Download as doc, pdf, or txt
You might also like
- ICSD3Document383 pagesICSD3Antonio100% (1)
- The Norton Psychology Reader by Gary Marcus (Editor)Document203 pagesThe Norton Psychology Reader by Gary Marcus (Editor)Elizaveta Semyanovskaya100% (3)
- I Am an Indigo Child – Hear My Words: Help Us Transcend Humanity Through the Upcoming Change of Consciousness and into the Next DimensionFrom EverandI Am an Indigo Child – Hear My Words: Help Us Transcend Humanity Through the Upcoming Change of Consciousness and into the Next DimensionNo ratings yet
- Introduction To CriminologyDocument100 pagesIntroduction To CriminologyJanille Hermosa100% (3)
- MSL 101 L11 Intro To Army LeadershipDocument14 pagesMSL 101 L11 Intro To Army LeadershipVetLegacyLdr100% (2)
- Richardson UDL Guidelines - Educator WorksheetDocument3 pagesRichardson UDL Guidelines - Educator WorksheetMelissa Maas RichardsonNo ratings yet
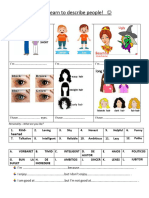
- Describing People Pre-Movers Adina Luiza CristinaDocument2 pagesDescribing People Pre-Movers Adina Luiza Cristinaivanoiuionela48No ratings yet
- 3rd ReportDocument12 pages3rd ReportAli AmadNo ratings yet
- Its Not Your FaultDocument30 pagesIts Not Your Faultcsiki.monika29No ratings yet
- Overcoming Depression - A trrue story of an African migrantFrom EverandOvercoming Depression - A trrue story of an African migrantNo ratings yet
- Wiyata Husada Samarinda: Sekolah Tinggi Ilmu Kesehatan (Stikes)Document1 pageWiyata Husada Samarinda: Sekolah Tinggi Ilmu Kesehatan (Stikes)anitaNo ratings yet
- Codependency BookDocument139 pagesCodependency BookScribdTranslationsNo ratings yet
- Basic Principles - RS - JhongDocument17 pagesBasic Principles - RS - JhongShanks Le RouxNo ratings yet
- Darcy Cole - Seduce Me How To Ignite Your Partners Passion Id1945874825 Size825Document153 pagesDarcy Cole - Seduce Me How To Ignite Your Partners Passion Id1945874825 Size825nilton_avilaNo ratings yet
- The Top 10 Traits of Highly Resilient People: Real Life Stories of Resilience Show You How to Build a Stress Resistant PersonalityFrom EverandThe Top 10 Traits of Highly Resilient People: Real Life Stories of Resilience Show You How to Build a Stress Resistant PersonalityRating: 5 out of 5 stars5/5 (1)
- WomenDocument5 pagesWomenNatalia RebeckaNo ratings yet
- 4 Year - Extra Material Handout 2021Document79 pages4 Year - Extra Material Handout 2021alejandroNo ratings yet
- Ethics Unit2 (Remulta)Document10 pagesEthics Unit2 (Remulta)remultarebelitoNo ratings yet
- AppendicesDocument36 pagesAppendicesgogetteraceNo ratings yet
- RegineDocument11 pagesRegineNellen Grace OrtizNo ratings yet
- English Sba SampleDocument15 pagesEnglish Sba Samplekollyb565No ratings yet
- Case Record Form For ChildrenDocument32 pagesCase Record Form For ChildrenPrasad javvajiNo ratings yet
- Ielts SpeakingDocument51 pagesIelts SpeakingLavanya Priya Sathyan100% (1)
- Internship Case ReportDocument32 pagesInternship Case Reportusama hayatNo ratings yet
- The Impact of Married by Accident ParentDocument28 pagesThe Impact of Married by Accident Parentemiliavalda02No ratings yet
- DESTINED2DOMINATE: Transition from a Supershy, To become a Solitary SavageFrom EverandDESTINED2DOMINATE: Transition from a Supershy, To become a Solitary SavageNo ratings yet
- The Anxious Buddhist by Stephen SantDocument168 pagesThe Anxious Buddhist by Stephen SantAlexander Lazarus WolffNo ratings yet
- 5 Powerful Habits To Dominate Life Inside and Outside The Gym PDFDocument22 pages5 Powerful Habits To Dominate Life Inside and Outside The Gym PDFRabu xoNo ratings yet
- Nur 413 RLE Week 2 Activity 1Document4 pagesNur 413 RLE Week 2 Activity 1ACIO, STEPHANY G.No ratings yet
- Cam 6 Test 1Document5 pagesCam 6 Test 1namhoangg2007No ratings yet
