Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- CHAKRA FOR SEX - Harnessing The Sexual EnergyDocument36 pagesCHAKRA FOR SEX - Harnessing The Sexual EnergyDamir67% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Offshore Engineer-February 2015Document84 pagesOffshore Engineer-February 2015ilkerkozturk100% (2)
- 2 Material HandlingDocument218 pages2 Material HandlingJon Blac100% (1)
- Dance Like A ManDocument4 pagesDance Like A ManShubhadip aichNo ratings yet
- Materials Letters: Featured LetterDocument4 pagesMaterials Letters: Featured Letterbiomedicalengineer 27No ratings yet
- FRANKL, CROSSLEY, 2000, Gothic Architecture IDocument264 pagesFRANKL, CROSSLEY, 2000, Gothic Architecture IGurunadham MuvvaNo ratings yet
- Palanca vs. CADocument16 pagesPalanca vs. CASherwin Anoba CabutijaNo ratings yet
- A Conversation Explaining BiomimicryDocument6 pagesA Conversation Explaining Biomimicryapi-3703075100% (2)
- G.R. No. 52179 - Municipality of San Fernando, La Union v. FirmeDocument6 pagesG.R. No. 52179 - Municipality of San Fernando, La Union v. FirmeBluebells33No ratings yet
- Mathematics: Quarter 3 - Module 5: Independent & Dependent EventsDocument19 pagesMathematics: Quarter 3 - Module 5: Independent & Dependent EventsAlexis Jon NaingueNo ratings yet
- Presentation: Like/love + Noun or - Ing FormDocument2 pagesPresentation: Like/love + Noun or - Ing FormKaren GimezNo ratings yet
- Fadi CV 030309Document5 pagesFadi CV 030309fkhaterNo ratings yet
- International Capital BudgetingDocument29 pagesInternational Capital BudgetingSaadat ShaikhNo ratings yet
- RA 020 Risk Assessment - Risk Assessment - Installation of Cables in Ducts & TrenchesDocument11 pagesRA 020 Risk Assessment - Risk Assessment - Installation of Cables in Ducts & Trenchesthomson100% (2)
- Where Have All The Peasants Gone Susana NarotskyDocument21 pagesWhere Have All The Peasants Gone Susana NarotskyHoward Steven Rojas DivantoqueNo ratings yet
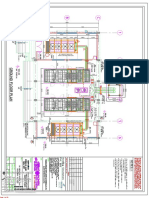
- Dg-1 (Remote Radiator) Above Control Room Slab: 05-MAR-2018 Atluri Mohan Krishna (B845)Document32 pagesDg-1 (Remote Radiator) Above Control Room Slab: 05-MAR-2018 Atluri Mohan Krishna (B845)Shaik AbdullaNo ratings yet
- Lap Trình KeyenceDocument676 pagesLap Trình Keyencetuand1No ratings yet
- Global Guidelines For The Prevention of Surgical Site Infection: An IntroductionDocument8 pagesGlobal Guidelines For The Prevention of Surgical Site Infection: An IntroductionJNUHospital NABHNo ratings yet
- 4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMDocument2 pages4.54 A EN DS RDBF01RDBF02RDBF03RDGD01 Sprinkler Guard and Shield FMAhmad AliNo ratings yet
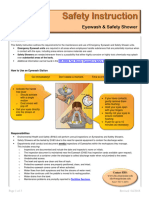
- Eyewash and Safety Shower SiDocument3 pagesEyewash and Safety Shower SiAli EsmaeilbeygiNo ratings yet
- Презентация smartwatchesDocument10 pagesПрезентация smartwatchesZiyoda AbdulloevaNo ratings yet
- Aire - 1 ReinigenDocument25 pagesAire - 1 Reinigengino aldo palomino ludeñaNo ratings yet
- Recruitment Requisition FormDocument1 pageRecruitment Requisition FormrahulNo ratings yet
- Woolworths Group Limited, Share Purchase Plan (SPP) Cancellation of Salary Sacrifice Arrangements Form F20-21Document1 pageWoolworths Group Limited, Share Purchase Plan (SPP) Cancellation of Salary Sacrifice Arrangements Form F20-21HaadS.AbbasiNo ratings yet
- Panadent SystemDocument70 pagesPanadent SystemDhananjay GandageNo ratings yet
- Amyand's HerniaDocument5 pagesAmyand's HerniamonoarulNo ratings yet
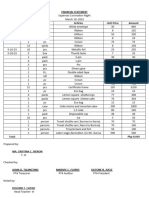
- Financial Statement Coronation NightDocument8 pagesFinancial Statement Coronation NightRuel Gapuz ManzanoNo ratings yet
- Proforma Invoice: TOTAL:300000 Meters $3,900,000Document3 pagesProforma Invoice: TOTAL:300000 Meters $3,900,000Eslam A. AliNo ratings yet
- Enfermedades Emergentes y Embarazo - EID - November 2006 - Volume CompletoDocument187 pagesEnfermedades Emergentes y Embarazo - EID - November 2006 - Volume CompletoRuth Vargas GonzalesNo ratings yet
- Priority Payment: The Status For Payment 78735WQ007TU Is: Pending AuthorisationDocument3 pagesPriority Payment: The Status For Payment 78735WQ007TU Is: Pending AuthorisationShohag RaihanNo ratings yet