Download as docx, pdf, or txt
You might also like
- Williamoaks Construct GuideDocument14 pagesWilliamoaks Construct GuidefalergonNo ratings yet
- Stuxnet and Its Hidden Lessons On The Ethics of CyberweaponsDocument9 pagesStuxnet and Its Hidden Lessons On The Ethics of CyberweaponsprofcameloNo ratings yet
- History of Public Health Nursing in The PhilippinesDocument6 pagesHistory of Public Health Nursing in The PhilippinesClaudette Kyle Cornelio100% (1)
- Infertility: Dr. Carolina Paula C. MartinDocument6 pagesInfertility: Dr. Carolina Paula C. MartinMaikka IlaganNo ratings yet
- D75 14Document8 pagesD75 14JorgeCalvoLara100% (2)
- Types of ArthritisDocument3 pagesTypes of ArthritisSolomon Seth SallforsNo ratings yet
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Vasculitis ReviewDocument132 pagesVasculitis Reviewajmal_rashid@hotmail.com100% (2)
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDocument11 pagesDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- Dermatology Biologics Boards Fodder DIR Winter 2017Document6 pagesDermatology Biologics Boards Fodder DIR Winter 2017riskhakov100% (1)
- Gestational Trophoblastic Disease Pt2Document75 pagesGestational Trophoblastic Disease Pt2Abdullah KesalNo ratings yet
- Taking Obstetrical HistoryDocument20 pagesTaking Obstetrical Historymawada abdallaNo ratings yet
- Cerebral PalsyDocument14 pagesCerebral PalsyWaode SittrisnawatiNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- PATHO2 1.2 ImmunopathologyDocument9 pagesPATHO2 1.2 Immunopathologymiguel cuevasNo ratings yet
- Pathophysiology of AgingDocument5 pagesPathophysiology of AgingRemelou Garchitorena AlfelorNo ratings yet
- Rheuma (Gout, CPD, Rheumatoid Arthritis, Osteoarthritis)Document2 pagesRheuma (Gout, CPD, Rheumatoid Arthritis, Osteoarthritis)Jezreel Yanah De LeonNo ratings yet
- Differential Diagnosis Fever With RashDocument15 pagesDifferential Diagnosis Fever With RashJeetat OngNo ratings yet
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaNo ratings yet
- MCQ in GynecologyDocument5 pagesMCQ in GynecologySaber AlasmarNo ratings yet
- PEDS NOTES - QBank - EmmaDocument13 pagesPEDS NOTES - QBank - Emmasmian08No ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- Hernia Examination OSCE GuideDocument7 pagesHernia Examination OSCE GuideEssa AfridiNo ratings yet
- Part IIDocument64 pagesPart IIhussainNo ratings yet
- Leg MedDocument11 pagesLeg MedAradhanaRamchandaniNo ratings yet
- Abdominal Mass Differential PresentationDocument42 pagesAbdominal Mass Differential Presentationdeb haartNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- 1 Benign and Malignant Lesions of The CervixDocument46 pages1 Benign and Malignant Lesions of The CervixRohitNo ratings yet
- CPC For Students 2016Document10 pagesCPC For Students 2016Kwadwo Sarpong JnrNo ratings yet
- PEDIA para 08AMDocument17 pagesPEDIA para 08AMpedia blue bookNo ratings yet
- Legal Medicine Review PDFDocument10 pagesLegal Medicine Review PDFGhie TangonanNo ratings yet
- HistoplasmosisDocument12 pagesHistoplasmosis사이맄 진No ratings yet
- Pedia HXDocument3 pagesPedia HXeyakoyNo ratings yet
- Differential DiagnosisDocument10 pagesDifferential DiagnosisRhaffy Bearneza RapaconNo ratings yet
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Rheumatology OXF.: I. Immunology & InvestigationsDocument12 pagesRheumatology OXF.: I. Immunology & InvestigationsFarah FarahNo ratings yet
- Inflammatory & Immunologic Diseases IIIDocument252 pagesInflammatory & Immunologic Diseases IIIiamaldrinoNo ratings yet
- Surgery Cycle MCQSDocument27 pagesSurgery Cycle MCQSHeeb Warda100% (1)
