Download as docx, pdf, or txt
You might also like
- History of Medical Technology ProfessionDocument5 pagesHistory of Medical Technology ProfessionJunnie Lastimosa33% (6)
- Module Code & Module Title CU6051NA - Artificial Intelligence Assessment Weightage & Type 20% Individual Coursework Year and Semester 2019-20 AutumnDocument10 pagesModule Code & Module Title CU6051NA - Artificial Intelligence Assessment Weightage & Type 20% Individual Coursework Year and Semester 2019-20 AutumnRey NeshNo ratings yet
- EtsyBusinessModel PDFDocument1 pageEtsyBusinessModel PDFChâu TheSheep100% (1)
- CH 1 CLINICAL TRIALS New 1 PDFDocument22 pagesCH 1 CLINICAL TRIALS New 1 PDFexcel proNo ratings yet
- Chiulli Paradigm Shift EssayDocument10 pagesChiulli Paradigm Shift Essayapi-741531928No ratings yet
- r101 Session1Document58 pagesr101 Session1Budsaba WiriyasirivajNo ratings yet
- Sesion 1 2 Textbook Pages 1-25Document24 pagesSesion 1 2 Textbook Pages 1-25Viviana LNo ratings yet
- Chemical and Bio Warefare Experiment ProgramsDocument17 pagesChemical and Bio Warefare Experiment ProgramsHåkøn Kyle Kjærulf100% (2)
- Gcpseminar 150412113701 Conversion Gate01Document71 pagesGcpseminar 150412113701 Conversion Gate01parminder.nain29No ratings yet
- Health Care Ethics Nuremberg Code IDocument41 pagesHealth Care Ethics Nuremberg Code ICyrille Aira AndresaNo ratings yet
- Weindling PJ (2008) The Nazi Medical ExperimentsDocument13 pagesWeindling PJ (2008) The Nazi Medical ExperimentscolectoraNo ratings yet
- History of Epidemiology: Presented By: Dr. Imrose Rashid Guide & Mentor: Dr. (Prof.) S.M. Salim KhanDocument32 pagesHistory of Epidemiology: Presented By: Dr. Imrose Rashid Guide & Mentor: Dr. (Prof.) S.M. Salim KhanBijay kumar kushwahaNo ratings yet
- MT 111 QuizzzzDocument16 pagesMT 111 QuizzzzKwin elleNo ratings yet
- 4 Research in HumansDocument9 pages4 Research in HumansMaelNo ratings yet
- MLS054 Lesson2Document6 pagesMLS054 Lesson2Allejah Jane CantaNo ratings yet
- Introduction To Medical TechnologyDocument18 pagesIntroduction To Medical TechnologyChrissa Mae Tumaliuan Catindoy100% (2)
- Modern MedicineDocument6 pagesModern MedicinePenny FebriantiNo ratings yet
- Breve Historia de La Investigacion MedicaDocument6 pagesBreve Historia de La Investigacion Medicayp24-0734No ratings yet
- The Tuskegee Syphilis Experiment: Carolinak12@Unc - EduDocument12 pagesThe Tuskegee Syphilis Experiment: Carolinak12@Unc - EdufirdausNo ratings yet
- If The Physician Diagnoses The Patient Wrongly He Would Get BeatenDocument4 pagesIf The Physician Diagnoses The Patient Wrongly He Would Get BeatenSheen GabatoNo ratings yet
- SGS Ethics in Research June 2019Document104 pagesSGS Ethics in Research June 2019Kumera Dinkisa ToleraNo ratings yet
- PMLS1 Module 1Document5 pagesPMLS1 Module 1Jonice NavarroNo ratings yet
- Evolution of Human ProtectionDocument6 pagesEvolution of Human ProtectionMelodia Turqueza GandezaNo ratings yet
- Lesson 1 Reviewer in PmlsDocument10 pagesLesson 1 Reviewer in PmlsCharisa Joyce AgbonNo ratings yet
- Chapter1 IntroductionDocument54 pagesChapter1 IntroductionMridul Mavila VeetilNo ratings yet
- Horrific US Medical Experiments Come To LightDocument2 pagesHorrific US Medical Experiments Come To Lighthalojumper63No ratings yet
- Module 7 STSDocument9 pagesModule 7 STSZaira NooyNo ratings yet
- The First Documented Human ExperimentDocument2 pagesThe First Documented Human ExperimentJohn Paul CamitanNo ratings yet
- PLMS First SemDocument50 pagesPLMS First Semshiella mae baltazarNo ratings yet
- Hom Top 8 SainiDocument4 pagesHom Top 8 SainiASHUTOSH GAMERNo ratings yet
- Pharmacology and Its Brief HistoryDocument4 pagesPharmacology and Its Brief HistoryNiala AlmarioNo ratings yet
