Download as pdf or txt
You might also like
- Essentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadDocument38 pagesEssentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadcarrielivingstonocifrtkgnyNo ratings yet
- Bjorn Lomborg - How To Spend $50 Billion To Make The World A Better Place (2006) PDFDocument207 pagesBjorn Lomborg - How To Spend $50 Billion To Make The World A Better Place (2006) PDFENRIQUE GARCIA GARCIA100% (5)
- Lesson Plan - A Caffeine Fueled WorldDocument5 pagesLesson Plan - A Caffeine Fueled WorldYaraCarobrez100% (1)
- Amniotic Fluid EmbolismDocument2 pagesAmniotic Fluid EmbolismMyk Twentytwenty NBeyondNo ratings yet
- Postpartum HemorrhageDocument21 pagesPostpartum HemorrhageCintya PradyanthiNo ratings yet
- Basic Life Support For Lay Rescuer: TitleDocument72 pagesBasic Life Support For Lay Rescuer: Titlekheyan2013100% (1)
- Amniotic Fluid EmbolismDocument13 pagesAmniotic Fluid EmbolismDrNorNo ratings yet
- Amniotic Fluid EmbolismDocument13 pagesAmniotic Fluid Embolismelfa riniNo ratings yet
- Aurelio - Afe PBLDocument26 pagesAurelio - Afe PBLLyca Mae AurelioNo ratings yet
- Amniotic FluidsDocument7 pagesAmniotic FluidsMazlina MaidinNo ratings yet
- Amniotic Fluid EmbolismDocument8 pagesAmniotic Fluid EmbolismArri KurniawanNo ratings yet
- Amniotic Fluid Embolism.: ReferencesDocument7 pagesAmniotic Fluid Embolism.: ReferencesRSIA UMMINo ratings yet
- Anaphylactoid Syndrome of Pregnancy: A Review of The Literature With Latest Management and Outcome DataDocument7 pagesAnaphylactoid Syndrome of Pregnancy: A Review of The Literature With Latest Management and Outcome DataMaheen EinestineNo ratings yet
- 398 - Amniotic Fluid EmbolismDocument8 pages398 - Amniotic Fluid EmbolismAggrawal AnilNo ratings yet
- Tinjauan Pustaka: DefinisiDocument19 pagesTinjauan Pustaka: DefinisiKhandar YosuaNo ratings yet
- Maternal Hemorrhage Br. J. Anaesth.-2009-WalfishDocument10 pagesMaternal Hemorrhage Br. J. Anaesth.-2009-WalfishWindy MentariiNo ratings yet
- Amniotic Fluid EmbolismDocument5 pagesAmniotic Fluid EmbolismDenim Embalzado MaghanoyNo ratings yet
- Hemorragia Intraparto PDFDocument12 pagesHemorragia Intraparto PDFana catalinaNo ratings yet
- Amniotic Fluid EmbolismDocument5 pagesAmniotic Fluid EmbolismRafael BagusNo ratings yet
- A Current Concept of EclampsiaDocument4 pagesA Current Concept of EclampsiadrheayNo ratings yet
- What Is Pulmonary Hypertension?: Right VentricleDocument10 pagesWhat Is Pulmonary Hypertension?: Right VentriclecharmieangelNo ratings yet
- Amniotic Fuid EmbolismDocument7 pagesAmniotic Fuid EmbolismNishaThakuriNo ratings yet
- Amniotic Fluid Embolism - UpToDateDocument39 pagesAmniotic Fluid Embolism - UpToDateCristinaCaprosNo ratings yet
- Amniotic Fluid Embolism ArticleDocument3 pagesAmniotic Fluid Embolism ArticleShailesh JainNo ratings yet
- Amniotic Fluid EmbolismDocument1 pageAmniotic Fluid EmbolismAnne VillanuevaNo ratings yet
- Amniotic Fluid EmbolismDocument4 pagesAmniotic Fluid Embolismmedicinaun74100% (1)
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloNo ratings yet
- Placenta As Witness 07Document15 pagesPlacenta As Witness 07Vetési OrsolyaNo ratings yet
- Joacp 32 153Document7 pagesJoacp 32 153thresh mainNo ratings yet
