Download as pdf or txt
You might also like
- The Fisher King WoundDocument6 pagesThe Fisher King WoundEdward L Hester100% (2)
- Smart Time Special Edition Grade 12 Teachers Book Web1Document307 pagesSmart Time Special Edition Grade 12 Teachers Book Web1Thùy Linh PhùngNo ratings yet
- Topic 2 ExercisesDocument6 pagesTopic 2 ExercisesRaniel Pamatmat0% (1)
- Eppd-A Discourse CommunityDocument11 pagesEppd-A Discourse Communityapi-254655486No ratings yet
- Residual Breast Tissue After Mastectomy, How Often and Where It Is LocatedDocument11 pagesResidual Breast Tissue After Mastectomy, How Often and Where It Is LocatedBunga Tri AmandaNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- Robotic Image Guided BiopsyDocument6 pagesRobotic Image Guided BiopsymnasihsNo ratings yet
- Surgery For Cervical Cancer Consensus & ControversiesDocument9 pagesSurgery For Cervical Cancer Consensus & ControversiesmilenahugueninNo ratings yet
- Analysis of Ovarian Tumor Pathology by Fourier Transform Infrared SpectrosDocument6 pagesAnalysis of Ovarian Tumor Pathology by Fourier Transform Infrared SpectrosDAVID ROSAS VARANo ratings yet
- Image Features of True Positive and False Negative Cancers in Screening MammogramsDocument9 pagesImage Features of True Positive and False Negative Cancers in Screening MammogramsTher RayNo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- Icru 82Document67 pagesIcru 82Aditya DisdusNo ratings yet
- Prognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTDocument13 pagesPrognostic Factors Affecting Survial and Recurrence in Patientes With Early Cervical Squamous Cell Cancer Following Radical HTfernandallmagalhaesNo ratings yet
- Jbo 025 116006Document16 pagesJbo 025 116006Jamaah Ki HendroNo ratings yet
- Consensus Guideline On Breast Cancer Lumpectomy MarginsDocument6 pagesConsensus Guideline On Breast Cancer Lumpectomy MarginsSubhamSarthakNo ratings yet
- 220101014arun BalajiDocument135 pages220101014arun Balajiعبدمالك GamesNo ratings yet
- Breast Cancer Screening Modalities, Recommendations, and Novel Imaging TechniquesDocument20 pagesBreast Cancer Screening Modalities, Recommendations, and Novel Imaging TechniquesZuriNo ratings yet
- Diagnosing Breast Cancer by Using Raman SpectrosDocument7 pagesDiagnosing Breast Cancer by Using Raman SpectrosVidal VillanuevaNo ratings yet
- Optical Imaging InbreastsDocument11 pagesOptical Imaging InbreastsCezara RasinarNo ratings yet
- (Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast CancerDocument5 pages(Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast Cancer최윤No ratings yet
- 816-Article Text-5949-1-10-20230609Document6 pages816-Article Text-5949-1-10-20230609NikadekPramesti Dewi Puspita SariNo ratings yet
- ObginDocument5 pagesObginNahrisyah Ulfa SafnaNo ratings yet
- Microwave Imaging For Breast Tumor Detection Using Uniplanar AMC Based CPW-fed Microstrip AntennaDocument13 pagesMicrowave Imaging For Breast Tumor Detection Using Uniplanar AMC Based CPW-fed Microstrip AntennakhyatichavdaNo ratings yet
- 宫腔镜-Transrectal Ultrasound-Guided Hysteroscopic Myomectomy of Submucosal Myomas With a Varying Degree of Myometrial PenetrationDocument14 pages宫腔镜-Transrectal Ultrasound-Guided Hysteroscopic Myomectomy of Submucosal Myomas With a Varying Degree of Myometrial PenetrationAmy ZhangNo ratings yet
- Palliative Mastectomy Revisited - PMCDocument4 pagesPalliative Mastectomy Revisited - PMCTony YongNo ratings yet
- Gastrectomía LaparoscópicaDocument7 pagesGastrectomía LaparoscópicaGreyza VelazcoNo ratings yet
- Omidiji 2017Document7 pagesOmidiji 2017Dewa OkaNo ratings yet
- Detection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009Document8 pagesDetection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009samouille6666No ratings yet
- Shape NejmDocument11 pagesShape NejmMicaela Cavii CaviglioneNo ratings yet
- EeDocument8 pagesEeEstiPramestiningtyasNo ratings yet
- Long-Term Cosmesis Following A Novel Schedule ofDocument7 pagesLong-Term Cosmesis Following A Novel Schedule ofEmin PehlivanogluNo ratings yet
- Diagnostics 10 00103Document13 pagesDiagnostics 10 00103Ahmed NomanNo ratings yet
