Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HP Pavilion 14-F002laDocument32 pagesHP Pavilion 14-F002laRaul Lopez ReinaNo ratings yet
- Yamaha R6 2007 Varios Modelos PDFDocument538 pagesYamaha R6 2007 Varios Modelos PDFCARLOSNo ratings yet
- Emedicine Hypersemesis GravidarumDocument26 pagesEmedicine Hypersemesis GravidarumAnonymous 3OoumAUytNo ratings yet
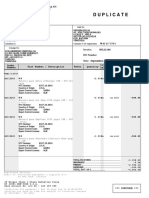
- Duplicate: Invoice: DO NumberDocument2 pagesDuplicate: Invoice: DO NumberLiau Zhan HongNo ratings yet
- Manual Solution Fundamentals Cosmology RichDocument43 pagesManual Solution Fundamentals Cosmology Richrscaraca100% (1)
- Living Rosary 2022Document17 pagesLiving Rosary 2022AhnNo ratings yet
- Prof. Stefano Benedicenti: Dean of Endodotic, Restorative and Laser Dental DepartmentDocument7 pagesProf. Stefano Benedicenti: Dean of Endodotic, Restorative and Laser Dental DepartmentAsif IqbalNo ratings yet
- Prueba - Inequalities - QuizletDocument14 pagesPrueba - Inequalities - QuizletNICOLAS CASTELLANOS TAMAYONo ratings yet
- Xi Chemistry Past Paper Karachi Board: Page 1 of 68Document68 pagesXi Chemistry Past Paper Karachi Board: Page 1 of 68salman100% (1)
- PT-4 Week 2 ExercisesDocument3 pagesPT-4 Week 2 ExercisesElijah Judson AlanzalonNo ratings yet
- Aqua Puss Instruction Manual 701: Dunlop Manufacturing, Inc. P.O. Box 846 Benicia, Ca 94510 U.S.ADocument2 pagesAqua Puss Instruction Manual 701: Dunlop Manufacturing, Inc. P.O. Box 846 Benicia, Ca 94510 U.S.AJohn JonesNo ratings yet
- MaglevDocument10 pagesMaglevCaramihai DenisNo ratings yet
- SAP HANA Cloud in A NutshellDocument288 pagesSAP HANA Cloud in A NutshellSumit MahanagNo ratings yet
- Mini Project Report On: Visvesvaraya Technological UniversityDocument8 pagesMini Project Report On: Visvesvaraya Technological UniversityTejáś ĢøwđâNo ratings yet
- Brgy. Songsong ConcretingDocument29 pagesBrgy. Songsong ConcretingRvin Jay Cabontocan Mariano100% (1)
- GemologyDocument7 pagesGemologyManish MalhotraNo ratings yet
- BADMINTON 1st and 2nd DiscussionDocument21 pagesBADMINTON 1st and 2nd DiscussionLyka Mae De GuzmanNo ratings yet
- Example Lab ReportDocument20 pagesExample Lab ReportbobtentpegNo ratings yet
- BM SA ROPE ATTACHMENTS HRDocument4 pagesBM SA ROPE ATTACHMENTS HRTheo van der BergNo ratings yet
- John Aebercrombie Concepts For Jazz Guitar Improvisation AbmajGmDocument3 pagesJohn Aebercrombie Concepts For Jazz Guitar Improvisation AbmajGmIsrael CevallosNo ratings yet
- Water Level Controller Using 8051 Circuit PrincipleDocument4 pagesWater Level Controller Using 8051 Circuit PrincipleLappi SchematicsNo ratings yet
- Barbell Medicine 12wk Press v2Document924 pagesBarbell Medicine 12wk Press v2Wen YNo ratings yet
- Res#2018-697 PROVINCIAL ORDINANCE NO. 2018-177 - Responsible Pet Ownership Ordinance of 2018Document6 pagesRes#2018-697 PROVINCIAL ORDINANCE NO. 2018-177 - Responsible Pet Ownership Ordinance of 2018Imarie Pinuela100% (1)
- GAILGas ExistingCNGStationsDocument4 pagesGAILGas ExistingCNGStationsclass xNo ratings yet
- Product Maintenance Manual: HIK/72XXHVI-SVDocument15 pagesProduct Maintenance Manual: HIK/72XXHVI-SVMilton Pereira Dos SantosNo ratings yet
- Hawke 711 Assembly InstructionDocument4 pagesHawke 711 Assembly InstructiongeneraljomoNo ratings yet
- Citrobacter Freundii: (Atcc 8090™)Document2 pagesCitrobacter Freundii: (Atcc 8090™)carlosNo ratings yet
- 01-System Devices Configuration - Rev GDocument36 pages01-System Devices Configuration - Rev GPABITRA PATRANo ratings yet
- HerzogDocument28 pagesHerzogSreekanth RaviNo ratings yet
- Air-Main Charging Systems: DHS 4.0 Series Compact Assistants That Make A Big DifferenceDocument12 pagesAir-Main Charging Systems: DHS 4.0 Series Compact Assistants That Make A Big DifferenceandreaNo ratings yet