Download as pdf or txt
You might also like
- Pasig RiverDocument34 pagesPasig RiverNhilo ReginoNo ratings yet
- Pi Is 0923753420360798Document16 pagesPi Is 0923753420360798ekanovicaNo ratings yet
- Dinosaurs Before DarkDocument9 pagesDinosaurs Before DarkIna SimacheNo ratings yet
- Plasma Cell Myeloma Literature Review and Case StudyDocument6 pagesPlasma Cell Myeloma Literature Review and Case StudyafdtygyhkNo ratings yet
- Prognostic Factors in Acute Myeloid Leukaemia 4: Bob LoèwenbergDocument11 pagesPrognostic Factors in Acute Myeloid Leukaemia 4: Bob LoèwenbergStephania SandovalNo ratings yet
- 2008 Article 25Document8 pages2008 Article 25Firda PotterNo ratings yet
- Flowcytometryin Diagnosis, Prognostication, Andmonitoringofmultiple MyelomaandrelateddisordersDocument13 pagesFlowcytometryin Diagnosis, Prognostication, Andmonitoringofmultiple MyelomaandrelateddisordersmatanhibNo ratings yet
- Case Study. Aml - IntroDocument44 pagesCase Study. Aml - IntroDice BautistaNo ratings yet
- Myeloid LeukemiaDocument36 pagesMyeloid LeukemiaLia pramitaNo ratings yet
- 10 Use of Flow Cytometry in Clonal Plasma Cell DisordersDocument7 pages10 Use of Flow Cytometry in Clonal Plasma Cell DisorderscandiddreamsNo ratings yet
- Classification of Adult Acute Myeloid LeukemiaDocument24 pagesClassification of Adult Acute Myeloid LeukemiaSusianna RismandaNo ratings yet
- Advances in The Pathologic Diagnosis and Biology of Acute Myeloid LeukemiaDocument27 pagesAdvances in The Pathologic Diagnosis and Biology of Acute Myeloid LeukemiaRmt JosephNo ratings yet
- Myeloid Leukemia: DR Budi Enoch SPPDDocument36 pagesMyeloid Leukemia: DR Budi Enoch SPPDRoby KieranNo ratings yet
- Pages 4 7Document4 pagesPages 4 7andreas_251650No ratings yet
- Acute Myeloid Leukemia in Children and Adolescents - UpToDateDocument33 pagesAcute Myeloid Leukemia in Children and Adolescents - UpToDateainihanifiah100% (1)
- MM Bladè 2010Document7 pagesMM Bladè 2010Tommaso CaravitaNo ratings yet
- BR J Haematol - 2020 - Patel - Distinctive and Common Features of Moderate Aplastic AnaemiaDocument9 pagesBR J Haematol - 2020 - Patel - Distinctive and Common Features of Moderate Aplastic AnaemiaMarcellia AngelinaNo ratings yet
- A Triumvirate Correlating Thyroid Cytopathology Mole 2023 Surgical PatholDocument14 pagesA Triumvirate Correlating Thyroid Cytopathology Mole 2023 Surgical PatholrubenmacaNo ratings yet
- Acute Myeloid Leukemia A Concise ReviewDocument17 pagesAcute Myeloid Leukemia A Concise Reviewberlianza activiraNo ratings yet
- Penyebab Hepatomegali Pada AmlDocument6 pagesPenyebab Hepatomegali Pada AmlErawati ArmayaniNo ratings yet
- Acute Megakaryocytic Leukemia (Fab M7) : AbstractDocument4 pagesAcute Megakaryocytic Leukemia (Fab M7) : AbstractIrmagian PaleonNo ratings yet
- 10 1016@j CLL 2017 07 003 PDFDocument17 pages10 1016@j CLL 2017 07 003 PDFpiero317No ratings yet
- New England Journal Medicine: The ofDocument16 pagesNew England Journal Medicine: The ofMauricio FemeníaNo ratings yet
- Leukaemia Section: Refractory Anemia (RA)Document2 pagesLeukaemia Section: Refractory Anemia (RA)Devi Christina Damanik (Papua medical School)No ratings yet
- Article 2Document5 pagesArticle 2Mahadev HaraniNo ratings yet
- Acute Myeloid Leukemia With Myelodysplasia RelatedDocument6 pagesAcute Myeloid Leukemia With Myelodysplasia RelatedAgus WiniNo ratings yet
- Acute Myeloid LeukemiaDocument26 pagesAcute Myeloid Leukemiajustified13No ratings yet
- Myelodysplastic Syndromes: Diagnosis, Prognosis, and TreatmentDocument11 pagesMyelodysplastic Syndromes: Diagnosis, Prognosis, and TreatmentTataNo ratings yet
- Bacher 2005Document7 pagesBacher 2005Josué Cristhian Del Valle HornaNo ratings yet
- Estey-2018-American Journal of HematologyDocument25 pagesEstey-2018-American Journal of Hematologysury listinNo ratings yet
