Download as pdf or txt
You might also like
- Causes and Treatment of Malignant Melanoma: DiscussionDocument4 pagesCauses and Treatment of Malignant Melanoma: DiscussionAriSeliengNo ratings yet
- Burlington Ban On Noisy, Gas-Powered Leaf BlowersDocument2 pagesBurlington Ban On Noisy, Gas-Powered Leaf BlowersJoel Banner BairdNo ratings yet
- McqsDocument21 pagesMcqsOsama Bakheet100% (2)
- Measles PamphletDocument2 pagesMeasles Pamphletapi-384459604No ratings yet
- PDFDocument422 pagesPDFThuRein WinNo ratings yet
- CA de Piel y MelanomaDocument30 pagesCA de Piel y MelanomaDiego Bedón AscurraNo ratings yet
- MelanomaDocument10 pagesMelanomaShalu RjNo ratings yet
- Epidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergDocument12 pagesEpidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergGabriela AgrigNo ratings yet
- ABout Melanoma Skin CancerDocument11 pagesABout Melanoma Skin CancerOdair Braz JuniorNo ratings yet
- Melanoma: Epidemiology, Risk Factors, Pathogenesis, Diagnosis and ClassificationDocument7 pagesMelanoma: Epidemiology, Risk Factors, Pathogenesis, Diagnosis and ClassificationTirza StevanyNo ratings yet
- What Is Melanoma Skin Cancer?Document58 pagesWhat Is Melanoma Skin Cancer?Ruslan KamilNo ratings yet
- Biology ProjectDocument8 pagesBiology ProjectShivani Tyagi67% (6)
- Skin CancerDocument32 pagesSkin CancerAnkit GuptaNo ratings yet
- What You Should Know: Skin CancerDocument32 pagesWhat You Should Know: Skin CancerRicky WilliamsNo ratings yet
- Diagnosis and Management of Malignant MelanomaDocument10 pagesDiagnosis and Management of Malignant MelanomaDewinsNo ratings yet
- Melanoma Skin Cancer OverviewDocument39 pagesMelanoma Skin Cancer OverviewHardy WibowoNo ratings yet
- AnaPhy Skin Cancer Case Study-BASCODocument6 pagesAnaPhy Skin Cancer Case Study-BASCOChristine Jane BascoNo ratings yet
- MelanomaDocument1 pageMelanomaMarcus PiroteNo ratings yet
- MelanomaDocument19 pagesMelanomaAdhiguna PrabawaNo ratings yet
- Skin CancerDocument32 pagesSkin CancerTim StanleyNo ratings yet
- Ultraviolet Radiation and Skin CancerDocument10 pagesUltraviolet Radiation and Skin CancerPrathita AmandaNo ratings yet
- Melanoma FinallllDocument14 pagesMelanoma FinallllHIND MOHAMEDNo ratings yet
- Nurul Wahida BT Hamdan 030.08.301Document15 pagesNurul Wahida BT Hamdan 030.08.301Nor Ubudiah SetiNo ratings yet
- Assignment 1 (Cancer)Document8 pagesAssignment 1 (Cancer)Leo Aurelio MarcelinoNo ratings yet
- Skin Cancer: Problem: Skin Cancer Is One of The Most Common Types of Cancer in The UK. As ADocument11 pagesSkin Cancer: Problem: Skin Cancer Is One of The Most Common Types of Cancer in The UK. As AlalaNo ratings yet
- New Microsoft Office Word DocumentDocument23 pagesNew Microsoft Office Word DocumentMoinak GuhaNo ratings yet
- Questions I Asked MyselfDocument2 pagesQuestions I Asked Myselfapi-646942864No ratings yet
- Skin CancerDocument3 pagesSkin CancerourskrishNo ratings yet
- Biology ProjectDocument8 pagesBiology ProjectpragnyapratikshyapadhiNo ratings yet
- Cancer of The Larynx ComDocument10 pagesCancer of The Larynx ComKenneth ColeNo ratings yet
- Cancer For DummiesDocument26 pagesCancer For DummiesrkdivyaNo ratings yet
- Midgut Volvulus ABSTRACTDocument27 pagesMidgut Volvulus ABSTRACTely saktiNo ratings yet
- Skin CancerDocument5 pagesSkin Cancerapi-646942864No ratings yet
- MelanomaDocument11 pagesMelanomaAriSeliengNo ratings yet
- 3 Page PaperDocument4 pages3 Page Paperapi-252731818No ratings yet
- What Is CancerDocument16 pagesWhat Is CancerLee Teng LinNo ratings yet
- Malignancy ReportDocument52 pagesMalignancy Reportapi-3758497No ratings yet
- What Is CancerDocument15 pagesWhat Is CancerroggesterNo ratings yet
- Melanoma - PregradoDocument8 pagesMelanoma - PregradoDaniela DuránNo ratings yet
- What Is Lung CancerDocument9 pagesWhat Is Lung CancerpeterjongNo ratings yet
- Bio1010 Melanoma PaperDocument5 pagesBio1010 Melanoma Paperapi-300889005No ratings yet
