
Hydrocephalus
Hydrocephalus
You might also like
- Outsmart Your Cancer - Tanya PierceDocument530 pagesOutsmart Your Cancer - Tanya PierceParallaxster100% (4)
- Atlas of Canine and Feline Peripheral Blood SmearsDocument516 pagesAtlas of Canine and Feline Peripheral Blood SmearsLaura MewsNo ratings yet
- Child Protection Policy TemplateDocument2 pagesChild Protection Policy TemplateJewelyn Retome100% (1)
- Lesson Plan ON Congenital SyphilisDocument19 pagesLesson Plan ON Congenital SyphilisRenuga SureshNo ratings yet
- Lumbar PunctureDocument27 pagesLumbar PunctureWitneyGrace100% (1)
- Models of PreventionDocument21 pagesModels of Preventionprecillathoppil100% (6)
- Course PlANDocument7 pagesCourse PlANprecillathoppil50% (4)
- Building Resilience in Preschool ChildrenDocument65 pagesBuilding Resilience in Preschool ChildrenAnamari SlavicNo ratings yet
- Hydrocephalus PPT SSMC RewaDocument60 pagesHydrocephalus PPT SSMC RewaAbhishek Mishra100% (3)
- HydrocephalusDocument33 pagesHydrocephalusrajan kumar100% (2)
- Lumbar Puncture: First LP TechniqueDocument8 pagesLumbar Puncture: First LP TechniquenamithaNo ratings yet
- Modern Concept of Child CareDocument14 pagesModern Concept of Child CareKiranNo ratings yet
- Endotracheal Suctioning PDFDocument4 pagesEndotracheal Suctioning PDFDebipriya MistryNo ratings yet
- Administration of OxygenDocument52 pagesAdministration of OxygenSivabarathy50% (2)
- Case Study BronchiolitisDocument15 pagesCase Study Bronchiolitisanimesh panda0% (1)
- HydrocephalusDocument72 pagesHydrocephalusZharah RuzNo ratings yet
- Lesson Plan Section IDocument17 pagesLesson Plan Section IAshly NygilNo ratings yet
- Case 2 Hydrocephalus Group 4Document27 pagesCase 2 Hydrocephalus Group 4younggirldavidNo ratings yet
- Rheumatic Heart DiseaseDocument37 pagesRheumatic Heart Diseasesalman hNo ratings yet
- HydrocephalusDocument8 pagesHydrocephalusJean Albine CatipanNo ratings yet
- Neurological AssessmentDocument18 pagesNeurological AssessmentMackenzie GaranNo ratings yet
- Nephrotic SyndromeDocument17 pagesNephrotic Syndromevishnu0% (1)
- Nursing Management of Patient With Mechanical VentilationDocument77 pagesNursing Management of Patient With Mechanical Ventilationrojina poudel0% (1)
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDocument23 pagesAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaNo ratings yet
- HydrocephalusDocument25 pagesHydrocephalusعمارہ عمر100% (1)
- Group 11 Cleft Lip and Cleft Palate Case Study N2BDocument46 pagesGroup 11 Cleft Lip and Cleft Palate Case Study N2BLerma PagcaliwanganNo ratings yet
- Government College of Nursing, Jodhpur (Raj.) : Ballard ScoringDocument14 pagesGovernment College of Nursing, Jodhpur (Raj.) : Ballard ScoringASHISH KUMAR YADAV100% (1)
- Reffractive ErrorsDocument13 pagesReffractive ErrorsSagiraju SrinuNo ratings yet
- Case Presentation On ARMsDocument39 pagesCase Presentation On ARMsSomyee PachuauNo ratings yet
- Hirschsprung Disease (Aganglionic Megacolon)Document6 pagesHirschsprung Disease (Aganglionic Megacolon)Julliza Joy PandiNo ratings yet
- The Challenged ChildDocument17 pagesThe Challenged ChildAmy Lalringhluani Chhakchhuak50% (2)
- Choanal Atresia, Epistaxis & AspirationDocument12 pagesChoanal Atresia, Epistaxis & Aspirationsubinj_350% (2)
- Neonatal SepsisDocument63 pagesNeonatal SepsisDemewoz Fikir100% (2)
- Congenital AnomaliesDocument94 pagesCongenital AnomaliesDeepti Kukreti100% (1)
- Convulsions in ChildrenDocument12 pagesConvulsions in ChildrenShesly Philomina0% (1)
- EncephalitisDocument37 pagesEncephalitisPRADEEPNo ratings yet
- Presentation On Guillain Barre Syndrome: Submitted To: Submitted byDocument12 pagesPresentation On Guillain Barre Syndrome: Submitted To: Submitted bypandem soniyaNo ratings yet
