Download as pdf or txt
You might also like
- Yi Jin Jing-Yi Gun Gin 12 ExercisesDocument12 pagesYi Jin Jing-Yi Gun Gin 12 ExercisesMateo Lunden100% (1)
- Ovarian Cancer Paper Final Version 4Document9 pagesOvarian Cancer Paper Final Version 4api-241216897No ratings yet
- 2anatomy of The Inguinal RegionDocument47 pages2anatomy of The Inguinal Regionthowell3No ratings yet
- Prostate Cancer Research PaperDocument12 pagesProstate Cancer Research PapershaunNo ratings yet
- Cancer Screening: Dr. Waqar MunirDocument26 pagesCancer Screening: Dr. Waqar MunirWaqar MunirNo ratings yet
- Progressive Prostate Cancer, Biochemically DefinedDocument9 pagesProgressive Prostate Cancer, Biochemically DefinedchrisjoyfulNo ratings yet
- APJCP Volume 15 Issue 22 Pages 9575-9578Document4 pagesAPJCP Volume 15 Issue 22 Pages 9575-9578DoyoxNo ratings yet
- Prostate Cancer: Signs and SymptomsDocument5 pagesProstate Cancer: Signs and SymptomsLicio LentimoNo ratings yet
- Prostate NeoplasmsDocument45 pagesProstate NeoplasmsJoe KhdeirNo ratings yet
- Prostate EMEDICINEDocument14 pagesProstate EMEDICINESan Phạm ĐìnhNo ratings yet
- Prostate Cancer PSADocument5 pagesProstate Cancer PSAvictoria martin zaccariaNo ratings yet
- AssessmentDocument5 pagesAssessmentshujin_sama100% (2)
- Prostate Cancer Screening and The Associated ControversyDocument17 pagesProstate Cancer Screening and The Associated ControversyBolivar IseaNo ratings yet
- Liver, Gallbladder, and Biliary Tract Cancers: Hepatocellular CancerDocument20 pagesLiver, Gallbladder, and Biliary Tract Cancers: Hepatocellular CancerEdgarem28No ratings yet
- The Dilemmas of Prostate CancerDocument8 pagesThe Dilemmas of Prostate CancerAugusto MilanezNo ratings yet
- Artículo Inglés Cáncer de PróstataDocument10 pagesArtículo Inglés Cáncer de PróstataAxel ColmeneroNo ratings yet
- Arc PSA PDFDocument17 pagesArc PSA PDFBharat KumarNo ratings yet
- Prostate Cancer Between Prognosis and Adequate/proper TherapyDocument8 pagesProstate Cancer Between Prognosis and Adequate/proper TherapyGabriel NguyenNo ratings yet
- Prostate CancerDocument45 pagesProstate CancerNeethiselvam Devadoss100% (2)
- Nej MCP 2209151Document10 pagesNej MCP 2209151Dario TaimalNo ratings yet
- Colorectal Cancer Screening English 2007 PDFDocument18 pagesColorectal Cancer Screening English 2007 PDFtanjudinNo ratings yet
- Prostate Cancer Research PapersDocument5 pagesProstate Cancer Research Papersyscgudvnd100% (1)
- Clinical Presentation and Diagnosis of Prostate CáncerDocument5 pagesClinical Presentation and Diagnosis of Prostate CáncermanuelNo ratings yet
- Prostate Cancer, 2nd Ed. by Anne KatzDocument317 pagesProstate Cancer, 2nd Ed. by Anne Katzkrisz.vorosNo ratings yet
- Twelve Major Cancers: Fact SheetDocument7 pagesTwelve Major Cancers: Fact SheetSCRUPEUSSNo ratings yet
- Prostate Cancer FinalDocument20 pagesProstate Cancer FinalKim Gonzales100% (3)
- Prostate CancerDocument67 pagesProstate CancerMalueth AnguiNo ratings yet
- An Introduction To: Prostate CancerDocument8 pagesAn Introduction To: Prostate Cancerkw21167No ratings yet
- Urogenital CancersDocument2 pagesUrogenital CancerssdfNo ratings yet
- Final Prostate CancerDocument6 pagesFinal Prostate CancerJerryboy69No ratings yet
- Prostate Cancer Screening, Diagnosis and Risk Stratification - Oncology - Adult - Urology Core CurriculumDocument31 pagesProstate Cancer Screening, Diagnosis and Risk Stratification - Oncology - Adult - Urology Core CurriculumMarco Túlio La Guardia PiresNo ratings yet
