarie Cel VirtucioNo ratings yet
- TIN Module 3 PDFDocument17 pagesTIN Module 3 PDFAudrey Aban AcostaNo ratings yet
- People v. Patalin, Jr.Document16 pagesPeople v. Patalin, Jr.John Michael BabasNo ratings yet
- Olfu Vision, Mission and Core ValuesDocument7 pagesOlfu Vision, Mission and Core ValuesNicole Calisay Verzosa100% (1)
- Legal Foundations of Nursing EducationDocument9 pagesLegal Foundations of Nursing EducationtruebluepawNo ratings yet
- Graduate School of NursingDocument11 pagesGraduate School of NursingpwunewsNo ratings yet
- Analysis of Movie Snowpiercer From The Issue of Ideology and Ideological State ApparatusDocument6 pagesAnalysis of Movie Snowpiercer From The Issue of Ideology and Ideological State Apparatus宏一封No ratings yet
- Nursing Market in PhilippinesDocument17 pagesNursing Market in Philippinesramit77No ratings yet
- 4Ps Nursing ProgramsDocument8 pages4Ps Nursing ProgramsPhanieNo ratings yet
- Informative Essay Final DraftDocument8 pagesInformative Essay Final Draftapi-302021014No ratings yet
- Nurse As EducatorDocument28 pagesNurse As Educatornaelnael chaaNo ratings yet
- History, Significance, and Analysis of Nursing Theory NewDocument23 pagesHistory, Significance, and Analysis of Nursing Theory NewferaNo ratings yet
- Hand Out Nursing History TimelineDocument13 pagesHand Out Nursing History TimelineRosemarie EustaquioNo ratings yet
- History of Nursing (Part 1)Document56 pagesHistory of Nursing (Part 1)Joseph TheThirdNo ratings yet
- Culture of The PhilippinesDocument24 pagesCulture of The Philippinesgian reyesNo ratings yet
- Case DigestDocument5 pagesCase DigestAlex Ian EvangelistaNo ratings yet
- TFNDocument34 pagesTFNpatriceNo ratings yet
- TFN - Quiz Module 4Document2 pagesTFN - Quiz Module 4April Ann Flores RamosNo ratings yet
- Leaving Against Medical AdviceDocument4 pagesLeaving Against Medical Advicef1400491No ratings yet
- PRC-BON Resolution No. 17 Series of 2010Document2 pagesPRC-BON Resolution No. 17 Series of 2010PhilippineNursingDirectory.comNo ratings yet
- Lecture 4Document17 pagesLecture 4rajeshkumarmbcetNo ratings yet
- Goal-Attainment Theory by Imogene KingDocument55 pagesGoal-Attainment Theory by Imogene KingGrace Lyn Borres ImpasNo ratings yet
- Euthanasia EssayDocument2 pagesEuthanasia Essaysophie_sherlock4917No ratings yet
- Anthropometric Measurements 2Document19 pagesAnthropometric Measurements 2Gajender SharmaNo ratings yet
- Florence NightingaleDocument3 pagesFlorence NightingaleMary Rose S DomingoNo ratings yet
- Theoretical Foundations in NursingDocument4 pagesTheoretical Foundations in NursingAl Cris BarroNo ratings yet
- RizalDocument10 pagesRizalBennard Cariño FajardoNo ratings yet
- Nursing Theory, Practice and ResearchDocument25 pagesNursing Theory, Practice and ResearchJoseph Levi G. DuranNo ratings yet
- Ubcv ReviewerDocument9 pagesUbcv ReviewerKim DimaanoNo ratings yet
- Code of Ethics For Fiipino NursesDocument4 pagesCode of Ethics For Fiipino NursesShaun Gabriel AmpoNo ratings yet
- Expt No 3 - Marquez, YDocument27 pagesExpt No 3 - Marquez, YYean MarquezNo ratings yet
- Nursing Service AdminsterationDocument208 pagesNursing Service Adminsterationhope bebeNo ratings yet
- Myra Levine'S Conservation ModelDocument13 pagesMyra Levine'S Conservation ModelPriya Mary PauloseNo ratings yet
- THEORETICAL FOUNDATION OF NURSING - Session 1 To 3Document11 pagesTHEORETICAL FOUNDATION OF NURSING - Session 1 To 3Mary LimlinganNo ratings yet
- Nursing Leadership TheoryDocument7 pagesNursing Leadership Theoryapi-480618512No ratings yet
- Our Lady of Fatima UniversityDocument7 pagesOur Lady of Fatima UniversityJess SyNo ratings yet
- Theoretical Foundations in NursingDocument9 pagesTheoretical Foundations in NursingYanis Emmanuelle LimNo ratings yet