- Accidentpreventioninchildren 160508054518Document28 pagesAccidentpreventioninchildren 160508054518maanka aliNo ratings yet
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Intestinal Obstruction FinalDocument10 pagesIntestinal Obstruction FinalAmlan jyoti thanapatiNo ratings yet
- Oxygen InsufficiencyDocument93 pagesOxygen InsufficiencyAnjali Rahul Ajmeri100% (2)
- Hydrocephalus N C P BY BHERU LALDocument1 pageHydrocephalus N C P BY BHERU LALBheru LalNo ratings yet
- HypothermiaDocument5 pagesHypothermiaMRS CHAKRAPANINo ratings yet
- Child Guidance ClinicDocument8 pagesChild Guidance Clinicpurnasha_mitra12100% (6)
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Drugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterDocument42 pagesDrugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterPrernaSharma100% (1)
- NCP HydrocephalusDocument10 pagesNCP HydrocephalusHardeep Akku100% (1)
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- Seminar On Bronchial Asthma NewDocument42 pagesSeminar On Bronchial Asthma NewShabna SameerNo ratings yet
- Case Presentation: HydrocephalusDocument22 pagesCase Presentation: HydrocephalusNina100% (2)
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDocument10 pagesSister Nivedita Govt. Nursing College Igmc, ShimlashivaniNo ratings yet
- Assisting in Ventilator Care ProcedureDocument13 pagesAssisting in Ventilator Care ProcedureSAYMABANU100% (1)
- Tetralogy of FallotDocument10 pagesTetralogy of FallotanggiehardiyantiNo ratings yet
- Otitis MediaDocument39 pagesOtitis MediaGilian Dacanay100% (4)
- Assignment On Unconciousness: Subject:-Advanced Nursing PracticeDocument15 pagesAssignment On Unconciousness: Subject:-Advanced Nursing PracticeShaells JoshiNo ratings yet
- Meningitis PPT 2.0Document15 pagesMeningitis PPT 2.0Francis Adrian100% (1)
- Leukaemia PDFDocument21 pagesLeukaemia PDFbrijsingNo ratings yet
- Pulse OximetryDocument3 pagesPulse OximetryJanna Favila100% (3)
- Lesson Plan Wilms TumorDocument29 pagesLesson Plan Wilms TumorAnusha Verghese100% (2)
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Hydrocephalus PDFDocument17 pagesHydrocephalus PDFEdna López100% (1)
- Ventricles of BrainDocument16 pagesVentricles of BrainAzeemNo ratings yet
- Hydrocephalus .WPS OfficeDocument87 pagesHydrocephalus .WPS Officepiyushk999.60No ratings yet
- Bahan Hidrosefalus2Document17 pagesBahan Hidrosefalus2Arry Wijaya LieNo ratings yet
- Cerebrospinal Fluid: Dr. Usman Farooq (PT) Lecturer NWIHS DPT, MS-NMPTDocument14 pagesCerebrospinal Fluid: Dr. Usman Farooq (PT) Lecturer NWIHS DPT, MS-NMPTtwity 1No ratings yet
- Pathway, Show The Major Pathway of CSF Flow. Beginning in The Lateral Ventricles, CSF FlowsDocument2 pagesPathway, Show The Major Pathway of CSF Flow. Beginning in The Lateral Ventricles, CSF FlowsMary Scarlette CenaNo ratings yet
- PHPQ 6 X 8 SSDocument6 pagesPHPQ 6 X 8 SSprecillathoppilNo ratings yet
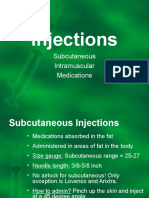
- Injections: Subcutaneous Intramuscular MedicationsDocument9 pagesInjections: Subcutaneous Intramuscular MedicationsprecillathoppilNo ratings yet
- Visit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7Document7 pagesVisit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7precillathoppilNo ratings yet
- Current Trends in Nursing Educaion..MadhuDocument13 pagesCurrent Trends in Nursing Educaion..Madhuprecillathoppil100% (3)
- AbgDocument8 pagesAbgprecillathoppilNo ratings yet
- Master Rotatoin Plan M.SC Nursing 1st YearDocument2 pagesMaster Rotatoin Plan M.SC Nursing 1st YearprecillathoppilNo ratings yet
- Principles of PreventionDocument14 pagesPrinciples of PreventionprecillathoppilNo ratings yet