- Prostate Cancer Treatment in India Detailed InformationDocument3 pagesProstate Cancer Treatment in India Detailed InformationinadorNo ratings yet
- Active Surveillance For Prostate Cancer AUA Update 33 2008Document8 pagesActive Surveillance For Prostate Cancer AUA Update 33 2008moetazNo ratings yet
- Assignmnet LondonDocument16 pagesAssignmnet LondonRikenkumar BariaNo ratings yet
- Prognostic Value of Serum Markers For PRDocument18 pagesPrognostic Value of Serum Markers For PRDrAbhishek SoniNo ratings yet
- Prostate Cancer in TripuraDocument13 pagesProstate Cancer in TripuraSnehendu BhowmikNo ratings yet
- Prostate Cancer Research by Ahmed RoushdyDocument20 pagesProstate Cancer Research by Ahmed RoushdyAhmed RoushdyNo ratings yet
- Prostate CancerDocument10 pagesProstate Canceraji20No ratings yet
- Rostate Ancer: Jill M. KolesarDocument14 pagesRostate Ancer: Jill M. KolesarbencleeseNo ratings yet
- Dissertation On Prostate CancerDocument24 pagesDissertation On Prostate CancerZainab ShahidNo ratings yet
- Cancerul de ProstataDocument19 pagesCancerul de ProstataTiperciuc BrindusaNo ratings yet
- Epidemiology of Prostate Cancer: ReviewDocument27 pagesEpidemiology of Prostate Cancer: ReviewSurya MaruxNo ratings yet
- Principles of Oncology and Outline of ManagementDocument78 pagesPrinciples of Oncology and Outline of ManagementPavan JonnadaNo ratings yet
- Cancer de Próstata (Screening) 2011Document7 pagesCancer de Próstata (Screening) 2011Nadia CmNo ratings yet
- Cancer CareDocument84 pagesCancer Careakoeljames8543No ratings yet
- 359-Book Chapter-4007-1-10-20210526Document12 pages359-Book Chapter-4007-1-10-20210526Melinda Novy RamadhaniNo ratings yet
- IT 27 - Rujukan Pada Doga - EMDocument19 pagesIT 27 - Rujukan Pada Doga - EMRurie Awalia SuhardiNo ratings yet
- Case Study On Prostatic CancerDocument21 pagesCase Study On Prostatic CancerJai - Ho100% (3)
- Screening For Prostate CancerDocument16 pagesScreening For Prostate CancerGabriel NguyenNo ratings yet
- Cancer Screening Guidelines: Prepared By: DR. Hanan AbbasDocument35 pagesCancer Screening Guidelines: Prepared By: DR. Hanan AbbashanfmhananfmhanNo ratings yet
- Assignment of Prostate Cancer by Adel Khalil PDFDocument18 pagesAssignment of Prostate Cancer by Adel Khalil PDFعادل خليلNo ratings yet
- Colon CancerDocument25 pagesColon Cancerchori2008No ratings yet
- Thyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e RDocument7 pagesThyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e REndang Rahayu Fuji LestaryNo ratings yet
- Lifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDocument10 pagesLifestyle and Dietary Factors in The Prevention of Lethal Prostate CancerDale MckinneyNo ratings yet
- Prostate Cancer: What You Need To KnowDocument2 pagesProstate Cancer: What You Need To KnowMedlabs - Sehtak Bil DeniaNo ratings yet
- Ovarian Cancer - StatPearls - NCBI BookshelfDocument13 pagesOvarian Cancer - StatPearls - NCBI BookshelfeeeeeeNo ratings yet
- Prostate CancerDocument58 pagesProstate CancerIsaac MwangiNo ratings yet
- Colorectal Cancer Research PaperDocument10 pagesColorectal Cancer Research PapershaunNo ratings yet
- Prostate cancerPRIMERDocument27 pagesProstate cancerPRIMERLuan MarcosNo ratings yet
- How to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthFrom EverandHow to Prevent Prostate Problems: A Complete Guide to the Essentials of Prostate HealthNo ratings yet
- 461 Full PDFDocument8 pages461 Full PDFCarlos MichasNo ratings yet
