
Pandemic H1N1 2009 Influenza: Clinical Management Guidelines For Pregnancy
Pandemic H1N1 2009 Influenza: Clinical Management Guidelines For Pregnancy
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BHU Daily Stock PerformaDocument6 pagesBHU Daily Stock PerformabilalNo ratings yet
- PCS Questions and AnswersDocument26 pagesPCS Questions and Answerszuhaib86% (7)
- Continuous and Extended Infusion Beta Lactams PDFDocument3 pagesContinuous and Extended Infusion Beta Lactams PDFarnaldops333No ratings yet
- Notes On Microbiology - BiologyDocument83 pagesNotes On Microbiology - BiologyRajaDeepak VermaNo ratings yet
- What Are AntibioticsDocument31 pagesWhat Are Antibiotics1211988610No ratings yet
- Management Report 2012Document41 pagesManagement Report 2012Daniela AlimanNo ratings yet
- Endodontic Emergencies / Orthodontic Courses by Indian Dental AcademyDocument31 pagesEndodontic Emergencies / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
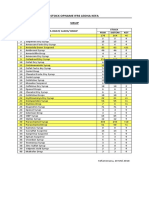
- Stock Opname Ifrs Leona Kefa Sirup: NO Nama Obat/ Alkes/ BMHP Stock Fisik Sistem KETDocument1 pageStock Opname Ifrs Leona Kefa Sirup: NO Nama Obat/ Alkes/ BMHP Stock Fisik Sistem KETAnonymous 4q7DzSENo ratings yet
- 5th European Conference On Marine Natural ProductsDocument224 pages5th European Conference On Marine Natural ProductsrlegarNo ratings yet
- Are Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiDocument6 pagesAre Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiRadia LachehebNo ratings yet
- Sulfonamides: PHRM 304: Antibiotics and Chemotherapeutic AgentsDocument36 pagesSulfonamides: PHRM 304: Antibiotics and Chemotherapeutic AgentsApurba Sarker Apu100% (2)
- Revision Test of Chapter 1 ScienceDocument4 pagesRevision Test of Chapter 1 ScienceYasoktaran AnanthanNo ratings yet
- Extended Spectrum PenicillinsDocument80 pagesExtended Spectrum PenicillinsSunanda mohanNo ratings yet
- Units Essential For Maintaining Cell Integrity Prevention ofDocument2 pagesUnits Essential For Maintaining Cell Integrity Prevention ofJayde TabanaoNo ratings yet
- Ppra Ab Terapi PDFDocument83 pagesPpra Ab Terapi PDFDIONYSIUS BENINo ratings yet
- Penicilina: Alexander FlemingDocument5 pagesPenicilina: Alexander FlemingKath Bravo GonzálezNo ratings yet
- Antibacterial and Antibiofilm Potential of Ethanolic Extract From Bintaro Flower (Cerbera Odollam) Against StaphylococcusDocument4 pagesAntibacterial and Antibiofilm Potential of Ethanolic Extract From Bintaro Flower (Cerbera Odollam) Against Staphylococcusdwisl95No ratings yet
- UTI Algorithm-Inpatient RQHRDocument1 pageUTI Algorithm-Inpatient RQHRDe RadianNo ratings yet
- Empiric IV RX CAP Children - UpToDateDocument3 pagesEmpiric IV RX CAP Children - UpToDateMagda Mariana Medina100% (1)
- Infección Urinaria - UpToDateDocument29 pagesInfección Urinaria - UpToDateDeivid Ruidiazz GmezzNo ratings yet
- CephalosporinDocument8 pagesCephalosporinvidagurlNo ratings yet
- USP Veterinary Clinical Drug Information Monograph Development ProcessDocument6 pagesUSP Veterinary Clinical Drug Information Monograph Development ProcessKelma TayebaNo ratings yet
- Brevibacterium LengkapDocument23 pagesBrevibacterium LengkapanggaririnNo ratings yet
- Note Antibacterial Activity of Medicinal Plants From The PhilippinesDocument4 pagesNote Antibacterial Activity of Medicinal Plants From The PhilippinesRey TantiadoNo ratings yet
- DFSV - (TIN) Antibiotic Detection LimitsDocument2 pagesDFSV - (TIN) Antibiotic Detection LimitsChevronelleNo ratings yet
- Ai AssignmentDocument24 pagesAi AssignmentskmitunNo ratings yet
- MGO Manuka HoneyDocument1 pageMGO Manuka Honeyromi-kunNo ratings yet
- Print Antibiotics ReviewDocument6 pagesPrint Antibiotics ReviewtiuwangNo ratings yet
- 41 Symplocos Racemosa - MonographDocument9 pages41 Symplocos Racemosa - MonographMSKCNo ratings yet