- NCM 102 Notes (Physical Health)Document24 pagesNCM 102 Notes (Physical Health)Lc VillahermosaNo ratings yet
- Florence Nightingale: Environmental TheoryDocument25 pagesFlorence Nightingale: Environmental TheoryJAMES TONNY OKINYINo ratings yet
- Pre-Test: Lesson 5Document13 pagesPre-Test: Lesson 5MaeAnneMarceloTambio0% (1)
- TFN Prelim For PrintingDocument14 pagesTFN Prelim For PrintingjuNo ratings yet
- Martha RogersDocument27 pagesMartha RogersPewDiePie JuniorNo ratings yet
- Alzaga vs. SandiganbayanDocument1 pageAlzaga vs. SandiganbayanKelly RoxasNo ratings yet
- Indigenous Peoples of The Philippines: Prepared By: Jose R. GaviolaDocument17 pagesIndigenous Peoples of The Philippines: Prepared By: Jose R. GaviolaGeorge RosalNo ratings yet
- Candace Merl E. Gahisan BSN 1 - A Nursing Theorist: Katharine Kolcaba Title of Theory: Theory of Comfort Nursing Background: EducationDocument14 pagesCandace Merl E. Gahisan BSN 1 - A Nursing Theorist: Katharine Kolcaba Title of Theory: Theory of Comfort Nursing Background: EducationCandace Merl E. GahisanNo ratings yet
- Uts ReviewerDocument4 pagesUts ReviewerMA. LOUIMAR CATUNo ratings yet
- Phil FolkdanceDocument17 pagesPhil FolkdanceJay Carlo Bagayas0% (2)
- Module 2a Introduction To TheoryDocument29 pagesModule 2a Introduction To TheoryRon OpulenciaNo ratings yet
- History of NursingDocument4 pagesHistory of NursingLaica Kasan SidikNo ratings yet
- Unit 2 - Ideas and TermsDocument48 pagesUnit 2 - Ideas and TermsCalamdag Monzales Jhon MarkNo ratings yet
- Art Appreciation Lesson 1-3Document34 pagesArt Appreciation Lesson 1-3John Robert GasbanNo ratings yet
- (Current Trends and Issues in Nursing) Av Aid 3Document19 pages(Current Trends and Issues in Nursing) Av Aid 3Reshma rsrNo ratings yet
- History of Nursing in The PhilippinesDocument6 pagesHistory of Nursing in The PhilippinesWnwixiejwis Usisjdx8xjwiNo ratings yet
- History of Nursing in The PhilippinesDocument29 pagesHistory of Nursing in The PhilippinesNellie Ramos100% (3)
- History of Nursing - Raquenio-Trisha-DianneDocument9 pagesHistory of Nursing - Raquenio-Trisha-DianneTrisha Dianne RaquenioNo ratings yet
- MarzanoandKendall2007Taxonomy PDFDocument1 pageMarzanoandKendall2007Taxonomy PDFAnonymous 75TDy2yNo ratings yet
- CUR-F007 Curriculum Evaluation FormDocument3 pagesCUR-F007 Curriculum Evaluation FormAnonymous 75TDy2yNo ratings yet
- BSNDocument1 pageBSNAnonymous 75TDy2yNo ratings yet
- CTP Amacu 2014 PDFDocument2 pagesCTP Amacu 2014 PDFAnonymous 75TDy2yNo ratings yet
- Scholarship Examination SY 2018-2019: Application FormDocument3 pagesScholarship Examination SY 2018-2019: Application FormAnonymous 75TDy2yNo ratings yet
- BTP Menu 25 10 2018 Final PDFDocument4 pagesBTP Menu 25 10 2018 Final PDFAnonymous 75TDy2yNo ratings yet
- DOH Scholarship Application Form SampleDocument2 pagesDOH Scholarship Application Form SampleJohn Green100% (1)
- A Comparative Study of The Curriculum and Approach Towards Teaching Science: An International StudyDocument10 pagesA Comparative Study of The Curriculum and Approach Towards Teaching Science: An International StudyAnonymous 75TDy2yNo ratings yet
- CPRT 2013 PDFDocument1 pageCPRT 2013 PDFAnonymous 75TDy2yNo ratings yet
- The Obstacles Perceived by Critical Care Nurses in Performing Endotracheal SuctioningDocument7 pagesThe Obstacles Perceived by Critical Care Nurses in Performing Endotracheal SuctioningAnonymous 75TDy2yNo ratings yet
- Andorra's Constitution of 1993Document32 pagesAndorra's Constitution of 1993Anonymous 75TDy2yNo ratings yet
- Rocket Coffee Bar MenuDocument12 pagesRocket Coffee Bar MenuAnonymous 75TDy2yNo ratings yet
- Pathophysiology: Age of 46 Years Old, Gender (Female)Document1 pagePathophysiology: Age of 46 Years Old, Gender (Female)Anonymous 75TDy2yNo ratings yet
