Download as pdf or txt
You might also like
- 209-Hematology Review - Case StudiesDocument129 pages209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- Breathing, Sensing and Expressing Emotions: The Influence of Elsa Gindler and Mary Wigman On Body Psychotherapy and Dance/movement TherapyDocument16 pagesBreathing, Sensing and Expressing Emotions: The Influence of Elsa Gindler and Mary Wigman On Body Psychotherapy and Dance/movement TherapytaspreNo ratings yet
- Arnett-Facial Keys To Orthodontic Diagnosis IIDocument17 pagesArnett-Facial Keys To Orthodontic Diagnosis IIFiorella Loli Pinto100% (1)
- Computer Vision SyndromeDocument18 pagesComputer Vision SyndromeAtika PrissiliaNo ratings yet
- SOAPIEDocument34 pagesSOAPIEEm Castillo100% (1)
- Clinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaDocument6 pagesClinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaKevin ArdiansyahNo ratings yet
- Comparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesDocument7 pagesComparison of The Outcome of Silicone Ahmed Glaucoma Valve Implantation With A Surface Area Between 96 and 184 MM in Adult EyesVlady BordaNo ratings yet
- Iris-Claw Intraocular Lenses To Correct Aphakia in The Absence of Capsule SupportDocument6 pagesIris-Claw Intraocular Lenses To Correct Aphakia in The Absence of Capsule SupportAnonymous k4F8sAs25No ratings yet
- Comparative Effects of Various Types of Toric Intraocular Lenses On Astigmatism CorrectionDocument9 pagesComparative Effects of Various Types of Toric Intraocular Lenses On Astigmatism CorrectionAndrés QueupumilNo ratings yet
- Sulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryDocument6 pagesSulcus Implantation of A Single-Piece Foldable Acrylic Intraocular Lens After Posterior Capsular Rupture in Cataract SurgeryPrizilia SaimimaNo ratings yet
- Ebn RugayDocument6 pagesEbn RugayJeffrey Barcelon TanglaoNo ratings yet
- s12886 022 02620 7Document8 pagess12886 022 02620 7MarioNo ratings yet
- Intraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformDocument6 pagesIntraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformAkhilesh KumarNo ratings yet
- Kag Rully (B.IG)Document7 pagesKag Rully (B.IG)Rully Dwi SaputraNo ratings yet
- Evaluation of SuturlessDocument7 pagesEvaluation of SuturlesskenapayaNo ratings yet
- Kruger 2000Document5 pagesKruger 2000Magista NugrahaNo ratings yet
- Highlights From The 2011 ICL/Toric ICL Experts Symposium: Insert ToDocument8 pagesHighlights From The 2011 ICL/Toric ICL Experts Symposium: Insert ToArif MohammadNo ratings yet
- Therapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismDocument7 pagesTherapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismStephanie PfengNo ratings yet
- Reverse Optic Capture of The SingleDocument10 pagesReverse Optic Capture of The SingleIfaamaninaNo ratings yet
- Ascrs 2Document7 pagesAscrs 2leokapilNo ratings yet
- 1112CRSTEuro Cs VinciguerraDocument3 pages1112CRSTEuro Cs VinciguerraR Andres Plaza ZNo ratings yet
- Jrs0215garzon 2Document9 pagesJrs0215garzon 2Enrique Ferrando BarbenaNo ratings yet
- Olsen 2012Document7 pagesOlsen 2012Camila GuerraNo ratings yet
- Jurnal Referat MataDocument8 pagesJurnal Referat MataWinda KristantiNo ratings yet
- Clinical Differences Between Toric Intraocular LenDocument8 pagesClinical Differences Between Toric Intraocular LenonderonderNo ratings yet
- s12886 017 0419 1Document8 pagess12886 017 0419 1Madhu C KNo ratings yet
- Vitrectomy Results in Proliferative Diabetic RetinopathyDocument3 pagesVitrectomy Results in Proliferative Diabetic RetinopathyRohamonangan TheresiaNo ratings yet