- Simplifying Your Life: Learning How to Live Instead of Just Existing!From EverandSimplifying Your Life: Learning How to Live Instead of Just Existing!No ratings yet
- Regular and Decaf: One Friend with Schizophrenia, One Friend with Bipolar, One Cup at a Time.From EverandRegular and Decaf: One Friend with Schizophrenia, One Friend with Bipolar, One Cup at a Time.No ratings yet
- How To Say NO To People Who Just Wont ListenDocument60 pagesHow To Say NO To People Who Just Wont ListenkikkyNo ratings yet
- Ab PsyDocument3 pagesAb PsyGabriel AlmeidaNo ratings yet
- Most To Least Most To Least: ST ND RD THDocument4 pagesMost To Least Most To Least: ST ND RD THRommel SarjNo ratings yet
- Children, Teens and Suicide LossDocument48 pagesChildren, Teens and Suicide LossJulieta Di RoccoNo ratings yet
- AdditionsDocument44 pagesAdditionsapi-276610794No ratings yet
- Parents Know BestDocument6 pagesParents Know BestleehomeNo ratings yet
- Personal Case Study: Introduction To Psychology 8:30 MWFDocument8 pagesPersonal Case Study: Introduction To Psychology 8:30 MWFShaira Ires Jumawid BrazaNo ratings yet
- Camir R QuestionnaireDocument3 pagesCamir R QuestionnaireScribdTranslations100% (1)
- 5404 1Document5 pages5404 1Inzamam Ul Haq HashmiNo ratings yet
- Lampiran 1. Etika Penelitian: Universitas Sumatera UtaraDocument13 pagesLampiran 1. Etika Penelitian: Universitas Sumatera UtaraMul YaniNo ratings yet
- 14appendices PDFDocument36 pages14appendices PDFAnonymous L77eD5uoNo ratings yet
- Survey FormDocument6 pagesSurvey FormKrishnaveni MurugeshNo ratings yet
- Psychological Mind Games Parents Must Avoid with Their ChildrenFrom EverandPsychological Mind Games Parents Must Avoid with Their ChildrenNo ratings yet
- The Last Time I Felt ValuedDocument6 pagesThe Last Time I Felt Valueddaryl doxNo ratings yet
- Personal Development 12Document3 pagesPersonal Development 12xxthotslayerxx222No ratings yet
- Ingilis Dili-AytacDocument15 pagesIngilis Dili-AytacSevdaNo ratings yet
- Simpsons Doc RentréeDocument3 pagesSimpsons Doc RentréeCaroline BouchardNo ratings yet
- Explaining Suicide To Children and Young PeopleDocument4 pagesExplaining Suicide To Children and Young Peoplemohammed munafNo ratings yet
- From College To Covid: 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & Dollars: 24 Learned : 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & Dollars: 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & DestinyFrom EverandFrom College To Covid: 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & Dollars: 24 Learned : 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & Dollars: 24 Lessons Learned During Lockdown To Increase Your Drive, Destiny, & DestinyNo ratings yet
- I am the Resident: Becoming the Advocate Your Loved One Needs!From EverandI am the Resident: Becoming the Advocate Your Loved One Needs!No ratings yet
- Where Your Happiness Hides: 22 Beliefs and 1 simple code that will transform your lifeFrom EverandWhere Your Happiness Hides: 22 Beliefs and 1 simple code that will transform your lifeNo ratings yet
- Understanding Myself As A Counselor & IndividualDocument45 pagesUnderstanding Myself As A Counselor & IndividualGerieNo ratings yet
- Fortune Teller's Handbook: 20 Fun and Easy Techniques for Predicting the FutureFrom EverandFortune Teller's Handbook: 20 Fun and Easy Techniques for Predicting the FutureNo ratings yet
- Revision NotesDocument612 pagesRevision NotesSusi Rutmalem100% (2)
- Pollak 2013Document13 pagesPollak 2013Susi RutmalemNo ratings yet
- Bipolar and Related Disorders Induced by Sodium 4-Phenylbutyrate in A Male Adolescent With Bile Salt Export Pump Deficiency DiseaseDocument3 pagesBipolar and Related Disorders Induced by Sodium 4-Phenylbutyrate in A Male Adolescent With Bile Salt Export Pump Deficiency DiseaseSusi RutmalemNo ratings yet
- NeglectedDocument95 pagesNeglectedSusi RutmalemNo ratings yet