- RobbinsBasicPathologyCha Small00center10 492010Document3 pagesRobbinsBasicPathologyCha Small00center10 492010Tony DawaNo ratings yet
- Neoplastic Diseases of The OvaryDocument61 pagesNeoplastic Diseases of The Ovaryea013No ratings yet
- Surg 3.4 - LiverDocument8 pagesSurg 3.4 - LiveryayayanizaNo ratings yet
- Infra-Auricular Mass Case PresDocument8 pagesInfra-Auricular Mass Case PresEjay Jacob RicamaraNo ratings yet
- (Surg2) 5.3 Urology Part 2 - Dr. YusiDocument19 pages(Surg2) 5.3 Urology Part 2 - Dr. YusiAlloiBialbaNo ratings yet
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDocument15 pagesCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarNo ratings yet
- Rheumatoid ArthritisDocument11 pagesRheumatoid ArthritisVerli Fajriati Nofli0% (1)
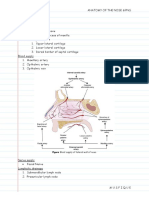
- Anatomy of The Nose & Paranasal Air SinusesDocument4 pagesAnatomy of The Nose & Paranasal Air SinusesMusfique RashidNo ratings yet
- Vasculitis MindnodeDocument1 pageVasculitis MindnodeToño VargasNo ratings yet
- 24 HR History 2Document2 pages24 HR History 2Arjun KatariaNo ratings yet
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- Pedia History Taking TemplateDocument5 pagesPedia History Taking TemplateNilfred SolatorioNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- Joint Pain - ApproachDocument32 pagesJoint Pain - ApproachHassan Bin AjmalNo ratings yet
- Gynecology HXDocument4 pagesGynecology HXlovelots1234No ratings yet
- Krok 2 Medicine (EN) Attempt Review 1Document52 pagesKrok 2 Medicine (EN) Attempt Review 1IS ZDNo ratings yet
- Krok 2 Medicine (EN) - Attempt Review 4Document52 pagesKrok 2 Medicine (EN) - Attempt Review 4IS ZDNo ratings yet
- Pedia Bacte Table 08amDocument25 pagesPedia Bacte Table 08ampedia blue bookNo ratings yet
- GYNECOLOGY - 2.8 B&M Lesions of The OvariesDocument6 pagesGYNECOLOGY - 2.8 B&M Lesions of The OvariesAngela CaguitlaNo ratings yet
- Headache History: Introduction - WIPPPDocument4 pagesHeadache History: Introduction - WIPPPAmjad_2020No ratings yet
- Sweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Cardiomyopathy Self StudyDocument3 pagesCardiomyopathy Self StudySolomon Seth SallforsNo ratings yet
- Part of Aorta Main Branch: AscendingDocument5 pagesPart of Aorta Main Branch: AscendingSolomon Seth SallforsNo ratings yet
- Cardio My Opa Thies ChartDocument2 pagesCardio My Opa Thies ChartSolomon Seth SallforsNo ratings yet
- Indications by ClassDocument1 pageIndications by ClassSolomon Seth SallforsNo ratings yet
- AV Block ChartDocument1 pageAV Block ChartSolomon Seth SallforsNo ratings yet
- Epidemiology Clinical Features Diagnosis Treatment EndocarditisDocument1 pageEpidemiology Clinical Features Diagnosis Treatment EndocarditisSolomon Seth SallforsNo ratings yet
- FOBS Test 2 Key SlidesDocument140 pagesFOBS Test 2 Key SlidesSolomon Seth SallforsNo ratings yet
- Book ListDocument3 pagesBook ListSolomon Seth SallforsNo ratings yet
- Introduction To Cardiovascular Radiography: Spencer M. Smith, M.D. August 24, 2007Document49 pagesIntroduction To Cardiovascular Radiography: Spencer M. Smith, M.D. August 24, 2007Solomon Seth SallforsNo ratings yet
- Neuro Practical I TablesDocument9 pagesNeuro Practical I TablesSolomon Seth Sallfors100% (1)
- Handout Cases, Childhood Disorders, PLMDocument12 pagesHandout Cases, Childhood Disorders, PLMSolomon Seth SallforsNo ratings yet
- Neuro Written I TablesDocument6 pagesNeuro Written I TablesSolomon Seth SallforsNo ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- A6: Mild Suicidal Ideation of Limited Frequency, Intensity, andDocument1 pageA6: Mild Suicidal Ideation of Limited Frequency, Intensity, andSolomon Seth SallforsNo ratings yet