- Chronic Lymphocytic Leukemia: A Clinical and Molecular Heterogenous DiseaseDocument14 pagesChronic Lymphocytic Leukemia: A Clinical and Molecular Heterogenous DiseaseCallisthenisLeventisNo ratings yet
- Management of Acute LeukemiaDocument11 pagesManagement of Acute LeukemiaNicoletta ColomboNo ratings yet
- Blood Research: Diagnosis and Treatment of Chronic Myelomonocytic LeukemiaDocument12 pagesBlood Research: Diagnosis and Treatment of Chronic Myelomonocytic LeukemiaFilzah Anisa MayariNo ratings yet
- Acute - Myeloid - Leukemia - (AML) - W (Jurnal HEMA)Document9 pagesAcute - Myeloid - Leukemia - (AML) - W (Jurnal HEMA)nadaNo ratings yet
- Laboratory Diagnosis of ThalassemiaDocument9 pagesLaboratory Diagnosis of Thalassemiareza rivaldy azaNo ratings yet
- CSF3R 4Document7 pagesCSF3R 4AndikhaNo ratings yet
- Multiple Myeloma ESMO Clinical Practice GuidelinesDocument5 pagesMultiple Myeloma ESMO Clinical Practice GuidelinesFlaKitaNo ratings yet
- Review Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionDocument8 pagesReview Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionCat NhanNo ratings yet
- Genomics of Myelodysplastic Syndrome:myeloproliferative Neoplasm Overlap SyndromesDocument10 pagesGenomics of Myelodysplastic Syndrome:myeloproliferative Neoplasm Overlap Syndromesnutnut29No ratings yet
- Blood 1997 Jennings 2863 92Document31 pagesBlood 1997 Jennings 2863 92Neo Mervyn MonahengNo ratings yet
- Amlreview PDFDocument12 pagesAmlreview PDFMitaNo ratings yet
- American J Hematol - 2023 - Cheah-2Document14 pagesAmerican J Hematol - 2023 - Cheah-2salman mehriNo ratings yet
- Plasma Cell LeukemiaDocument18 pagesPlasma Cell LeukemiaMaria Carolina CoutoNo ratings yet
- Acute Leukemia HerfindalDocument35 pagesAcute Leukemia HerfindalAanshi ShahNo ratings yet
- Acute Myeloid Leukemia Research PaperDocument5 pagesAcute Myeloid Leukemia Research Paperafeartslf100% (1)
- Ijms 19 03492Document33 pagesIjms 19 03492Qaasim DramatNo ratings yet
- Acute Myeloid Leukemia ThesisDocument5 pagesAcute Myeloid Leukemia ThesisBuyCheapEssayOmaha100% (2)
- Chabot Richards2014 PDFDocument10 pagesChabot Richards2014 PDFGabriel MouraNo ratings yet
- Who Classification of The LAMDocument11 pagesWho Classification of The LAMAyoub HajjarNo ratings yet
- Mantle Cell LymphomaDocument8 pagesMantle Cell LymphomagauravsinghalNo ratings yet
- Kriteria Remisi AmlDocument6 pagesKriteria Remisi AmldjebrutNo ratings yet
- Hematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamDocument72 pagesHematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamAstri Arri FebriantiNo ratings yet
- MR 25Document9 pagesMR 25Riko JumattullahNo ratings yet
- Acute Lukemia FinalDocument248 pagesAcute Lukemia FinalRakesh JadhavNo ratings yet
- Acute Erythroid Leukemia: Review ArticleDocument10 pagesAcute Erythroid Leukemia: Review Articlemita potabugaNo ratings yet
- Myeloproliferative Neoplasms: Diagnostic Workup of The Cythemic PatientDocument9 pagesMyeloproliferative Neoplasms: Diagnostic Workup of The Cythemic PatientHashim AhmadNo ratings yet
- Mixed Phenotype Acute LeukemiaDocument10 pagesMixed Phenotype Acute LeukemiaMarco Aurélio SartoriNo ratings yet
- Leukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUDocument47 pagesLeukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUJr SparkNo ratings yet
- Acute Myeloid LeukemiaDocument20 pagesAcute Myeloid LeukemiahemendreNo ratings yet
- American J Hematol - 2022 - Patnaik - Chronic Myelomonocytic Leukemia 2022 Update On Diagnosis Risk Stratification andDocument21 pagesAmerican J Hematol - 2022 - Patnaik - Chronic Myelomonocytic Leukemia 2022 Update On Diagnosis Risk Stratification andamysweet.everNo ratings yet
- Laparoscopic AdrenalectomyDocument12 pagesLaparoscopic AdrenalectomyTay SalinasNo ratings yet
- Bowel Obstruction StatPearlsDocument5 pagesBowel Obstruction StatPearlsTay SalinasNo ratings yet
