Download as pdf or txt
You might also like
- Aerial Yoga Manual 2018 Third Edition ADocument156 pagesAerial Yoga Manual 2018 Third Edition Atito1628100% (8)
- Aerial Yoga Manual 2018 Third Edition ADocument156 pagesAerial Yoga Manual 2018 Third Edition Atito1628100% (8)
- Alberto Villoldo Book PDFDocument120 pagesAlberto Villoldo Book PDFtito1628100% (4)
- Regulatory Affairs PDFDocument27 pagesRegulatory Affairs PDFDipak BhingardeveNo ratings yet
- Cleaning Validation Guidelines - A Complete ListDocument11 pagesCleaning Validation Guidelines - A Complete ListSanjay SharmaNo ratings yet
- GMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsFrom EverandGMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsRating: 5 out of 5 stars5/5 (2)
- Appendix 1 Compulsory Exercises Aerial Silk Eng 2018Document23 pagesAppendix 1 Compulsory Exercises Aerial Silk Eng 2018tito1628100% (6)
- The Formalized Risk Assessment For Excipients - GenialDocument22 pagesThe Formalized Risk Assessment For Excipients - Genialtito1628No ratings yet
- Fundamentals of An Environmental Monitoring ProgramDocument71 pagesFundamentals of An Environmental Monitoring Programtito1628No ratings yet
- Pharmacological PlanDocument10 pagesPharmacological Planaadrika negiNo ratings yet
- International PV Lec 4Document26 pagesInternational PV Lec 4Eman AhmedNo ratings yet
- Pharmacovigilance-Related Topics Lec 2 CpyDocument22 pagesPharmacovigilance-Related Topics Lec 2 CpyEman AhmedNo ratings yet
- PV Guidance DocumentDocument54 pagesPV Guidance DocumentRenneyNo ratings yet
- RAHB - Unit IIIDocument60 pagesRAHB - Unit IIIManas DhariyaNo ratings yet
- Review Management: Manual of Policies and Procedures Center For Drug Evaluation and Research MAPP 6700.1Document8 pagesReview Management: Manual of Policies and Procedures Center For Drug Evaluation and Research MAPP 6700.1depardieu1973No ratings yet
- 2020 09 H PP EuropaBio Patient-EngagementDocument6 pages2020 09 H PP EuropaBio Patient-Engagementqichen0818No ratings yet
- KAHKASHADocument107 pagesKAHKASHAcity9848835243 cyberNo ratings yet
- BP702T Ip IiiDocument27 pagesBP702T Ip IiiGURU PRASAD TIWARINo ratings yet
- GHTF-Quality Management System - Medical Devices - Guidance On Corrective Action and Preventive Action and Related QMS ProcessesDocument26 pagesGHTF-Quality Management System - Medical Devices - Guidance On Corrective Action and Preventive Action and Related QMS ProcessesSam Moses100% (1)
- 1.preface The International Pharmacopoeia, Tenth EditionDocument3 pages1.preface The International Pharmacopoeia, Tenth Editionزيد هشام السيدNo ratings yet
- Elemental Impurities PDFDocument85 pagesElemental Impurities PDFsuey0209No ratings yet
- Guidelines Developing National Drug Policies: World OrganizationDocument56 pagesGuidelines Developing National Drug Policies: World Organizationsome buddyyNo ratings yet
- Clinical Pharmacology and PharmacodynamicsDocument23 pagesClinical Pharmacology and Pharmacodynamicsrr48843No ratings yet
- Access New Medicines TR PIO Collaboration ResearchDocument184 pagesAccess New Medicines TR PIO Collaboration ResearchJoana Brazão CachuloNo ratings yet
- International Conference Harmonisation Technical Requirements Registration Pharmaceuticals Human Use - en 25Document16 pagesInternational Conference Harmonisation Technical Requirements Registration Pharmaceuticals Human Use - en 25Karla GarcíaNo ratings yet
- IntroductionDocument6 pagesIntroductionعبدالعزيز بدرNo ratings yet
- GDP (Informe 40)Document23 pagesGDP (Informe 40)eeNo ratings yet
- Ype The Company Name: Abbreviations in The Pharmaceutical Industry: Key Terms in Drug Development and RegulationDocument7 pagesYpe The Company Name: Abbreviations in The Pharmaceutical Industry: Key Terms in Drug Development and RegulationNajeebNo ratings yet
- Pharmaco Vigilance 1Document9 pagesPharmaco Vigilance 1chatrapatigraphics252No ratings yet
- Clinical Guidelines Ecbs 2001Document52 pagesClinical Guidelines Ecbs 2001Ajay KumarNo ratings yet
- S 14136 eDocument416 pagesS 14136 eaminos90No ratings yet
- Guidelines For Product RecallDocument18 pagesGuidelines For Product RecallSenthamaraiShanmughamNo ratings yet
- ICH - by MeDocument21 pagesICH - by MesahooprapteeNo ratings yet