- Cancer in Adults and ChildrenDocument21 pagesCancer in Adults and Childrenapi-313341021No ratings yet
- CCCC CC C CC CCCCCCCCCC CC CCCCCC CC CCC CCCC CC C CCCC CC C C RDocument10 pagesCCCC CC C CC CCCCCCCCCC CC CCCCCC CC CCC CCCC CC C CCCC CC C C RTulin Al JundiNo ratings yet
- Skin Cancer Research Paper 1Document4 pagesSkin Cancer Research Paper 1api-646942864No ratings yet
- The Most Common Cancer in The United StatesDocument3 pagesThe Most Common Cancer in The United StatesKrishnaKKrishnaNo ratings yet
- AbcdDocument2 pagesAbcda40198617No ratings yet
- Case Study g3p3 Am Shift Guzman LusungDocument38 pagesCase Study g3p3 Am Shift Guzman Lusungxuxi dulNo ratings yet
- Terapi SCC Kemo RadiasiDocument42 pagesTerapi SCC Kemo RadiasiAndreNo ratings yet
- 2.female Genital System IIDocument70 pages2.female Genital System IIأسود / BlackNo ratings yet
- Psy 512 CH 37Document3 pagesPsy 512 CH 37Maya GeeNo ratings yet
- CancerDocument4 pagesCancerDhanuAtmaNo ratings yet
- Breast CancerDocument7 pagesBreast CancerDeepankar Srigyan100% (1)
- Skin Cancer Editing DraftDocument4 pagesSkin Cancer Editing Draftapi-646942864No ratings yet
- Seminar On Cancer: Submitted To Submitted byDocument13 pagesSeminar On Cancer: Submitted To Submitted byUdaya Sree100% (1)
- NATIONAL CANCER CONTROL PROGRAMM 2 (Prakash)Document19 pagesNATIONAL CANCER CONTROL PROGRAMM 2 (Prakash)angayarkanni100% (1)
- Melanoma Skin CancerDocument62 pagesMelanoma Skin CancerHardy WibowoNo ratings yet
- TESTICULAR CANCER BookletDocument33 pagesTESTICULAR CANCER BookletCheeBrendaNo ratings yet
- Colorectal Cancer Epidemiology: Incidence, Mortality, Survival, and Risk FactorsDocument7 pagesColorectal Cancer Epidemiology: Incidence, Mortality, Survival, and Risk FactorsCamy CarmenNo ratings yet
- What Is Ovarian CancerDocument22 pagesWhat Is Ovarian CancersupahvyNo ratings yet
- Eval AnglaisDocument1 pageEval AnglaisSaloking NitogNo ratings yet
- CancerDocument24 pagesCancermiltynethouseNo ratings yet
- Uterine SarcomaDocument43 pagesUterine SarcomaherryNo ratings yet
- CancerDocument24 pagesCancerPavitam ChucksNo ratings yet
- Cannabis Expungement - S. 234Document6 pagesCannabis Expungement - S. 234Joel Banner BairdNo ratings yet
- City Wards in BurlingtonDocument1 pageCity Wards in BurlingtonJoel Banner BairdNo ratings yet
- Investigative Memo Richards 9-1-21 - RedactedDocument13 pagesInvestigative Memo Richards 9-1-21 - RedactedJoel Banner BairdNo ratings yet
- Letter To Dan Richardson, Esq.2021.09.06Document5 pagesLetter To Dan Richardson, Esq.2021.09.06Joel Banner BairdNo ratings yet
- Vermont Governor Marijuana Bill LetterDocument3 pagesVermont Governor Marijuana Bill LetterMarijuana MomentNo ratings yet
- Colcheste Ave Upgrade Alternatives (Jan. 11, 2021)Document59 pagesColcheste Ave Upgrade Alternatives (Jan. 11, 2021)Joel Banner BairdNo ratings yet
- Hot Times in The Queen CityDocument2 pagesHot Times in The Queen CityJoel Banner BairdNo ratings yet
- Cold Vs Flu Vs Allergies Vs Coronavirus PDFDocument1 pageCold Vs Flu Vs Allergies Vs Coronavirus PDFDavid HoreshNo ratings yet
- City Wards in BurlingtonDocument1 pageCity Wards in BurlingtonJoel Banner BairdNo ratings yet
- Hot Times in The Queen CityDocument2 pagesHot Times in The Queen CityJoel Banner BairdNo ratings yet
- Swede Midge Organic ManagementDocument4 pagesSwede Midge Organic ManagementJoel Banner BairdNo ratings yet
- CityPlace: Mayor Weinberger's Summary To City Council, Aug. 24, 2018Document2 pagesCityPlace: Mayor Weinberger's Summary To City Council, Aug. 24, 2018Joel Banner BairdNo ratings yet
- City Hall Park - Proposed Redesign, November 2016Document43 pagesCity Hall Park - Proposed Redesign, November 2016Joel Banner BairdNo ratings yet
- Burlinton Town CNTR - Settlement AgreementDocument6 pagesBurlinton Town CNTR - Settlement AgreementJoel Banner BairdNo ratings yet