- Nodulos Tiroideos PDFDocument16 pagesNodulos Tiroideos PDFTay SalinasNo ratings yet
- Mesenterico PDFDocument7 pagesMesenterico PDFTay SalinasNo ratings yet
- Dysphagia: Ahmad S. Ashrafi, and R. Sudhir SundaresanDocument9 pagesDysphagia: Ahmad S. Ashrafi, and R. Sudhir SundaresanTay SalinasNo ratings yet
- Placental Vascular Pathology and Increased Thrombin Generation As Mechanisms of Disease in Obstetrical SyndromesDocument26 pagesPlacental Vascular Pathology and Increased Thrombin Generation As Mechanisms of Disease in Obstetrical SyndromesTay SalinasNo ratings yet
- Railway Ballast PerformanceDocument27 pagesRailway Ballast PerformanceSamuel Carlos Sanjuán TorresNo ratings yet
- Controllers and Controller StationsDocument65 pagesControllers and Controller StationsLucian ChorusNo ratings yet
- Progressive Utilisation Prospects of Coal Fly Ash A ReviewDocument36 pagesProgressive Utilisation Prospects of Coal Fly Ash A ReviewDivakar SaiNo ratings yet
- Exhaust Gas Recirculation (EGR)Document18 pagesExhaust Gas Recirculation (EGR)Srinath Pai100% (1)
- Project Documentation SandeepDocument19 pagesProject Documentation SandeepFYIT80Sultan ShaikhNo ratings yet
- Motion Information and MediaDocument39 pagesMotion Information and Mediajadeshades12No ratings yet
- (Chris A.M. Peters, Joseph H. M. Steenbrink) Mixed Hodge StructuresDocument467 pages(Chris A.M. Peters, Joseph H. M. Steenbrink) Mixed Hodge StructuresShaulB7100% (1)
- Inspiratory Muscle TrainingDocument15 pagesInspiratory Muscle Trainingulfapanjaitan100% (2)
- Scati DAT ScatiEye - SES 1604 - Bracket enDocument2 pagesScati DAT ScatiEye - SES 1604 - Bracket enEnrique ColoniaNo ratings yet
- Tabel EmisivitasDocument16 pagesTabel EmisivitasImam Bukhori100% (1)
- SyllogismDocument25 pagesSyllogismSunil GahlotNo ratings yet
- Product Requirements Specification Process in ProdDocument12 pagesProduct Requirements Specification Process in ProdemmyNo ratings yet
- Caudal Duplication Syndrome-Report of A CaseDocument4 pagesCaudal Duplication Syndrome-Report of A Casekhumaira1982No ratings yet
- Turbodrain EnglDocument8 pagesTurbodrain EnglIonut BuzescuNo ratings yet
- Park Tool - Torque Specifications and ConceptsDocument9 pagesPark Tool - Torque Specifications and ConceptszuberNo ratings yet
- Our Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Document3 pagesOur Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Abimanyu ShenilNo ratings yet
- Comparison of The Ratios of Coca Cola and PepsiDocument6 pagesComparison of The Ratios of Coca Cola and PepsiassadullahNo ratings yet
- General Twin Seal 06Document24 pagesGeneral Twin Seal 06Gk GaneshNo ratings yet
- UG RA 005 - Thermal Integrity and Resistivity TestingDocument6 pagesUG RA 005 - Thermal Integrity and Resistivity TestingshamshuddinNo ratings yet
- Quantitative Interpretation of The Response of Surface Plasmon Resonance Sensors To Adsorbed FilmsDocument13 pagesQuantitative Interpretation of The Response of Surface Plasmon Resonance Sensors To Adsorbed FilmsKaren Régules MedelNo ratings yet
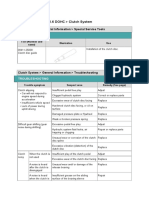
- 06.clutch SystemDocument24 pages06.clutch SystemTony D'AngeloNo ratings yet
- MN402 01Document22 pagesMN402 01UnknownNo ratings yet
- 5th Fancy BreadDocument7 pages5th Fancy BreadMera Funportal0% (1)
- Individual Development WorkoutDocument3 pagesIndividual Development WorkoutmichelleNo ratings yet
- Drill ShaftDocument462 pagesDrill ShaftngodangquangNo ratings yet
- Nabcep AppendixesDocument32 pagesNabcep AppendixeshockpinNo ratings yet
- FYP Module 1 IntroductionDocument32 pagesFYP Module 1 IntroductionAizuddin SazaliNo ratings yet
- Dorothy E. Johnson: Behavioral System ModelDocument15 pagesDorothy E. Johnson: Behavioral System Modelwickwax100% (1)
- 2012 Training Materials PDFDocument32 pages2012 Training Materials PDFWisam Ankah100% (1)