- Global Regulatory Strategy For Veterinary MedicinesDocument11 pagesGlobal Regulatory Strategy For Veterinary MedicinesCsar Sanchez Gracia50% (2)
- FDA PhotostabilityDocument8 pagesFDA PhotostabilityLina SakellariouNo ratings yet
- Monografi Obat WHODocument84 pagesMonografi Obat WHOade_boy2imutNo ratings yet
- Goldsmith 1998Document3 pagesGoldsmith 1998Carlita LuzónNo ratings yet
- ICH Q9 GuidelineDocument23 pagesICH Q9 GuidelineSairam EdupugantiNo ratings yet
- 47 FAQs RH Medicines For WHO PrequalifucationDocument9 pages47 FAQs RH Medicines For WHO PrequalifucationAmit KochharNo ratings yet
- S14136e PDFDocument416 pagesS14136e PDFAgung Perkasa0% (1)
- 2006 The IPEC Good Distribution Practices GuidelineDocument29 pages2006 The IPEC Good Distribution Practices GuidelineHertchel Lozano100% (1)
- Guideline For Registration of Low Risk MedicinesDocument23 pagesGuideline For Registration of Low Risk Medicinesmelaku yazieNo ratings yet
- X-Ray GuidelinesDocument76 pagesX-Ray Guidelinesanggabianz100% (1)
- COMMON TECHNICAL DOCUMENTS For Industry - NigeriaDocument99 pagesCOMMON TECHNICAL DOCUMENTS For Industry - NigeriaAnkur Drugs and Pharma Ltd.No ratings yet
- PAT - A Framework For Innovative Pharmaceutical Development, Manufacturing, and Quality AssuranceDocument19 pagesPAT - A Framework For Innovative Pharmaceutical Development, Manufacturing, and Quality AssuranceHeba El-TayebNo ratings yet
- Annex 4: WHO - TRS - 981.indb 155 16/04/13 08:26Document34 pagesAnnex 4: WHO - TRS - 981.indb 155 16/04/13 08:26schumonNo ratings yet
- Guidelines On Import Procedures For Pharmaceutical ProductsDocument14 pagesGuidelines On Import Procedures For Pharmaceutical Productsjot GuiaoNo ratings yet
- E11 GuidelineDocument16 pagesE11 GuidelinevyshnosudhaNo ratings yet
- ICH Q3E ConceptPaper 2020 0710Document3 pagesICH Q3E ConceptPaper 2020 0710rodcam1No ratings yet
- WHO Drug Information 2000Document66 pagesWHO Drug Information 2000Rajib ChowdhuryNo ratings yet
- EU-GMP.2014 - Annex - 20 (Quality Risk Management)Document25 pagesEU-GMP.2014 - Annex - 20 (Quality Risk Management)bvsc77035No ratings yet
- The Ipec Excipient Stability Program GuideDocument18 pagesThe Ipec Excipient Stability Program GuideshrikantmsdNo ratings yet
- 1.preface The International Pharmacopoeia, Eleventh EditionDocument3 pages1.preface The International Pharmacopoeia, Eleventh EditionLIZ NORMA ARROYO TORRESNo ratings yet
- Pharmaco VigilanceDocument19 pagesPharmaco VigilanceJayson MontemayorNo ratings yet
- Krishna Mba ProDocument24 pagesKrishna Mba ProKrishnaSinghNo ratings yet
- Clinical Safety Data Management Periodic Safety UpdateDocument19 pagesClinical Safety Data Management Periodic Safety UpdatedopamNo ratings yet
- Ansh File FinalDocument31 pagesAnsh File Finala7465426No ratings yet
- What Is A Risk Management PlanDocument2 pagesWhat Is A Risk Management PlanAre Pee EtcNo ratings yet
- Guideline For JapanDocument27 pagesGuideline For Japandepardieu1973No ratings yet
- Fig: Role of Regulatory Affairs in Pharmaceutical IndustryDocument3 pagesFig: Role of Regulatory Affairs in Pharmaceutical IndustryMonem Shahriar Ibn FaruqueNo ratings yet
- Hvs NirpharmaDocument22 pagesHvs NirpharmaSubhadip BanerjeeNo ratings yet
- UntitledDocument5 pagesUntitledNguyễn HiếuNo ratings yet
- Importance of Pharmacovigilance For Pharmaceutical IndustryDocument24 pagesImportance of Pharmacovigilance For Pharmaceutical IndustryPiratesNo ratings yet
- Pharmacovigilance Medical Writing: A Good Practice GuideFrom EverandPharmacovigilance Medical Writing: A Good Practice GuideRating: 4 out of 5 stars4/5 (1)
- International Code of Conduct on Pesticide Management: Guidance for Inspection of Pesticide Producers, Importers, Distributors and RetailersFrom EverandInternational Code of Conduct on Pesticide Management: Guidance for Inspection of Pesticide Producers, Importers, Distributors and RetailersNo ratings yet
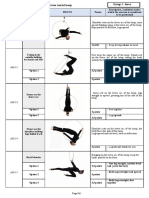
- Appendix 2 Compulsory Exercises Aerial Hoop 2018 EngDocument28 pagesAppendix 2 Compulsory Exercises Aerial Hoop 2018 Engtito1628100% (1)
- Company - Business Form: Business System Management Review TemplateDocument12 pagesCompany - Business Form: Business System Management Review Templatetito1628No ratings yet