- Neuro Written II TablesDocument10 pagesNeuro Written II TablesSolomon Seth SallforsNo ratings yet
- Well Woman LabDocument2 pagesWell Woman LabSolomon Seth SallforsNo ratings yet
- Personality Disorders ChartDocument11 pagesPersonality Disorders ChartSolomon Seth Sallfors100% (1)
- OMT & The Workplace: Basic Ergonomics & Poor Postural HabitsDocument51 pagesOMT & The Workplace: Basic Ergonomics & Poor Postural HabitsSolomon Seth Sallfors100% (1)
- Feature Delirium Dementia CausesDocument9 pagesFeature Delirium Dementia CausesSolomon Seth SallforsNo ratings yet
- Hx-Chart Humid Air: Humidity Ratio, G/KG (Dry Air)Document1 pageHx-Chart Humid Air: Humidity Ratio, G/KG (Dry Air)KundzoNo ratings yet
- PFI ES-5-1993 Cleaning of Fabricated PipingDocument4 pagesPFI ES-5-1993 Cleaning of Fabricated PipingRodrigo Chambilla VernazaNo ratings yet
- CRDB Bank Job Opportunities Customer ExperienceDocument4 pagesCRDB Bank Job Opportunities Customer ExperienceAnonymous FnM14a0No ratings yet
- New Record TDocument2 pagesNew Record Tapi-309280225No ratings yet
- Seven Paths To Perfection Kirpal SinghDocument52 pagesSeven Paths To Perfection Kirpal SinghjaideepkdNo ratings yet
- जनावरहरूमा फेनबेन्डाजोलको प्रयोग (Use of Fenbendazole in animals)Document17 pagesजनावरहरूमा फेनबेन्डाजोलको प्रयोग (Use of Fenbendazole in animals)Jibachha SahNo ratings yet
- Guyoga Fitness Tracker Instructions PDFDocument8 pagesGuyoga Fitness Tracker Instructions PDFcavaleramaxNo ratings yet
- General Definition of Sag and Tension in Electrical Transmission LinesDocument11 pagesGeneral Definition of Sag and Tension in Electrical Transmission Linesdskymaximus67% (3)
- Research GR 2 Pinaka Final 1Document36 pagesResearch GR 2 Pinaka Final 1Richeille JoshNo ratings yet
- Critical Analysis of Story Number 2Document12 pagesCritical Analysis of Story Number 2David MorganNo ratings yet
- Department of Business Administration: Submitted ToDocument15 pagesDepartment of Business Administration: Submitted Topinky271994No ratings yet
- An Introduction To Macroeconomics A Heterodox Approach To Economic Analysis 2Nd Edition Full ChapterDocument42 pagesAn Introduction To Macroeconomics A Heterodox Approach To Economic Analysis 2Nd Edition Full Chapterjohn.hill578100% (23)
- SyntaxDocument9 pagesSyntaxVeronicaTurtusanNo ratings yet
- BiossDocument11 pagesBiossPriyanka SharmaNo ratings yet
- Problems 1Document2 pagesProblems 1Rajiv KumarNo ratings yet
- Telangana CADocument26 pagesTelangana CAPudeti Raghusreenivas0% (1)
- Software Requirement Engineering - CS708 Power Point Slides Lecture-09Document25 pagesSoftware Requirement Engineering - CS708 Power Point Slides Lecture-09ALTAIRI SALEHNo ratings yet
- Complete Using ConditionalsDocument2 pagesComplete Using ConditionalsicecrisNo ratings yet
- COT1-3rd HirarkiyaDocument49 pagesCOT1-3rd HirarkiyaRommel LasugasNo ratings yet
- Water Flow Meter South AfricaDocument2 pagesWater Flow Meter South AfricaH2oNetNo ratings yet
- Dreams LuDocument325 pagesDreams Luscrib3030100% (1)
- Complete Research Ch1 5Document57 pagesComplete Research Ch1 5Angelie Regie J EstorqueNo ratings yet
- Environmental ScienceDocument2 pagesEnvironmental Sciencegillianbernice.alaNo ratings yet
- Week 1 Ethics Defined-1Document4 pagesWeek 1 Ethics Defined-1Timo ThsNo ratings yet
- PMEC Flash CardsDocument17 pagesPMEC Flash CardsHariyantoNo ratings yet
- Studying The Performance of Pongamia Biodiesel by Using Nano Partical Fuel AdditivesDocument6 pagesStudying The Performance of Pongamia Biodiesel by Using Nano Partical Fuel Additivessemi1919No ratings yet