- Jouranl Emboli Cairan Ketuban1Document6 pagesJouranl Emboli Cairan Ketuban1Moh RamliNo ratings yet
- Antepartum and Postpartum Hemorrhage: Fitsum AshebirDocument64 pagesAntepartum and Postpartum Hemorrhage: Fitsum Ashebirzuzuyasi65No ratings yet
- 3rd Trimester Bleeding and Postpartum HemorrhageDocument100 pages3rd Trimester Bleeding and Postpartum Hemorrhagepeanutbutter ohNo ratings yet
- Complications of Pregnancy: Clinical Guidelines O MDocument12 pagesComplications of Pregnancy: Clinical Guidelines O MAlif FaqihNo ratings yet
- Antepartum Haemorrhage: ReviewDocument5 pagesAntepartum Haemorrhage: ReviewI_Ketut_Wahyu_MerthaNo ratings yet
- Guideline HipertensiDocument7 pagesGuideline HipertensiAgus RiyantoNo ratings yet
- Vaginalbleedinginlate Pregnancy: Janet S. Young,, Lindsey M. WhiteDocument14 pagesVaginalbleedinginlate Pregnancy: Janet S. Young,, Lindsey M. WhiteEka NataNo ratings yet
- Etiology, Clinical Manifestations, and Prediction of Placental AbruptionDocument9 pagesEtiology, Clinical Manifestations, and Prediction of Placental AbruptionKadije OanaNo ratings yet
- Postpartum Hemorrhage PDFDocument21 pagesPostpartum Hemorrhage PDFLillian HerreraNo ratings yet
- Amniotic FL Uid Embolism: Review ArticleDocument7 pagesAmniotic FL Uid Embolism: Review ArticleKinjal VasavaNo ratings yet
- Intrapartum HemorrhageDocument12 pagesIntrapartum HemorrhageLillian HerreraNo ratings yet
- Diagnosis and Management of Ectopic Pregnancy: Europe PMC Funders GroupDocument20 pagesDiagnosis and Management of Ectopic Pregnancy: Europe PMC Funders GroupDeby Nelsya Eka ZeinNo ratings yet
- Ulstermedj00194 0093 PDFDocument8 pagesUlstermedj00194 0093 PDFMohamed GeilNo ratings yet
- Amniotic Fluid Embolism: Irene Stafford, MD, Jeanne She Eld, MDDocument9 pagesAmniotic Fluid Embolism: Irene Stafford, MD, Jeanne She Eld, MDChristian JuarezNo ratings yet
- April Baylon2Document1 pageApril Baylon2April Love Baylon EndoNo ratings yet
- ACOG Committee Opinion No 348 Umbilical Cord Blood Gas and Acid-Base AnalysisDocument4 pagesACOG Committee Opinion No 348 Umbilical Cord Blood Gas and Acid-Base AnalysisLina E. Arango100% (1)
- Green Top Guidelines 11Document24 pagesGreen Top Guidelines 11garfield1No ratings yet
- Mcdonnell 2013Document8 pagesMcdonnell 2013Erlyn SevilleNo ratings yet
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- Postpartum HemorrhageDocument17 pagesPostpartum HemorrhageAdel GameliNo ratings yet
- Hemorrgia Obstetrica 2020Document20 pagesHemorrgia Obstetrica 2020Carolina VargasNo ratings yet
- New Aspects in The Pathophysiology of Preeclampsia: Clinical ScienceDocument27 pagesNew Aspects in The Pathophysiology of Preeclampsia: Clinical Sciencenaumee100% (2)
- Ngeh 2006Document5 pagesNgeh 2006ayu fitriaNo ratings yet
- Acta Obstet Gynecol Scand - 2011 - TIKKANENDocument9 pagesActa Obstet Gynecol Scand - 2011 - TIKKANENsawsanNo ratings yet
- Nejmra 1513247Document11 pagesNejmra 1513247Jose BoderoNo ratings yet
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaNo ratings yet
- Maternal Collapse During PregnancyDocument57 pagesMaternal Collapse During PregnancytapayanaNo ratings yet
- Amniotic Fluid EmbolismDocument8 pagesAmniotic Fluid EmbolismjNo ratings yet
- B41. Su-Et-Al PPH PDFDocument21 pagesB41. Su-Et-Al PPH PDFjhon heriansyahNo ratings yet
