
NIH Public Access: Author Manuscript
NIH Public Access: Author Manuscript
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson PlanDocument6 pagesLesson Planrozel de la cruz100% (1)
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
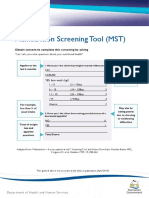
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Anabolic SteroidsDocument84 pagesAnabolic SteroidsRetno Rela Mahanani83% (6)
- Pharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MoreDocument3 pagesPharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MorepharmacydailyNo ratings yet
- Revenue CycleDocument0 pagesRevenue Cyclecasti134No ratings yet
- Registration Form: by Phone by Fax On The Web by MailDocument2 pagesRegistration Form: by Phone by Fax On The Web by MailjdrockeyNo ratings yet
- Magnesium EbookDocument19 pagesMagnesium Ebooksale18100% (9)
- Childhood ObesityDocument42 pagesChildhood ObesityLaTasha Ann Steven100% (3)
- DIR/Floortime ICDL Annual Conference November 11-13 2011Document8 pagesDIR/Floortime ICDL Annual Conference November 11-13 2011Floortime RepositoryNo ratings yet
- MBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveDocument10 pagesMBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveLina SantosNo ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet
- First Listening Test 1Document3 pagesFirst Listening Test 1Carles Sastre PérezNo ratings yet
- Antioxidant Properties of Garcinia Mangostana L (Mangosteen) RindDocument6 pagesAntioxidant Properties of Garcinia Mangostana L (Mangosteen) RindCristover FernandoNo ratings yet
- Puttur DetailDocument12 pagesPuttur DetailakileshNo ratings yet
- Immunology Exam 4 Study GuideDocument2 pagesImmunology Exam 4 Study GuideKeaton EisenmengerNo ratings yet
- SINP Excluded Occupation ListDocument5 pagesSINP Excluded Occupation ListMarjeanetteAgpaoaReyesNo ratings yet
- Price List Isamed'19Document10 pagesPrice List Isamed'19yohandaNo ratings yet
- Aroma TherapyDocument14 pagesAroma Therapysandhyapanicker1988No ratings yet
- TLIF6307A - Administer The Implementation of Fatigue Management Strategies - Learner GuideDocument83 pagesTLIF6307A - Administer The Implementation of Fatigue Management Strategies - Learner GuideromerofredNo ratings yet
- Decipher Final Year Updates-1Document10 pagesDecipher Final Year Updates-1Dr NnuNo ratings yet
- Food Microbiology, AASTUDocument119 pagesFood Microbiology, AASTUmikialeNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- Mouse PartsDocument1 pageMouse PartsBea JulongbayanNo ratings yet
- Skull FractureDocument13 pagesSkull FractureEddie LimNo ratings yet
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Journal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantDocument12 pagesJournal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantSebastian ChandraNo ratings yet
- Osteoporosis TALK ACR FINAL SK 11-10Document48 pagesOsteoporosis TALK ACR FINAL SK 11-10Liza EgudinsNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Diedrich Voderholzer Review OCPD PrintDocument11 pagesDiedrich Voderholzer Review OCPD PrintAbid AliNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson PlanDocument6 pagesLesson Planrozel de la cruz100% (1)
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Anabolic SteroidsDocument84 pagesAnabolic SteroidsRetno Rela Mahanani83% (6)
- Pharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MoreDocument3 pagesPharmacy Daily For Mon 14 Sep 2015 - ASMI Call To Speed Access, CMA Hails TGA CM Ticks, Hosp Phcy Standards, Weekly Comment and Much MorepharmacydailyNo ratings yet
- Revenue CycleDocument0 pagesRevenue Cyclecasti134No ratings yet
- Registration Form: by Phone by Fax On The Web by MailDocument2 pagesRegistration Form: by Phone by Fax On The Web by MailjdrockeyNo ratings yet
- Magnesium EbookDocument19 pagesMagnesium Ebooksale18100% (9)
- Childhood ObesityDocument42 pagesChildhood ObesityLaTasha Ann Steven100% (3)
- DIR/Floortime ICDL Annual Conference November 11-13 2011Document8 pagesDIR/Floortime ICDL Annual Conference November 11-13 2011Floortime RepositoryNo ratings yet
- MBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveDocument10 pagesMBEB - Mindfulness-Based Emotional Balance Teacher Training IntensiveLina SantosNo ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet
- First Listening Test 1Document3 pagesFirst Listening Test 1Carles Sastre PérezNo ratings yet
- Antioxidant Properties of Garcinia Mangostana L (Mangosteen) RindDocument6 pagesAntioxidant Properties of Garcinia Mangostana L (Mangosteen) RindCristover FernandoNo ratings yet
- Puttur DetailDocument12 pagesPuttur DetailakileshNo ratings yet
- Immunology Exam 4 Study GuideDocument2 pagesImmunology Exam 4 Study GuideKeaton EisenmengerNo ratings yet
- SINP Excluded Occupation ListDocument5 pagesSINP Excluded Occupation ListMarjeanetteAgpaoaReyesNo ratings yet
- Price List Isamed'19Document10 pagesPrice List Isamed'19yohandaNo ratings yet
- Aroma TherapyDocument14 pagesAroma Therapysandhyapanicker1988No ratings yet
- TLIF6307A - Administer The Implementation of Fatigue Management Strategies - Learner GuideDocument83 pagesTLIF6307A - Administer The Implementation of Fatigue Management Strategies - Learner GuideromerofredNo ratings yet
- Decipher Final Year Updates-1Document10 pagesDecipher Final Year Updates-1Dr NnuNo ratings yet
- Food Microbiology, AASTUDocument119 pagesFood Microbiology, AASTUmikialeNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- Mouse PartsDocument1 pageMouse PartsBea JulongbayanNo ratings yet
- Skull FractureDocument13 pagesSkull FractureEddie LimNo ratings yet
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Journal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantDocument12 pagesJournal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantSebastian ChandraNo ratings yet
- Osteoporosis TALK ACR FINAL SK 11-10Document48 pagesOsteoporosis TALK ACR FINAL SK 11-10Liza EgudinsNo ratings yet
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltDocument3 pagesAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniNo ratings yet
- Diedrich Voderholzer Review OCPD PrintDocument11 pagesDiedrich Voderholzer Review OCPD PrintAbid AliNo ratings yet