- Antimicrobial Properties of Allicin From GarlicDocument3 pagesAntimicrobial Properties of Allicin From GarlicEdward Kenneth DragasNo ratings yet





































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BHU Daily Stock PerformaDocument6 pagesBHU Daily Stock PerformabilalNo ratings yet
- PCS Questions and AnswersDocument26 pagesPCS Questions and Answerszuhaib86% (7)
- Continuous and Extended Infusion Beta Lactams PDFDocument3 pagesContinuous and Extended Infusion Beta Lactams PDFarnaldops333No ratings yet
- Notes On Microbiology - BiologyDocument83 pagesNotes On Microbiology - BiologyRajaDeepak VermaNo ratings yet
- What Are AntibioticsDocument31 pagesWhat Are Antibiotics1211988610No ratings yet
- Management Report 2012Document41 pagesManagement Report 2012Daniela AlimanNo ratings yet
- Endodontic Emergencies / Orthodontic Courses by Indian Dental AcademyDocument31 pagesEndodontic Emergencies / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Stock Opname Ifrs Leona Kefa Sirup: NO Nama Obat/ Alkes/ BMHP Stock Fisik Sistem KETDocument1 pageStock Opname Ifrs Leona Kefa Sirup: NO Nama Obat/ Alkes/ BMHP Stock Fisik Sistem KETAnonymous 4q7DzSENo ratings yet
- 5th European Conference On Marine Natural ProductsDocument224 pages5th European Conference On Marine Natural ProductsrlegarNo ratings yet
- Are Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiDocument6 pagesAre Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiRadia LachehebNo ratings yet
- Sulfonamides: PHRM 304: Antibiotics and Chemotherapeutic AgentsDocument36 pagesSulfonamides: PHRM 304: Antibiotics and Chemotherapeutic AgentsApurba Sarker Apu100% (2)
- Revision Test of Chapter 1 ScienceDocument4 pagesRevision Test of Chapter 1 ScienceYasoktaran AnanthanNo ratings yet
- Extended Spectrum PenicillinsDocument80 pagesExtended Spectrum PenicillinsSunanda mohanNo ratings yet
- Units Essential For Maintaining Cell Integrity Prevention ofDocument2 pagesUnits Essential For Maintaining Cell Integrity Prevention ofJayde TabanaoNo ratings yet
- Ppra Ab Terapi PDFDocument83 pagesPpra Ab Terapi PDFDIONYSIUS BENINo ratings yet
- Penicilina: Alexander FlemingDocument5 pagesPenicilina: Alexander FlemingKath Bravo GonzálezNo ratings yet
- Antibacterial and Antibiofilm Potential of Ethanolic Extract From Bintaro Flower (Cerbera Odollam) Against StaphylococcusDocument4 pagesAntibacterial and Antibiofilm Potential of Ethanolic Extract From Bintaro Flower (Cerbera Odollam) Against Staphylococcusdwisl95No ratings yet
- UTI Algorithm-Inpatient RQHRDocument1 pageUTI Algorithm-Inpatient RQHRDe RadianNo ratings yet
- Empiric IV RX CAP Children - UpToDateDocument3 pagesEmpiric IV RX CAP Children - UpToDateMagda Mariana Medina100% (1)
- Infección Urinaria - UpToDateDocument29 pagesInfección Urinaria - UpToDateDeivid Ruidiazz GmezzNo ratings yet
- CephalosporinDocument8 pagesCephalosporinvidagurlNo ratings yet
- USP Veterinary Clinical Drug Information Monograph Development ProcessDocument6 pagesUSP Veterinary Clinical Drug Information Monograph Development ProcessKelma TayebaNo ratings yet
- Brevibacterium LengkapDocument23 pagesBrevibacterium LengkapanggaririnNo ratings yet
- Note Antibacterial Activity of Medicinal Plants From The PhilippinesDocument4 pagesNote Antibacterial Activity of Medicinal Plants From The PhilippinesRey TantiadoNo ratings yet
- DFSV - (TIN) Antibiotic Detection LimitsDocument2 pagesDFSV - (TIN) Antibiotic Detection LimitsChevronelleNo ratings yet
- Ai AssignmentDocument24 pagesAi AssignmentskmitunNo ratings yet
- MGO Manuka HoneyDocument1 pageMGO Manuka Honeyromi-kunNo ratings yet
- Print Antibiotics ReviewDocument6 pagesPrint Antibiotics ReviewtiuwangNo ratings yet
- 41 Symplocos Racemosa - MonographDocument9 pages41 Symplocos Racemosa - MonographMSKCNo ratings yet
- Antimicrobial Properties of Allicin From GarlicDocument3 pagesAntimicrobial Properties of Allicin From GarlicEdward Kenneth DragasNo ratings yet