
Document PDF
Document PDF
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Santiago Calle LawsuitDocument7 pagesSantiago Calle LawsuitNeil StreetNo ratings yet
- Porcelain Club - Letter To HarvardDocument2 pagesPorcelain Club - Letter To HarvardEvanNo ratings yet
- Bachelor Degree TimetableDocument20 pagesBachelor Degree Timetablebite meNo ratings yet
- PowerSCADA Expert System Integrators Manual v7.30Document260 pagesPowerSCADA Expert System Integrators Manual v7.30Hutch WoNo ratings yet
- APT1001.A2.01E.V1.0 - Preparation For Debug Kit SetupDocument2 pagesAPT1001.A2.01E.V1.0 - Preparation For Debug Kit SetupСергей КаревNo ratings yet
- Tree Plantation Strategy - GTRDocument37 pagesTree Plantation Strategy - GTRPapa RajuNo ratings yet
- DevynsresumeDocument2 pagesDevynsresumeapi-272399469No ratings yet
- Assignment Waqf Fazrihan DuriatDocument8 pagesAssignment Waqf Fazrihan DuriatFazrihan DuriatNo ratings yet
- Social Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshDocument7 pagesSocial Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshEditor IJTSRDNo ratings yet
- The Impact of Social Media On Educational Performance With Reference To College StudentsDocument5 pagesThe Impact of Social Media On Educational Performance With Reference To College StudentsIjcams PublicationNo ratings yet
- PT Bank MandiriDocument2 pagesPT Bank MandiriImanuel Kevin NNo ratings yet
- Trading Stocks With Camarilla PivotsDocument6 pagesTrading Stocks With Camarilla Pivotsluca pilottiNo ratings yet
- ICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)Document10 pagesICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)YAP LEE KHIMNo ratings yet
- Po17 - Tax Planning and AdviceDocument2 pagesPo17 - Tax Planning and AdvicepassmoreNo ratings yet
- Features of A CompanyDocument14 pagesFeatures of A Companyanshulagarwal62No ratings yet
- Social Responsibility in The Jewelry IndustryDocument6 pagesSocial Responsibility in The Jewelry IndustryMK ULTRANo ratings yet
- Exclusive Offer - Join Brazzers Only 1$ Today ! (Promo) : EX CL UsiveDocument9 pagesExclusive Offer - Join Brazzers Only 1$ Today ! (Promo) : EX CL UsiveSaulo BentoNo ratings yet
- A. H. M. Jones - Studies in Roman Government and Law-Basil Blackwell (1960)Document260 pagesA. H. M. Jones - Studies in Roman Government and Law-Basil Blackwell (1960)L V100% (1)
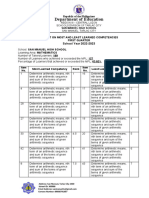
- Most and LEast LEarned Competencies 2022 2023 NUNAGDocument3 pagesMost and LEast LEarned Competencies 2022 2023 NUNAGJONATHAN NUNAGNo ratings yet
- Et Q Liqgsa: CFT/RQDocument2 pagesEt Q Liqgsa: CFT/RQvikash KumarNo ratings yet
- Del Rosario V ShellDocument2 pagesDel Rosario V Shellaratanjalaine0% (1)
- UNFCU Foundation Grant Application 2019Document4 pagesUNFCU Foundation Grant Application 2019Anonymous PbCsXeZNo ratings yet
- DocxDocument3 pagesDocxFarah Farah100% (1)
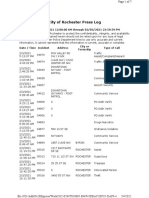
- RPD Daily Incident Report 2/3/21Document7 pagesRPD Daily Incident Report 2/3/21inforumdocsNo ratings yet
- Partograph 3Document49 pagesPartograph 3Geeta BhardwajNo ratings yet
- Taxation of Cross Border ActivitiesDocument5 pagesTaxation of Cross Border ActivitiesTriila manillaNo ratings yet
- EG L5 Incentivising and Disciplining ManagersDocument50 pagesEG L5 Incentivising and Disciplining ManagersPham Van HaNo ratings yet
- Life in The Universe 3rd Edition Bennett Test BankDocument35 pagesLife in The Universe 3rd Edition Bennett Test Bankjaundicecrincum05ba2100% (29)
- Analysis of Overlay For Airport Pavements CEAT Interrim ReportDocument54 pagesAnalysis of Overlay For Airport Pavements CEAT Interrim ReportJimmy ThomasNo ratings yet