- Comparison of Corneal Biomechanical Properties Among AxialDocument8 pagesComparison of Corneal Biomechanical Properties Among AxialPutri kartiniNo ratings yet
- OPTH D 22 00381 ReviewerDocument18 pagesOPTH D 22 00381 ReviewerPedro SerraNo ratings yet
- Chalam 2010Document6 pagesChalam 2010Sonya MabroukNo ratings yet
- Ophthalmology: Journal of and Advance ResearchDocument7 pagesOphthalmology: Journal of and Advance ResearchAthenaeum Scientific PublishersNo ratings yet
- Ijo 07 02 264Document9 pagesIjo 07 02 264Imade Candra PNo ratings yet
- CASE CLE in HIGH MYOPIA PatientDocument8 pagesCASE CLE in HIGH MYOPIA Patientpriscilla christina natanNo ratings yet
- البحث الخامسDocument5 pagesالبحث الخامسReham Fawzy ElshinawyNo ratings yet
- Iris-Claw Intraocular Lens and Scleral-Fixated Posterior Chamber Intraocular Lens Implanations in Correcting AphakiaDocument7 pagesIris-Claw Intraocular Lens and Scleral-Fixated Posterior Chamber Intraocular Lens Implanations in Correcting AphakiaMuhammad SukriNo ratings yet
- 3 Piece IOL SCL FixDocument6 pages3 Piece IOL SCL FixTvrtka BenašićNo ratings yet
- Toric ICLDocument8 pagesToric ICLjbahalkehNo ratings yet
- Corneal Endothelial Morphologic Assessment in Pediatric Cataract Surgery With Intraocular Lens Implantation - A Comparison of Preoperative and Early Postoperative Specular MicrosDocument8 pagesCorneal Endothelial Morphologic Assessment in Pediatric Cataract Surgery With Intraocular Lens Implantation - A Comparison of Preoperative and Early Postoperative Specular MicrosRael Rodrigues Dos SantosNo ratings yet
- Increased Iris Thickness and Association With Primary Angle Closure GlaucomaDocument6 pagesIncreased Iris Thickness and Association With Primary Angle Closure GlaucomaNinda AstariNo ratings yet
- Jurnal KuDocument6 pagesJurnal KuTamsilNo ratings yet
- SocivoDocument16 pagesSocivoSlobodan MilovanovicNo ratings yet
- Kjo 32 172Document10 pagesKjo 32 172Nurul Dwi LestariNo ratings yet
- Wa0000Document7 pagesWa0000Ocha24 TupamahuNo ratings yet
- Clinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsDocument6 pagesClinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsAldoNo ratings yet
- Journal Reading Mata - Pricilia Dan NadyaDocument14 pagesJournal Reading Mata - Pricilia Dan Nadyastepanus 102018062No ratings yet
- Coscarelli, 2012Document8 pagesCoscarelli, 2012vitor auzierNo ratings yet
- 2016 Article 229Document7 pages2016 Article 229nisa_kartikaNo ratings yet
- Accepted Manuscript: 10.1016/j.ajo.2014.05.016Document20 pagesAccepted Manuscript: 10.1016/j.ajo.2014.05.016Anonymous iInKGkMCNo ratings yet
- Ijss Jun Oa14Document4 pagesIjss Jun Oa14Yunanda RizkiNo ratings yet
- Ijss Jun Oa14Document4 pagesIjss Jun Oa14Yunanda RizkiNo ratings yet
- Pediatric Cataract Surgery - Rate of Secondary Visual Axis Opacification Depending On Intraocular Lens TypeDocument7 pagesPediatric Cataract Surgery - Rate of Secondary Visual Axis Opacification Depending On Intraocular Lens TypedinimaslomanNo ratings yet
- IOL Power Calculation, Correction of Defocus - CH 4Document18 pagesIOL Power Calculation, Correction of Defocus - CH 4riveliNo ratings yet
- Advanced Ophthalmic Diagnostic Procedures and InbstrumentationDocument5 pagesAdvanced Ophthalmic Diagnostic Procedures and InbstrumentationSayoki GhoshNo ratings yet
- Influence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaDocument7 pagesInfluence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaIJAR JOURNALNo ratings yet
- s12886 022 02600 XDocument8 pagess12886 022 02600 XHariom ShuklaNo ratings yet