- Benefits, Harms, and Cost-Effectiveness of Supplemental Ultrasonography Screening For Women With Dense BreastsDocument15 pagesBenefits, Harms, and Cost-Effectiveness of Supplemental Ultrasonography Screening For Women With Dense BreastsHarshoi KrishannaNo ratings yet
- Keywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMDocument13 pagesKeywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMChamar AshishNo ratings yet
- s12885 024 11831 8Document11 pagess12885 024 11831 8dk.iitkgp007No ratings yet
- KJR 17 59Document10 pagesKJR 17 59Regi FauzanNo ratings yet
- Jimed, Vol. 4, No. 1 Issn 2356-301X: Nova Aditya Surya Irawan, Gatot Murti Wibowo, KhumaidiDocument7 pagesJimed, Vol. 4, No. 1 Issn 2356-301X: Nova Aditya Surya Irawan, Gatot Murti Wibowo, KhumaidiNovia Indrii AstutieNo ratings yet
- Estudio LAACDocument10 pagesEstudio LAACGerardo Heber Delgado ValleNo ratings yet
- Vaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyDocument7 pagesVaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyFlor ZalazarNo ratings yet
- An Efficient Hybrid Data Mining Approach For Breast Tumors DiagnosisDocument9 pagesAn Efficient Hybrid Data Mining Approach For Breast Tumors DiagnosisRakeshconclaveNo ratings yet
- International Seminars in Surgical OncologyDocument8 pagesInternational Seminars in Surgical OncologyAhmad ShafiqNo ratings yet
- Oncologic Safety of Conservative Mastectomy in The Therapeutic SettingDocument10 pagesOncologic Safety of Conservative Mastectomy in The Therapeutic SettingIdaamsiyatiNo ratings yet
- Automated Breast Cancer Detection Using Machine Learning Techniques by Extracting Different Feature Extracting StrategiesDocument5 pagesAutomated Breast Cancer Detection Using Machine Learning Techniques by Extracting Different Feature Extracting Strategiesmanoj523No ratings yet
- Wood Module 3 AssignmentDocument2 pagesWood Module 3 Assignmentapi-591140528No ratings yet
- 10 1053@j Gastro 2019 12 018Document35 pages10 1053@j Gastro 2019 12 018PATRICIA HERNANDEZ CASTILLONo ratings yet
- An Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesDocument4 pagesAn Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesEditor IJRITCCNo ratings yet
- ManuscriptDocument5 pagesManuscriptAnisa Mulida SafitriNo ratings yet
- Angiosarcoma MamaDocument5 pagesAngiosarcoma MamaRaul Matute MartinNo ratings yet
- Applsci 10 00767 v3Document30 pagesApplsci 10 00767 v3meneeeeeNo ratings yet
- Proceedings of Spie: Breast Ultrasound Tomography: Bridging The Gap To Clinical PracticeDocument10 pagesProceedings of Spie: Breast Ultrasound Tomography: Bridging The Gap To Clinical Practicelcscosta2761No ratings yet
- Probabilistic Neural Network For Breast Cancer Classification - SpringerLinkDocument31 pagesProbabilistic Neural Network For Breast Cancer Classification - SpringerLinkberline djimeliNo ratings yet
- Thomson Reuters Indexing JournalsDocument7 pagesThomson Reuters Indexing JournalssanaNo ratings yet
- MRI of The Breast and Emerging TechnologiesDocument15 pagesMRI of The Breast and Emerging Technologiesგიორგი ჯიქიძე100% (1)
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDocument6 pagesJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionNo ratings yet
- Ultrasound Diagnosis of Breast Cancer-1Document27 pagesUltrasound Diagnosis of Breast Cancer-1Riza AstutiNo ratings yet
- EJGO2022054 Cervical CaDocument8 pagesEJGO2022054 Cervical CaRahmayantiYuliaNo ratings yet
- Research Article: Nonlinear Elasto-Mammography For Characterization of Breast Tissue PropertiesDocument11 pagesResearch Article: Nonlinear Elasto-Mammography For Characterization of Breast Tissue PropertiesNuno GueiralNo ratings yet
- The Comparison of Surgery and Chemo-Radio Therapy in Locally Recurrent Colorectal CancerDocument4 pagesThe Comparison of Surgery and Chemo-Radio Therapy in Locally Recurrent Colorectal CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Simple Ultrasound Rules To Distinguish Between Benign and Malignant Adnexal Masses Before Surgery: Prospective Validation by IOTA GroupDocument16 pagesSimple Ultrasound Rules To Distinguish Between Benign and Malignant Adnexal Masses Before Surgery: Prospective Validation by IOTA GroupherryNo ratings yet
- Mri - Best Practice - Bisi - 2020 PDFDocument7 pagesMri - Best Practice - Bisi - 2020 PDFBISI IndiaNo ratings yet