- A.1 Ethics 072012Document13 pagesA.1 Ethics 072012Susi RutmalemNo ratings yet
- Dyscalculia 160621081110Document13 pagesDyscalculia 160621081110Susi RutmalemNo ratings yet
- Ozonoff, 2015Document3 pagesOzonoff, 2015Susi RutmalemNo ratings yet
- E014158 FullDocument11 pagesE014158 FullSusi RutmalemNo ratings yet
- Presenters: Robert M. Gordon, PH.D., & Alan C. Tjeltveit, PH.DDocument118 pagesPresenters: Robert M. Gordon, PH.D., & Alan C. Tjeltveit, PH.DSusi RutmalemNo ratings yet
- Zinc Deficiency and Child Development: Maureen M BlackDocument6 pagesZinc Deficiency and Child Development: Maureen M BlackSusi RutmalemNo ratings yet
- Intellectual Ability and AssessmentDocument4 pagesIntellectual Ability and AssessmentSusi RutmalemNo ratings yet
- Genomics and The Classification of Mental Illness: Focus On Broader CategoriesDocument4 pagesGenomics and The Classification of Mental Illness: Focus On Broader CategoriesSusi RutmalemNo ratings yet
- Visual Teaching Strategies Lesson PlanDocument2 pagesVisual Teaching Strategies Lesson Planapi-363234642No ratings yet
- Lesson Plan TBLDocument9 pagesLesson Plan TBLAdolfo Limon CapacetaNo ratings yet
- Celebrity EssayDocument1 pageCelebrity EssayMary MendonçaNo ratings yet
- Psychiatry NotesDocument135 pagesPsychiatry Notesmerin sunilNo ratings yet
- Leadership Camp Training DesignDocument10 pagesLeadership Camp Training DesignLester Eslava Orpilla100% (2)
- Activity Design Sports ProgramDocument4 pagesActivity Design Sports ProgramTrisHa TreXie TraCy100% (2)
- Lesson Plan TemplateDocument3 pagesLesson Plan Templateapi-296883317No ratings yet
- Dunoon Rethinking LeadershipDocument21 pagesDunoon Rethinking LeadershipKilusang Ilagan Para Punong-BayanNo ratings yet
- Attachment 1 Scenario Packet V2Document57 pagesAttachment 1 Scenario Packet V2CBS Austin WebteamNo ratings yet
- Theories of Learning-Facilitating LearningDocument6 pagesTheories of Learning-Facilitating LearningKeisha ReccionNo ratings yet
- Brookside Garden Academy: Republic of The Philippines Department of EducationDocument5 pagesBrookside Garden Academy: Republic of The Philippines Department of Educationelize kay zapantaNo ratings yet
- Full ThesisDocument165 pagesFull Thesissivagiri.p100% (1)
- Creating A Positive Emotional CultureDocument8 pagesCreating A Positive Emotional Culturesuresh singhNo ratings yet
- Thesis Critique FormatDocument5 pagesThesis Critique Formatheatheredwardsmobile100% (2)
- Leadership and Team Building: Answer - 1Document3 pagesLeadership and Team Building: Answer - 1dua khanNo ratings yet
- Alexei Leontiev - On Vygotsky's Creative DevelopmentDocument28 pagesAlexei Leontiev - On Vygotsky's Creative DevelopmentOdraudeIttereipNo ratings yet
- Dispositional Vs Situational AttributionDocument6 pagesDispositional Vs Situational AttributionUmair Bin AhmadNo ratings yet
- Let RevDocument22 pagesLet RevJay-ar TubogNo ratings yet
- TSL3105 Teaching Listening and Speaking in The Primary ClassroomDocument10 pagesTSL3105 Teaching Listening and Speaking in The Primary ClassroomNanthini SubramaniamNo ratings yet
- Job Analysis (HRM) 05-05-2021Document28 pagesJob Analysis (HRM) 05-05-2021Dr Ayesha TariqNo ratings yet
- The Self and Culture: Moi - Idea of Person - Personne - Idea of The SelfDocument2 pagesThe Self and Culture: Moi - Idea of Person - Personne - Idea of The SelfCharityOriaNo ratings yet
- Negative Effects of TV On ChildrenDocument5 pagesNegative Effects of TV On Childrenmirinda147No ratings yet
- A Parents Guide To Learning Difficulties PDFDocument130 pagesA Parents Guide To Learning Difficulties PDFSusan Christen GrandjeanNo ratings yet
- Getting Him/her Ready For School .Document18 pagesGetting Him/her Ready For School .Nicole Chandrix LajaraNo ratings yet
- LET Professional Education 5Document25 pagesLET Professional Education 5ens0304No ratings yet