- Open House RouteDocument2 pagesOpen House RouteAnonymous 75TDy2yNo ratings yet
- File 5 SOPH, UWC, Health Promotion I Unit 4 OERFDocument18 pagesFile 5 SOPH, UWC, Health Promotion I Unit 4 OERFAnonymous 75TDy2yNo ratings yet
- Essi Respira ToDocument5 pagesEssi Respira ToAnonymous 75TDy2yNo ratings yet
- Out 175Document7 pagesOut 175Anonymous 75TDy2yNo ratings yet
- A Case Study:: - A 43-Year-Old Female, With Left Renal Stone, Presented To The Hospital AfterDocument1 pageA Case Study:: - A 43-Year-Old Female, With Left Renal Stone, Presented To The Hospital AfterAnonymous 75TDy2yNo ratings yet
- Under Martial LawDocument23 pagesUnder Martial LawAnonymous 75TDy2yNo ratings yet
- Describe One Memory Model With Reference To Research!Document10 pagesDescribe One Memory Model With Reference To Research!Thuý ThanhNo ratings yet
- RFP Development of Central Green Park in Gift City09092021011413Document151 pagesRFP Development of Central Green Park in Gift City09092021011413akashNo ratings yet
- TCCC Handbook Fall 2013Document192 pagesTCCC Handbook Fall 2013AMG_IA100% (4)
- Microprocessor - 8086 Addressing ModesDocument3 pagesMicroprocessor - 8086 Addressing ModesGaganBhayanaNo ratings yet
- Wachemo UniversityDocument48 pagesWachemo UniversityMarshet yohannes100% (1)
- Assesment BMDocument7 pagesAssesment BMTeja GajjarNo ratings yet
- Instructions / Checklist For Filling KYC FormDocument19 pagesInstructions / Checklist For Filling KYC FormPankaj KulkarniNo ratings yet
- Media and Information Literacy Is Defined As An Access To InformationDocument2 pagesMedia and Information Literacy Is Defined As An Access To InformationmarvinNo ratings yet
- Successful InterviewsDocument3 pagesSuccessful InterviewsRia SeprianiNo ratings yet
- HANA CV SampleDocument10 pagesHANA CV SampleJoy DeyNo ratings yet
- There's No Pill For This - IntroductionDocument4 pagesThere's No Pill For This - IntroductionChelsea Green PublishingNo ratings yet
- Samsung Brittle Fracture Evaluation - Additional Scope P23-0105-R3Document5 pagesSamsung Brittle Fracture Evaluation - Additional Scope P23-0105-R3Vipin NairNo ratings yet
- Memory Addressing and Instruction FormatsDocument9 pagesMemory Addressing and Instruction Formatsrobern ndoloNo ratings yet
- 1st Periodical Test in IctDocument3 pages1st Periodical Test in IctWander Mary81% (16)
- MSDS Artistri P5910 White Pigment Ink 071808Document10 pagesMSDS Artistri P5910 White Pigment Ink 071808Cisca BebetzNo ratings yet
- Adam Black2004Document8 pagesAdam Black2004Kókai BalázsNo ratings yet
- Basic Table Tennis DrillsDocument3 pagesBasic Table Tennis DrillsSadewa Putra Nussan100% (1)
- Embroidery Assistant: User Instruction GuideDocument92 pagesEmbroidery Assistant: User Instruction GuideAhlia Waqas AnjumNo ratings yet
- Research Process - StepsDocument31 pagesResearch Process - StepsPulkit SharmaNo ratings yet
- Simulink TutorialDocument15 pagesSimulink Tutorialsukhbir24No ratings yet
- Macroeconomics Principles Applications and Tools 8th Edition Osullivan Solutions ManualDocument26 pagesMacroeconomics Principles Applications and Tools 8th Edition Osullivan Solutions ManualMrJosephCruzMDfojy100% (63)
- Proper Preterism Vs Full Preterism - Steven Hawk PDFDocument115 pagesProper Preterism Vs Full Preterism - Steven Hawk PDFLeopoldoOrellanaAravena100% (1)
- Assignment Parts of SpeechDocument2 pagesAssignment Parts of SpeechFarman Ali KhaskheliNo ratings yet
- SilencerDocument6 pagesSilencerAlem HasicNo ratings yet
- Math InterventionDocument6 pagesMath InterventionPAOLO R. ALARDENo ratings yet
- Presentation About MyselfDocument18 pagesPresentation About MyselfbisnunepmanyNo ratings yet
- Soal B.ing LM Xii IpaDocument26 pagesSoal B.ing LM Xii IpaGuruh SasmitaNo ratings yet