Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 1 The Basics 1Document19 pages1 The Basics 11202blackNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Roadmap: A2 Achievement Test 2 (Units 3-4)Document4 pagesRoadmap: A2 Achievement Test 2 (Units 3-4)Nicolás MartínezNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1 Copyreading and Headline WritingDocument72 pages1 Copyreading and Headline WritingAdrian Yan Yan Delara100% (2)
- Membertou Family Homes Law Fact SheetDocument2 pagesMembertou Family Homes Law Fact SheetfiseradaNo ratings yet
- Cahn&Polich - 06 Meditation States and Traits ReviewDocument33 pagesCahn&Polich - 06 Meditation States and Traits ReviewfiseradaNo ratings yet
- Cultural Sensitivity and Adaptation in Family Based Prevention InterventionsDocument6 pagesCultural Sensitivity and Adaptation in Family Based Prevention Interventionsfiserada100% (1)
- Tsung-Mi and The Single Word "Awareness" (Chih) by Peter GregoryDocument20 pagesTsung-Mi and The Single Word "Awareness" (Chih) by Peter GregoryfiseradaNo ratings yet
- Shojin Ryori Culinary Fundamentals in Zen PDFDocument1 pageShojin Ryori Culinary Fundamentals in Zen PDFfiseradaNo ratings yet
- Qualitative PerspectivesDocument8 pagesQualitative PerspectivesfiseradaNo ratings yet
- Diagnostic Systematic Reviews Road Map V3Document2 pagesDiagnostic Systematic Reviews Road Map V3fiseradaNo ratings yet
- Large SystemsDocument220 pagesLarge SystemsfiseradaNo ratings yet
- Innovation in Instrument DesignDocument28 pagesInnovation in Instrument DesignfiseradaNo ratings yet
- How Far Can Q-Analysis Go Into Social Systems Understanding ?Document10 pagesHow Far Can Q-Analysis Go Into Social Systems Understanding ?fiseradaNo ratings yet
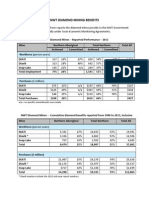
- NWT Diamond Mining Benefits: N/a - No Specific Commitments Were MadeDocument2 pagesNWT Diamond Mining Benefits: N/a - No Specific Commitments Were MadefiseradaNo ratings yet
- Making Outcome Mapping WorkDocument79 pagesMaking Outcome Mapping WorkfiseradaNo ratings yet
- Biblical Hebrew A Text and WorkbookDocument451 pagesBiblical Hebrew A Text and Workbookannegh100% (4)
- Diavik Fact BookDocument20 pagesDiavik Fact BookfiseradaNo ratings yet
- Economic Resilience To DisastersDocument59 pagesEconomic Resilience To DisastersfiseradaNo ratings yet
- Embragues y Frenos - P-1960-CDocument4 pagesEmbragues y Frenos - P-1960-Cdéborah_rosalesNo ratings yet
- Belgas R627 IOMDocument6 pagesBelgas R627 IOMSMcNo ratings yet
- Transducers & Isolators: TR - IsoDocument1 pageTransducers & Isolators: TR - IsoManikandan B100% (1)
- The 73rd Constitutional Amendment ActDocument26 pagesThe 73rd Constitutional Amendment ActYasser ArfatNo ratings yet
- CH 01 Wooldridge 5e PPTDocument23 pagesCH 01 Wooldridge 5e PPTKrithiga Soundrajan100% (1)
- Illustrated Spare Part List FOR: Kirloskar Oil Engines LimitedDocument61 pagesIllustrated Spare Part List FOR: Kirloskar Oil Engines LimitedDarshan MakwanaNo ratings yet
- VIR - Reform in TelecommunicationsDocument10 pagesVIR - Reform in TelecommunicationsNgu HoangNo ratings yet
- Knowledge, Creativity and Communication in Education: Multimodal DesignDocument11 pagesKnowledge, Creativity and Communication in Education: Multimodal DesignMartín VillagraNo ratings yet
- DM No. 149 S. 2023 Addendum To Division Memorandum No. 412 S. 2022Document14 pagesDM No. 149 S. 2023 Addendum To Division Memorandum No. 412 S. 2022Jessa GeronNo ratings yet
- BIG ASS FAN Element CustomerDocument10 pagesBIG ASS FAN Element CustomerJesus David Muñoz RoblesNo ratings yet
- Paint Data Sheet - National Synthetic Enamel Gloss IDocument3 pagesPaint Data Sheet - National Synthetic Enamel Gloss Iaakh0% (1)
- 08-01-17 EditionDocument28 pages08-01-17 EditionSan Mateo Daily JournalNo ratings yet
- MP 87.1-2008 Australian New Zealand Certification Scheme For Explosion-Protected Electrical Equipment (ANZExDocument6 pagesMP 87.1-2008 Australian New Zealand Certification Scheme For Explosion-Protected Electrical Equipment (ANZExSAI Global - APACNo ratings yet
- Final INTERNSHIP Report-AshishDocument66 pagesFinal INTERNSHIP Report-AshishAshish PantNo ratings yet
- Judi Online Di MedsosDocument11 pagesJudi Online Di MedsosHabibah HabibahNo ratings yet
- A Stingless Bee Hive Design For A Broader ClimateDocument4 pagesA Stingless Bee Hive Design For A Broader ClimateMarlon Manaya Garrigues100% (1)
- Servicemanual Panasonic kv-s5046h 5076h s3Document17 pagesServicemanual Panasonic kv-s5046h 5076h s3Ralf KöhlerNo ratings yet
- Azolla: A Review of Its Biology and UtilizationDocument6 pagesAzolla: A Review of Its Biology and UtilizationAaron PabionaNo ratings yet
- Terraria Official Lore PDFDocument3 pagesTerraria Official Lore PDFCavalo SebosoNo ratings yet
- Server Poweredge t610 Tech Guidebook PDFDocument65 pagesServer Poweredge t610 Tech Guidebook PDFMarouani AmorNo ratings yet
- Periodontal Ligament-SummerDocument24 pagesPeriodontal Ligament-Summerapi-3775747100% (1)
- Wabco Twin-Cylinder Air Dryer: Description / MaintenanceDocument12 pagesWabco Twin-Cylinder Air Dryer: Description / MaintenanceAlanNo ratings yet
- Courseplay English User ManualDocument12 pagesCourseplay English User ManualCelticgirlNo ratings yet
- Cassegrain Telescope: Presented by Mehar 12CDocument10 pagesCassegrain Telescope: Presented by Mehar 12CMehar FathimaNo ratings yet
- Factoring HandoutDocument2 pagesFactoring HandoutJordan SenkoNo ratings yet
- Filtrec F040 SeriesDocument8 pagesFiltrec F040 Serieshkhan10No ratings yet
- Building Construction and Materials Report: Curtain Wall Building Type Building Name: Seagrams BuildingDocument6 pagesBuilding Construction and Materials Report: Curtain Wall Building Type Building Name: Seagrams BuildingAyushi AroraNo ratings yet