- Challenge To Burlington Town Center in VT Enviro CourtDocument2 pagesChallenge To Burlington Town Center in VT Enviro CourtJoel Banner BairdNo ratings yet
- No To Mall Redevelopment: Petition Submitted Feb. 27, 2017Document8 pagesNo To Mall Redevelopment: Petition Submitted Feb. 27, 2017Joel Banner BairdNo ratings yet
- Official Ballot Special City Election Burlington, Vermont NOVEMBER 8, 2016Document2 pagesOfficial Ballot Special City Election Burlington, Vermont NOVEMBER 8, 2016NicoleNo ratings yet
- South End City Market - Art SoughtDocument6 pagesSouth End City Market - Art SoughtJoel Banner BairdNo ratings yet
- Map: Champlain Water District, 2016Document1 pageMap: Champlain Water District, 2016Joel Banner BairdNo ratings yet
- Predevelopment Agreement: & Waterfront Master Plan" ("Planbtv"), Which Contemplates The Redevelopment of TheDocument24 pagesPredevelopment Agreement: & Waterfront Master Plan" ("Planbtv"), Which Contemplates The Redevelopment of TheJoel Banner BairdNo ratings yet
- Raja Sir CampDocument6 pagesRaja Sir CampNivedan KothekarNo ratings yet
- Dinaburg Eval 2Document1 pageDinaburg Eval 2api-354606946No ratings yet
- Pricing of Cancer Medicines and Its ImpactDocument173 pagesPricing of Cancer Medicines and Its ImpactJennifer BuenoNo ratings yet
- Family Planning HandbookDocument387 pagesFamily Planning HandbookvthiseasNo ratings yet
- Demandes D'actions Correctives: Vendredi 21/09/12Document2 pagesDemandes D'actions Correctives: Vendredi 21/09/12Rochdi BahiriNo ratings yet
- The Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapDocument11 pagesThe Antibacterial Efficacy of Gotu Kola (Centella Asiatica) - Base SoapJohnnard BelenNo ratings yet
- Epidemiology Practice Exam Answers FallDocument20 pagesEpidemiology Practice Exam Answers Fallpmp123456No ratings yet
- CTH Food and Safety Practices Research, FinalDocument12 pagesCTH Food and Safety Practices Research, FinalAlexis OrganisNo ratings yet
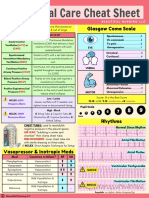
- Critical Care Cheat Sheet FreebieDocument2 pagesCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- Acupuncture: M. Kay Garcia and Joseph S. ChiangDocument1 pageAcupuncture: M. Kay Garcia and Joseph S. ChiangFaith Acu CureNo ratings yet
- Physics Folio... Simple2 Yg MungkinDocument15 pagesPhysics Folio... Simple2 Yg MungkinMuhammad HaikalNo ratings yet
- Performance Improvement Plan 2011-2012Document7 pagesPerformance Improvement Plan 2011-2012psynpNo ratings yet
- Common Errors in Xray Interpretation 2Document49 pagesCommon Errors in Xray Interpretation 2Shri RamaNo ratings yet
- Monera - With DPPDocument15 pagesMonera - With DPPAatreya DasNo ratings yet
- 2nd Peroxisome Metabolism 20760414Document56 pages2nd Peroxisome Metabolism 20760414Rawbeena RamtelNo ratings yet
- Parent Provider AgreementDocument5 pagesParent Provider AgreementDeepak SelaNo ratings yet
- Stroke Related Thesis TopicsDocument6 pagesStroke Related Thesis Topicskatrekahowardatlanta100% (2)
- Uddin322015ACRI22675 PDFDocument12 pagesUddin322015ACRI22675 PDFFarida Putri SyayarohNo ratings yet
- Diagnosis and Initial Management of NephrolithiasisDocument12 pagesDiagnosis and Initial Management of NephrolithiasisVina Marie DolorsoNo ratings yet
- G Spot BasicsDocument1 pageG Spot BasicsTirta Wahyudi100% (1)
- Introduction To Clinical TrialsDocument9 pagesIntroduction To Clinical Trialsmuhammad murtazaNo ratings yet
- (Hari 5) GHS Hazard Comm Labeling & SDS - 1Document61 pages(Hari 5) GHS Hazard Comm Labeling & SDS - 1Putra Adipradana100% (1)
- Case StudyDocument2 pagesCase Studyapi-244739669No ratings yet
- 1 Lower - Extremity Injuries inDocument30 pages1 Lower - Extremity Injuries inTien Khoa ReiNo ratings yet
- Khan Et Al-2017-Phytotherapy ResearchDocument12 pagesKhan Et Al-2017-Phytotherapy ResearchsanthiyasandyNo ratings yet
- Medical Gases CalculationsDocument14 pagesMedical Gases CalculationsNghiaNo ratings yet
- ImpressionDocument7 pagesImpressionAnnisa Nur AmalaNo ratings yet