- 10 1016@j Paed 2020 06 003 PDFDocument5 pages10 1016@j Paed 2020 06 003 PDFCarlos MichasNo ratings yet
- Parkinson's Disease: EpidemiologyDocument6 pagesParkinson's Disease: EpidemiologyCarlos MichasNo ratings yet
- Small BowelDocument7 pagesSmall BowelCarlos MichasNo ratings yet
- Anemia y Tracto GiDocument5 pagesAnemia y Tracto GiCarlos MichasNo ratings yet
- Cancer Pulmonar EstadiajeDocument8 pagesCancer Pulmonar EstadiajeCarlos MichasNo ratings yet
- Colitis UlcerrosaDocument5 pagesColitis UlcerrosaCarlos MichasNo ratings yet
- Genentech Internship Journal E-PortfolioDocument5 pagesGenentech Internship Journal E-Portfolioapi-317145308No ratings yet
- AssignmentDocument3 pagesAssignmentJam Sohail Ahmed DaharNo ratings yet
- Schematic Diagram of RabiesDocument1 pageSchematic Diagram of RabiesMykie Pearl Gamulo CabuyadaoNo ratings yet
- Relationship of Long Operation With Shivering Events in Post Spinal Anesthetic Patient at Rsud Leuwiliang Bogor RegencyDocument10 pagesRelationship of Long Operation With Shivering Events in Post Spinal Anesthetic Patient at Rsud Leuwiliang Bogor RegencySalim RumraNo ratings yet
- Acute Appendicitis in Adults ManagementDocument16 pagesAcute Appendicitis in Adults ManagementPriscila Tobar AlcántarNo ratings yet
- MMW MedicationDocument2 pagesMMW MedicationammarNo ratings yet
- ScriptDocument6 pagesScriptapi-298505323No ratings yet
- Family Medicine Concept and Patient ManagementDocument36 pagesFamily Medicine Concept and Patient ManagementSapta YudhaNo ratings yet
- Links Library Find Out If You WonDocument10 pagesLinks Library Find Out If You WonusmleNo ratings yet
- Madness and Politics: The Case of James Forrestal: Mary Akashah and Donald TennantDocument4 pagesMadness and Politics: The Case of James Forrestal: Mary Akashah and Donald TennantRobin TobarNo ratings yet
- 2009 A Critical Review of AuscultatingDocument6 pages2009 A Critical Review of AuscultatingaubinloNo ratings yet
- E Book HandstandDocument8 pagesE Book HandstandBorislav Georgiev100% (1)
- Antibiotic Sensitivity FINAL V4 Sheet1Document1 pageAntibiotic Sensitivity FINAL V4 Sheet1JHNo ratings yet
- Symptoms of Esophageal DiseaseDocument33 pagesSymptoms of Esophageal DiseaseRakesh PathrabeNo ratings yet
- Agrobuchtal-Baseino Projektai 2Document38 pagesAgrobuchtal-Baseino Projektai 2andravalentinaNo ratings yet
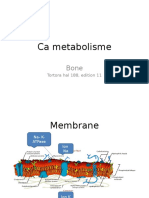
- Ca Metabolisme: Tortora Hal 188, Edition 11Document21 pagesCa Metabolisme: Tortora Hal 188, Edition 11Julian HuningkorNo ratings yet
- Sleep Like The Dead by Alex Gray - Chapter OneDocument22 pagesSleep Like The Dead by Alex Gray - Chapter OneLittle Brown UK0% (1)
- New PDF For PharmacologyDocument236 pagesNew PDF For PharmacologyDIPENDRA KUMAR KUSHAWAHA100% (1)
- Sensory Dysfunction & AutismDocument15 pagesSensory Dysfunction & AutismDiana DanciuNo ratings yet
- Hirsch SprungDocument3 pagesHirsch SprungBheru LalNo ratings yet
- MS CA and EN Ans KeyDocument15 pagesMS CA and EN Ans KeyAydh Dim-Mac RsclNo ratings yet
- Trauma Saraf SpinalDocument41 pagesTrauma Saraf SpinalFatahillah NazarNo ratings yet
- Revised Syllabus VLDD 2022-23Document18 pagesRevised Syllabus VLDD 2022-23Critical ThinkerNo ratings yet
- VitaminsDocument2 pagesVitaminsMDreamerNo ratings yet
- PRINTABLE APOTHECARY LABELS Healing HerbsDocument8 pagesPRINTABLE APOTHECARY LABELS Healing HerbsJES100% (4)
- GAD 7 Anxiety Updated 0Document1 pageGAD 7 Anxiety Updated 0Shintya DewiNo ratings yet
- Antigens ClassDocument61 pagesAntigens ClassKoushali BanerjeeNo ratings yet