- CA MammaeDocument6 pagesCA MammaeRiaNo ratings yet
- Gastrointestinal Malignancies: A Practical Guide on Treatment TechniquesFrom EverandGastrointestinal Malignancies: A Practical Guide on Treatment TechniquesSuzanne RussoNo ratings yet
- Contrast-Enhanced MammographyFrom EverandContrast-Enhanced MammographyMarc LobbesNo ratings yet
- Ensayo Mundo NuevoDocument2 pagesEnsayo Mundo NuevoJoan Joel Cáceres RamirezNo ratings yet
- The Masses and Shadows of The Black Holes Sagittarius A and M87 in Modified Gravity (MOG)Document4 pagesThe Masses and Shadows of The Black Holes Sagittarius A and M87 in Modified Gravity (MOG)Joan Joel Cáceres RamirezNo ratings yet
- Primes IIDocument138 pagesPrimes IIJoan Joel Cáceres RamirezNo ratings yet
- Programme Study SessionDocument1 pageProgramme Study SessionJoan Joel Cáceres RamirezNo ratings yet
- A Hybrid Cutting Force Model For High-Speed Milling of Titanium AlloysDocument4 pagesA Hybrid Cutting Force Model For High-Speed Milling of Titanium Alloysabdsu75No ratings yet
- Eth Adapter CN User ManualDocument34 pagesEth Adapter CN User Manualfahim47No ratings yet
- Cambridge International AS & A Level: Mathematics 9709/42Document16 pagesCambridge International AS & A Level: Mathematics 9709/42Nam TranNo ratings yet
- Master Your Minutes Mini - UpdatedDocument12 pagesMaster Your Minutes Mini - UpdatedPongnateeNo ratings yet
- Kissinger The Secret SideDocument98 pagesKissinger The Secret Sidekaf_kingNo ratings yet
- On Discrete Metric Space - Azhin Mohammed RasulDocument22 pagesOn Discrete Metric Space - Azhin Mohammed RasulSamm SungNo ratings yet
- Lift Theory DescriptionDocument6 pagesLift Theory Descriptionmangvic07No ratings yet
- Curriculum Vitae - Eka Devi Wulandari (2019) PDFDocument3 pagesCurriculum Vitae - Eka Devi Wulandari (2019) PDFDipta VioniNo ratings yet
- Bringing Life Back To Classrooms Through Smart TeachingDocument4 pagesBringing Life Back To Classrooms Through Smart TeachingRaj KumarNo ratings yet
- Performance Assesment-A Shift From Intangibles To TangiblesDocument25 pagesPerformance Assesment-A Shift From Intangibles To Tangibles2005ravi100% (1)
- ChemistryDocument1 pageChemistrySayantanNo ratings yet
- T-035-All-Tenses 2Document1 pageT-035-All-Tenses 2F5A12 JimenaChuNo ratings yet
- Communication As A Tool For Effective Performance in Local GDocument47 pagesCommunication As A Tool For Effective Performance in Local GLuqmon Olawale100% (1)
- Chapter 8 - Financial AnalysisDocument4 pagesChapter 8 - Financial AnalysisLưu Ngọc Tường ViNo ratings yet
- Daily Dose Day - 35Document29 pagesDaily Dose Day - 35Sayan Chatterjee100% (1)
- Transient Results and Response Spectra: Sofistik 2020Document25 pagesTransient Results and Response Spectra: Sofistik 2020Chris LumyNo ratings yet
- Supporting Significant Life EventsDocument5 pagesSupporting Significant Life Eventschandni0810100% (1)
- ProvRem - DM WenceslaoDocument3 pagesProvRem - DM WenceslaoKath LimNo ratings yet
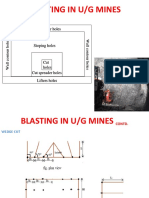
- Blasting in U/G Mines: Roof Contour Holes Roof Contour HolesDocument10 pagesBlasting in U/G Mines: Roof Contour Holes Roof Contour HolesSiddharth MukhillaNo ratings yet
- Paper Published PDFDocument16 pagesPaper Published PDFZeeshan SiddiqueNo ratings yet
- Designing Data Science: Rohan Raghavan Gavin SeewooruttunDocument12 pagesDesigning Data Science: Rohan Raghavan Gavin SeewooruttunNicolás Galavis VelandiaNo ratings yet
- V R Siddhartha Engineering College:: Vijayawada 17EC3701A: Antennas and Wave Propagation Questions Bank UNIT: I & II A.Y 2021-22Document2 pagesV R Siddhartha Engineering College:: Vijayawada 17EC3701A: Antennas and Wave Propagation Questions Bank UNIT: I & II A.Y 2021-22Narasimhareddy MmkNo ratings yet
- Decision-Making in Foreign Policy PDFDocument10 pagesDecision-Making in Foreign Policy PDFvishal rajput100% (1)
- A Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeDocument3 pagesA Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeIOSRjournalNo ratings yet
- 3 - Standing Movement Analysis WorksheetDocument2 pages3 - Standing Movement Analysis WorksheetMargarida PerestreloNo ratings yet
- Design Elements and PrinciplesDocument14 pagesDesign Elements and PrinciplesJaisurya SharmaNo ratings yet