- Retrospective Analysis of Wavefront Optimized Myopic LASIK Comparison of Preoperative To Postoperative AstigmatismDocument9 pagesRetrospective Analysis of Wavefront Optimized Myopic LASIK Comparison of Preoperative To Postoperative AstigmatismAthenaeum Scientific PublishersNo ratings yet
- Single-Step Transepithelial PHDocument9 pagesSingle-Step Transepithelial PHlenniNo ratings yet
- The Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanDocument6 pagesThe Ocular Biometric and Corneal Topographic Characteristics of High-Anisometropic Adults in TaiwanNurul Falah KalokoNo ratings yet
- Kjo 32 163Document9 pagesKjo 32 163John ElfranNo ratings yet
- At Lisatri ArticleDocument10 pagesAt Lisatri ArticleStefoane MadalinNo ratings yet
- Lectura 1Document8 pagesLectura 1Carmen Pérez JuradoNo ratings yet
- Mertens - The Staar Toric ICLDocument4 pagesMertens - The Staar Toric ICLAndreea L. MihalceaNo ratings yet
- BR J Ophthalmol-2014-Chan-79-81 PDFDocument4 pagesBR J Ophthalmol-2014-Chan-79-81 PDFRomi Mauliza FauziNo ratings yet
- Evaluation of Outcome of Retropupillary Iris Claw Intraocular Lens Implantation After P.C.R in Cataract SurgeryDocument12 pagesEvaluation of Outcome of Retropupillary Iris Claw Intraocular Lens Implantation After P.C.R in Cataract SurgeryMihir ShahNo ratings yet
- Keeping HealthyDocument10 pagesKeeping Healthyermal_binoNo ratings yet
- Informed Consent FormDocument3 pagesInformed Consent FormMichelle Ray del ValNo ratings yet
- HypotensionDocument9 pagesHypotensiondanny17ph100% (1)
- Gordon's QuestionnaireDocument2 pagesGordon's QuestionnaireJelai DNo ratings yet
- Acute Mesenteric IschemiaDocument20 pagesAcute Mesenteric IschemiasolysanNo ratings yet
- OT For AutismDocument2 pagesOT For AutismArianna Apreutesei3152eri8oawiNo ratings yet
- CVDocument4 pagesCVapi-312365364No ratings yet
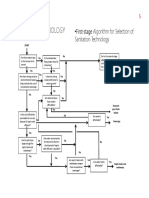
- FlowChart SeleksiTeknologiSANITASI PDFDocument3 pagesFlowChart SeleksiTeknologiSANITASI PDFClarita BangunNo ratings yet
- Chapter 50 Principles of PharmacologyDocument47 pagesChapter 50 Principles of PharmacologyTee WoodNo ratings yet
- Devlin2020 PDFDocument8 pagesDevlin2020 PDFMatias FlammNo ratings yet
- BDocument18 pagesBBenjamin Tantiansu100% (1)
- Clasificacion Senos MaxilaresDocument8 pagesClasificacion Senos MaxilaresSebastián BernalNo ratings yet
- BJR FOLFOX 6 DEBIRI Phase 2 TrialDocument7 pagesBJR FOLFOX 6 DEBIRI Phase 2 Trialpaquidermo85No ratings yet
- Energy Drink Exploritory PaperDocument7 pagesEnergy Drink Exploritory PaperJohn GoodmanNo ratings yet
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgNo ratings yet
- Form 2 Chapter 2 ExercisesDocument7 pagesForm 2 Chapter 2 ExercisesManisha Sekaran MuniandyNo ratings yet
- DNB Thesis Protocol StatusDocument6 pagesDNB Thesis Protocol Statuskulilev0bod3100% (2)
- MSDS Formic AcidDocument3 pagesMSDS Formic AcidChirag DobariyaNo ratings yet
- Classification and Management of Wounds: Warrington DivisionDocument2 pagesClassification and Management of Wounds: Warrington DivisionRoger ChristensenNo ratings yet
- Allison Pinto TestimonyDocument4 pagesAllison Pinto TestimonyficanetworkNo ratings yet
- Leptospirosis: Prof Anura Weerasinghe MD, FRCP, PHD, DCH, DTM&H, FC CPDocument16 pagesLeptospirosis: Prof Anura Weerasinghe MD, FRCP, PHD, DCH, DTM&H, FC CPanojanNo ratings yet
- Case Presentation-Nasopharyngeal CarcinomaDocument18 pagesCase Presentation-Nasopharyngeal Carcinomatehkie04100% (3)
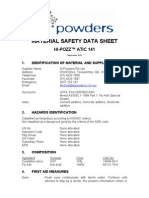
- Msds Hi PozzDocument6 pagesMsds Hi Pozzpenis1493No ratings yet
- Be The Prominent Dr. RombachDocument4 pagesBe The Prominent Dr. RombachRaziele RanesesNo ratings yet
- 4909Document2 pages4909Kevin Ariel Tiopan SimanjuntakNo ratings yet