- Tinder Reset GuideDocument13 pagesTinder Reset GuideAbel FekaduNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Santiago Calle LawsuitDocument7 pagesSantiago Calle LawsuitNeil StreetNo ratings yet
- Porcelain Club - Letter To HarvardDocument2 pagesPorcelain Club - Letter To HarvardEvanNo ratings yet
- Bachelor Degree TimetableDocument20 pagesBachelor Degree Timetablebite meNo ratings yet
- PowerSCADA Expert System Integrators Manual v7.30Document260 pagesPowerSCADA Expert System Integrators Manual v7.30Hutch WoNo ratings yet
- APT1001.A2.01E.V1.0 - Preparation For Debug Kit SetupDocument2 pagesAPT1001.A2.01E.V1.0 - Preparation For Debug Kit SetupСергей КаревNo ratings yet
- Tree Plantation Strategy - GTRDocument37 pagesTree Plantation Strategy - GTRPapa RajuNo ratings yet
- DevynsresumeDocument2 pagesDevynsresumeapi-272399469No ratings yet
- Assignment Waqf Fazrihan DuriatDocument8 pagesAssignment Waqf Fazrihan DuriatFazrihan DuriatNo ratings yet
- Social Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshDocument7 pagesSocial Media and Political Communication in India: An Analysis of 2017 Legislative Assembly Elections in Himachal PradeshEditor IJTSRDNo ratings yet
- The Impact of Social Media On Educational Performance With Reference To College StudentsDocument5 pagesThe Impact of Social Media On Educational Performance With Reference To College StudentsIjcams PublicationNo ratings yet
- PT Bank MandiriDocument2 pagesPT Bank MandiriImanuel Kevin NNo ratings yet
- Trading Stocks With Camarilla PivotsDocument6 pagesTrading Stocks With Camarilla Pivotsluca pilottiNo ratings yet
- ICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)Document10 pagesICGSE Y8 Maths Progression Test Mid-Year (Chapter1-11)YAP LEE KHIMNo ratings yet
- Po17 - Tax Planning and AdviceDocument2 pagesPo17 - Tax Planning and AdvicepassmoreNo ratings yet
- Features of A CompanyDocument14 pagesFeatures of A Companyanshulagarwal62No ratings yet
- Social Responsibility in The Jewelry IndustryDocument6 pagesSocial Responsibility in The Jewelry IndustryMK ULTRANo ratings yet
- Exclusive Offer - Join Brazzers Only 1$ Today ! (Promo) : EX CL UsiveDocument9 pagesExclusive Offer - Join Brazzers Only 1$ Today ! (Promo) : EX CL UsiveSaulo BentoNo ratings yet
- A. H. M. Jones - Studies in Roman Government and Law-Basil Blackwell (1960)Document260 pagesA. H. M. Jones - Studies in Roman Government and Law-Basil Blackwell (1960)L V100% (1)
- Most and LEast LEarned Competencies 2022 2023 NUNAGDocument3 pagesMost and LEast LEarned Competencies 2022 2023 NUNAGJONATHAN NUNAGNo ratings yet
- Et Q Liqgsa: CFT/RQDocument2 pagesEt Q Liqgsa: CFT/RQvikash KumarNo ratings yet
- Del Rosario V ShellDocument2 pagesDel Rosario V Shellaratanjalaine0% (1)
- UNFCU Foundation Grant Application 2019Document4 pagesUNFCU Foundation Grant Application 2019Anonymous PbCsXeZNo ratings yet
- DocxDocument3 pagesDocxFarah Farah100% (1)
- RPD Daily Incident Report 2/3/21Document7 pagesRPD Daily Incident Report 2/3/21inforumdocsNo ratings yet
- Partograph 3Document49 pagesPartograph 3Geeta BhardwajNo ratings yet
- Taxation of Cross Border ActivitiesDocument5 pagesTaxation of Cross Border ActivitiesTriila manillaNo ratings yet
- EG L5 Incentivising and Disciplining ManagersDocument50 pagesEG L5 Incentivising and Disciplining ManagersPham Van HaNo ratings yet
- Life in The Universe 3rd Edition Bennett Test BankDocument35 pagesLife in The Universe 3rd Edition Bennett Test Bankjaundicecrincum05ba2100% (29)
- Analysis of Overlay For Airport Pavements CEAT Interrim ReportDocument54 pagesAnalysis of Overlay For Airport Pavements CEAT Interrim ReportJimmy ThomasNo ratings yet
- Tinder Reset GuideDocument13 pagesTinder Reset GuideAbel FekaduNo ratings yet