- The Aerial Sling Manual: Prev Iew Prev IewDocument13 pagesThe Aerial Sling Manual: Prev Iew Prev Iewtito1628100% (1)
- Online OgilvieDocument7 pagesOnline Ogilvietito1628No ratings yet
- Technical Guide Change ControlDocument42 pagesTechnical Guide Change Controltito1628No ratings yet
- A Historical View of Human Resource ManagementDocument12 pagesA Historical View of Human Resource Managementtito1628No ratings yet
- Paper Fitness ClubDocument6 pagesPaper Fitness Clubtito1628No ratings yet
- Cermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaDocument2 pagesCermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaLaila Kurnia PramonoNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- Healthcare Organizations in Saudi ArabiaDocument10 pagesHealthcare Organizations in Saudi ArabiaJohn GomezNo ratings yet
- Chapter 2-Introduction To Health EconomicsDocument9 pagesChapter 2-Introduction To Health EconomicsLalita A/P AnbarasenNo ratings yet
- Nys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsDocument4 pagesNys Medicaid Pre-Adjudication Crosswalk For Health Care ClaimsTeresaNo ratings yet
- Final ProjectDocument27 pagesFinal ProjectMuhammad AwaisNo ratings yet
- The American Dream EssayDocument3 pagesThe American Dream Essayapi-331970133No ratings yet
- Nursing Care Plan: Risk For InfectionDocument3 pagesNursing Care Plan: Risk For Infectiongeorgeborja414726100% (3)
- Solution Manual Health Care Economics 7th Edition by Paul J. Feldstein SLC1106Document4 pagesSolution Manual Health Care Economics 7th Edition by Paul J. Feldstein SLC1106Thar AdeleiNo ratings yet
- Infection Prevention and Control (IPC) For COVID-19 VirusDocument21 pagesInfection Prevention and Control (IPC) For COVID-19 Virusalta graceNo ratings yet
- Konnichi Yawa Sa Mock Review Ictmpart1Document8 pagesKonnichi Yawa Sa Mock Review Ictmpart1Wansun MaglangitNo ratings yet
- Epidemiology - Intro - 11Document58 pagesEpidemiology - Intro - 11Tin WannNo ratings yet
- Disease Management For SchizophreniaDocument16 pagesDisease Management For SchizophreniaNational Pharmaceutical CouncilNo ratings yet
- EarlySense BrochureDocument4 pagesEarlySense BrochureIsrael ExporterNo ratings yet
- Nurs FPX 4020 Assessment 4 Improvement Plan Tool KitDocument6 pagesNurs FPX 4020 Assessment 4 Improvement Plan Tool KitCarolyn HarkerNo ratings yet
- Informatics ProjectDocument14 pagesInformatics Projectapi-665681076No ratings yet
- Ao2019 0002 PDFDocument17 pagesAo2019 0002 PDFLen SabayNo ratings yet
- Provider Id Numbers and Plan Codes: Medicaid Managed Care PlanDocument5 pagesProvider Id Numbers and Plan Codes: Medicaid Managed Care PlanMike DurkeeNo ratings yet
- Fy2015 CJ CDC FinalDocument461 pagesFy2015 CJ CDC FinalMark ReinhardtNo ratings yet
- Volume 1 Ministerial Meeting Final enDocument61 pagesVolume 1 Ministerial Meeting Final enAssou KekNo ratings yet
- Skills: Gourav JainDocument2 pagesSkills: Gourav JainNISHKARSH. MAURYANo ratings yet
- Re AWH JCI Mock Survey Agenda 8 - 13 March 2023Document20 pagesRe AWH JCI Mock Survey Agenda 8 - 13 March 2023balqeesomar8No ratings yet
- 5 Safety Health ResourcesDocument1 page5 Safety Health ResourcesJojolasNo ratings yet
- Community MedicineDocument49 pagesCommunity MedicineRiyaz AhamedNo ratings yet
- Chapter 15 Economic IssuesDocument4 pagesChapter 15 Economic IssuesAjien TaiajNo ratings yet
- UB-04 Billing Instructions Revision Table: Revision Date Sections Revised DescriptionDocument24 pagesUB-04 Billing Instructions Revision Table: Revision Date Sections Revised DescriptioncmabryNo ratings yet
- Medical Sociology 13th Edition Cockerham Test BankDocument36 pagesMedical Sociology 13th Edition Cockerham Test Bankwinifredmilcah4oo1100% (15)
- Interpreter Worksheet For Interpreting Solutions To PatientsDocument1 pageInterpreter Worksheet For Interpreting Solutions To PatientsSteven MooreNo ratings yet
- HMIS Data 02.11.2022Document92 pagesHMIS Data 02.11.2022Manish Mishra Biomedical EngineerNo ratings yet
- Navigating The Relationship Between Third-Party Payers and Pharmacy Providers of MTMDocument29 pagesNavigating The Relationship Between Third-Party Payers and Pharmacy Providers of MTMgmajdalaniiNo ratings yet