- Experiments in Human Bodies During The Last Fifty Years in The UsaDocument19 pagesExperiments in Human Bodies During The Last Fifty Years in The UsaYou AbbyNo ratings yet
- A Brief History of PharmacologyDocument6 pagesA Brief History of PharmacologyymonnNo ratings yet
- History of Medical Technology in A Global ContextDocument4 pagesHistory of Medical Technology in A Global ContextwiljenetteNo ratings yet
- Perspectives Immunity ObomsawinDocument66 pagesPerspectives Immunity ObomsawinsabiontNo ratings yet
- Dr.H.O.GUNEWARDENE (Folder)Document38 pagesDr.H.O.GUNEWARDENE (Folder)Ian GardnerNo ratings yet
- Ethical Issues in ResearchDocument75 pagesEthical Issues in ResearchBensonNo ratings yet
- Microbiologists 1900-1950Document8 pagesMicrobiologists 1900-1950yeddayadao123No ratings yet
- Science 100: Science, Technology and Society: Lesson 2: Nature of TechnologyDocument9 pagesScience 100: Science, Technology and Society: Lesson 2: Nature of Technology이시연No ratings yet
- Holocasut Research Paper Experiments MJR EditsDocument14 pagesHolocasut Research Paper Experiments MJR EditsMaddie RoeNo ratings yet
- Human Hoodwinking Website FinalDocument20 pagesHuman Hoodwinking Website Finalapi-316552776100% (1)
- Modern Medicine: Causes of DiseaseDocument3 pagesModern Medicine: Causes of Diseasey17mitchellrNo ratings yet
- Ethics in Clinical TrialsDocument1 pageEthics in Clinical TrialsGems GlasgowNo ratings yet
- Beginings of MTDocument65 pagesBeginings of MTMel JamitoNo ratings yet
- Medical Technology: Principles of Medical Laboratory ScienceDocument17 pagesMedical Technology: Principles of Medical Laboratory ScienceDrusilla LossNo ratings yet
- A Brief History of PharmacologyDocument3 pagesA Brief History of PharmacologymIKXNo ratings yet
- Early Beginning of Medical Technology: Vivian HerrickDocument13 pagesEarly Beginning of Medical Technology: Vivian HerrickWho KnowsNo ratings yet
- QUOTESDocument6 pagesQUOTESRaymala RamanNo ratings yet
- Research EthicsDocument2 pagesResearch EthicsCarla HAHAHAHANo ratings yet
- Chahat CRR Mod 2Document20 pagesChahat CRR Mod 2tyagichahat052No ratings yet
- Take A Look at The Sample Page To Get An Idea of What Your Notebook Should Look Like. The Questions and Sample Answers Are Also Provided For YouDocument15 pagesTake A Look at The Sample Page To Get An Idea of What Your Notebook Should Look Like. The Questions and Sample Answers Are Also Provided For Youapi-329175631No ratings yet
- The Evolution of Pharmacy, Theme C, Level 1 The Development of MedicinesDocument3 pagesThe Evolution of Pharmacy, Theme C, Level 1 The Development of MedicinesSusmita Mistry JuiNo ratings yet
- Nuremberg CodeDocument5 pagesNuremberg CodeAmrita Singh100% (3)
- 50 Anos Do Tuskegee Syphilis Study BJournal 2022Document14 pages50 Anos Do Tuskegee Syphilis Study BJournal 2022Raphael Chalbaud Biscaia HartmannNo ratings yet
- Practical Research - Tuskegee ExperimentDocument24 pagesPractical Research - Tuskegee ExperimentNio MacalindongNo ratings yet
- 13 Most Evil US Government Human Experiments - War Is Crime-8Document8 pages13 Most Evil US Government Human Experiments - War Is Crime-8sagor sagor0% (1)
- Lock 1995Document8 pagesLock 1995Petrucio Augusto SDNo ratings yet
- Global Health Ethics EssayDocument4 pagesGlobal Health Ethics Essaylynnetted621No ratings yet
- Becoming Widely Available Associated Press Story External Icon Concluded PDF Iconexternal IconDocument5 pagesBecoming Widely Available Associated Press Story External Icon Concluded PDF Iconexternal IconmattyNo ratings yet
- A Brief History of PharmacologyDocument3 pagesA Brief History of PharmacologyHurley Reef100% (1)
- New Drug Development Process GenomicsDocument3 pagesNew Drug Development Process GenomicsanagheshNo ratings yet