- GTG 56 PDFDocument24 pagesGTG 56 PDFKadelsy BristolNo ratings yet
- Urogenital Prolapse: Section A Prolapse and The Pelvic FloorDocument1 pageUrogenital Prolapse: Section A Prolapse and The Pelvic FloorarezqyfNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Wiley Journal APCs Open AccessDocument44 pagesWiley Journal APCs Open Accesstoyibatul hidayatiNo ratings yet
- Gene Transfer MethodsDocument41 pagesGene Transfer MethodsMayuriGulhane100% (1)
- CARDIO Intensive CareDocument6 pagesCARDIO Intensive CareDianne Erika MeguinesNo ratings yet
- Bio Medical Waste ManagementDocument48 pagesBio Medical Waste ManagementManu Raj Mathur100% (4)
- Actualizacion de La PreeclampsiaDocument8 pagesActualizacion de La PreeclampsiaPierina VeramatosNo ratings yet
- PNLE Community Health Nursing Exam 4Document9 pagesPNLE Community Health Nursing Exam 4Denisse PalayNo ratings yet
- 02/27/09 - The Stanford Daily (PDF)Document8 pages02/27/09 - The Stanford Daily (PDF)The Stanford DailyNo ratings yet
- Preventive Care: Female Checklist - UnitedHealthcareDocument3 pagesPreventive Care: Female Checklist - UnitedHealthcareLiz MNo ratings yet
- Republic v. Cagandahan, G.R. No. 166676, 12 September 2008Document1 pageRepublic v. Cagandahan, G.R. No. 166676, 12 September 2008Jovelan V. EscañoNo ratings yet
- 28-Abhishek TiwariDocument3 pages28-Abhishek TiwariAbhishek TiwariNo ratings yet
- Tension Pneumothorax PDFDocument2 pagesTension Pneumothorax PDFClarissa Aileen Caliva AdoraNo ratings yet
- Molluscum Contagiosum: Report of One Case With OverviewDocument3 pagesMolluscum Contagiosum: Report of One Case With Overviewevitri pasaribuNo ratings yet
- Doh Do 0223Document19 pagesDoh Do 0223J Velasco PeraltaNo ratings yet
- Bali BellyDocument3 pagesBali BellyAstri KarmilaNo ratings yet
- Sri LankaDocument4 pagesSri LankaJehan Somasiri JayathungaNo ratings yet
- Vascular DementiaDocument57 pagesVascular Dementiadrkadiyala2No ratings yet
- BloodlettingDocument5 pagesBloodlettingMaria Lana Grace DiazNo ratings yet
- Vital Sign #1: Body TemperatureDocument5 pagesVital Sign #1: Body TemperaturePrimelift Safety Resources LimitedNo ratings yet
- Caries Case StudyDocument19 pagesCaries Case Studyapi-279025476No ratings yet
- NIH Public Access: Growth and Laboratory Maintenance of PseudomonasDocument11 pagesNIH Public Access: Growth and Laboratory Maintenance of PseudomonasraveonNo ratings yet
- Primer For The Punctuation of Heart DiseaseDocument3 pagesPrimer For The Punctuation of Heart DiseaserespiraahoraNo ratings yet
- 28 NOVEMBER 2009 - 28 NOVEMBRE 2009: Belgian Equine Practitioners Society (BEPS)Document7 pages28 NOVEMBER 2009 - 28 NOVEMBRE 2009: Belgian Equine Practitioners Society (BEPS)Carlos Pedro VillaNo ratings yet
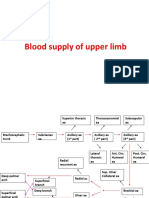
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- GASTRITISDocument11 pagesGASTRITISHemant SharmaNo ratings yet
- Nelec 2: Acute and Critical Care Nursing: Unit Learning OutcomeDocument4 pagesNelec 2: Acute and Critical Care Nursing: Unit Learning Outcomeyas minNo ratings yet
- Le Fort II Osteotomy and Modified Technique Presentation: Riginal RticleDocument6 pagesLe Fort II Osteotomy and Modified Technique Presentation: Riginal RticleSamuel SuazaNo ratings yet