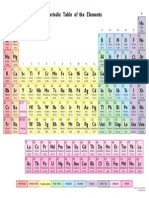
- Periodic Table ColorDocument1 pagePeriodic Table ColoranagheshNo ratings yet
- Cet - Mathematics - 2015 5: Version Code: A - 2Document7 pagesCet - Mathematics - 2015 5: Version Code: A - 2anagheshNo ratings yet
- 10 Myths JEE Aspirants Must KnowDocument14 pages10 Myths JEE Aspirants Must Knowabhiudeyvij100% (1)
- Automatic Blind Rivet Making PlantDocument4 pagesAutomatic Blind Rivet Making PlantsmarjanNo ratings yet
- Draft Resolution 1.0Document5 pagesDraft Resolution 1.0Priya SubramanianNo ratings yet
- Tropical Homes, Inc. vs. National Housing Authority - 1Document4 pagesTropical Homes, Inc. vs. National Housing Authority - 1PNP MayoyaoNo ratings yet
- Universal Mechanical Tester: Innovation With IntegrityDocument4 pagesUniversal Mechanical Tester: Innovation With IntegrityDlair Ramadan0% (1)
- Additions Basic Salary Fixed Allowance Days AttendedDocument3 pagesAdditions Basic Salary Fixed Allowance Days AttendedThiyagaraja ThilackshanNo ratings yet
- McKinsey 7S ModelDocument6 pagesMcKinsey 7S Modelpriyank1256No ratings yet
- Rizam Piat PresentationDocument17 pagesRizam Piat PresentationMohd RizNo ratings yet
- Intellectual Property Literature ReviewDocument17 pagesIntellectual Property Literature ReviewSashaNhara100% (1)
- YOLO-LITE: A Real-Time Object Detection Algorithm Optimized For Non-GPU ComputersDocument8 pagesYOLO-LITE: A Real-Time Object Detection Algorithm Optimized For Non-GPU ComputersDeepak Kumar SinghNo ratings yet
- PUBLIC Order For Preparation Release of Transcript Record of Grand JuryDocument4 pagesPUBLIC Order For Preparation Release of Transcript Record of Grand Jurykc wildmoon100% (1)
- Cabigas vs. PeopleDocument4 pagesCabigas vs. PeopleWilfredNo ratings yet
- Case Accounting - Air Asia BerhadDocument15 pagesCase Accounting - Air Asia BerhadWahyutri IndonesiaNo ratings yet
- Code Brochure 2022Document16 pagesCode Brochure 2022K SahinandanNo ratings yet
- Spec Pro Digests 3rd CompilationDocument12 pagesSpec Pro Digests 3rd CompilationKia FavorNo ratings yet
- Vesta Cylinder Shuttle Manual Part 1Document9 pagesVesta Cylinder Shuttle Manual Part 1celsribeiroNo ratings yet
- APO ReporteDocument162 pagesAPO ReporteJesús Pagó por TiNo ratings yet
- Diy Sls 3d PrinterDocument32 pagesDiy Sls 3d PrinterTF Escritório MGNo ratings yet
- The VerdictDocument4 pagesThe Verdicthttps://twitter.com/wagelabourNo ratings yet
- Nestle Vision MissionDocument1 pageNestle Vision MissionTrung Quân Trần0% (1)
- 6.stored Functions (Main Notes)Document5 pages6.stored Functions (Main Notes)Lakshman KumarNo ratings yet
- Company Name Address1 Address2 Area City Pincode Contact Number Designation Mobile URL Email ID Remarks Contact PersonDocument18 pagesCompany Name Address1 Address2 Area City Pincode Contact Number Designation Mobile URL Email ID Remarks Contact Personmurugesh18100% (1)
- Design of Buried Rigid Pipes: StandardsDocument26 pagesDesign of Buried Rigid Pipes: StandardsVarun VermaNo ratings yet
- IM 350F/430F/430Fb (D0AP/D0C4/D0C5-NA) Parts CatalogDocument101 pagesIM 350F/430F/430Fb (D0AP/D0C4/D0C5-NA) Parts CatalogDaniel S . ANo ratings yet
- Defining Your Idea, Product, And/Or Service (1) : Osong Fabrice MakiaDocument1 pageDefining Your Idea, Product, And/Or Service (1) : Osong Fabrice Makiangoufor atemafacNo ratings yet
- Itp For SanitaryDocument4 pagesItp For SanitaryDebesh Chaudhary100% (2)
- 2017 Rochester Business Hall of FameDocument24 pages2017 Rochester Business Hall of FameMichael DuntzNo ratings yet
- ElastomerDocument3 pagesElastomersiswoutNo ratings yet
- North South University: Assignment Cover Page Department of Public HealthDocument2 pagesNorth South University: Assignment Cover Page Department of Public HealthRupak IslamNo ratings yet