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocument6 pagesCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (25)
- Av Aids FinalDocument17 pagesAv Aids Finalprecillathoppil0% (1)
- Guidance & CounsellingDocument16 pagesGuidance & Counsellingprecillathoppil67% (9)
- Jsa Removal Fixing InsulationDocument2 pagesJsa Removal Fixing InsulationAprilia Rizki Ardila63% (8)
- The Experiences of Pregnant Teenagers About Their Pregnancy: Julie RangiahDocument93 pagesThe Experiences of Pregnant Teenagers About Their Pregnancy: Julie RangiahRonald Pacquiao MacaseroNo ratings yet
- Stemetil DCS SlideDocument31 pagesStemetil DCS SlideSanchit GargNo ratings yet
- RRLDocument7 pagesRRLFaye Dianne Damian-BuenafeNo ratings yet
- 1392149762keystone Reliance Reference Guide Feb 2014Document9 pages1392149762keystone Reliance Reference Guide Feb 2014Thiago BerthaudNo ratings yet
- Metabolism of XenobioticsDocument5 pagesMetabolism of XenobioticsJanelle Bondad100% (2)
- Bài Thi nói Tiếng Anh lớp 10 HKIDocument2 pagesBài Thi nói Tiếng Anh lớp 10 HKIMonochrome Neko ChanNo ratings yet
- Randomized Clinical TrialsDocument35 pagesRandomized Clinical TrialsFatt ZakiNo ratings yet
- Dka CalculatorDocument1 pageDka CalculatordelfiaNo ratings yet
- Tilt Table Testing For Assesing SyncopeDocument13 pagesTilt Table Testing For Assesing SyncopeNino SatriaNo ratings yet
- Table of Specifications in Bachelor of Physical Education/Grade 9 (Multiple Choice Test)Document1 pageTable of Specifications in Bachelor of Physical Education/Grade 9 (Multiple Choice Test)Gilbert Bulado0% (1)
- Jaha 120 017275Document150 pagesJaha 120 017275Leonardo LiswojoNo ratings yet
- Dental Fear ThesisDocument6 pagesDental Fear Thesismaritzapetersonpaterson100% (2)
- BW Muscle Gift PDFDocument22 pagesBW Muscle Gift PDFRohit Yadav100% (4)
- Respiratory Mechanics and Introduction To Respiratory PhysiologyDocument55 pagesRespiratory Mechanics and Introduction To Respiratory PhysiologyhariNo ratings yet
- Knowledge Attitudes and Practices Toward COVID-19Document9 pagesKnowledge Attitudes and Practices Toward COVID-19Nurin AdlinNo ratings yet
- MAPEH 10 4th Periodical TestDocument4 pagesMAPEH 10 4th Periodical TestJohn Alter LaraNo ratings yet
- Sample StoryboardDocument20 pagesSample StoryboardJFS100% (1)
- Acute PancreatitisDocument9 pagesAcute PancreatitisestefygomezsNo ratings yet
- Vims-Vas Final SeptDocument115 pagesVims-Vas Final SeptR Lamb D LeonNo ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Horm S 23 00313 1Document32 pagesHorm S 23 00313 1andreopNo ratings yet
- Green Building Green Building Codes CodesDocument94 pagesGreen Building Green Building Codes CodesSharvani MedaNo ratings yet
- Application For Iec NriasDocument15 pagesApplication For Iec NriasPavan Kumar TripuraneniNo ratings yet
- Daftar Pustaka Makalah ObatDocument2 pagesDaftar Pustaka Makalah Obatnur adiniNo ratings yet
- Risk Assessment Removal of Walers & StrutsDocument6 pagesRisk Assessment Removal of Walers & StrutsBhargav BbvsNo ratings yet




































































































Download as docx, pdf, or txt
You might also like
- Outsmart Your Cancer - Tanya PierceDocument530 pagesOutsmart Your Cancer - Tanya PierceParallaxster100% (4)
- Atlas of Canine and Feline Peripheral Blood SmearsDocument516 pagesAtlas of Canine and Feline Peripheral Blood SmearsLaura MewsNo ratings yet
- Child Protection Policy TemplateDocument2 pagesChild Protection Policy TemplateJewelyn Retome100% (1)
- Lesson Plan ON Congenital SyphilisDocument19 pagesLesson Plan ON Congenital SyphilisRenuga SureshNo ratings yet
- Lumbar PunctureDocument27 pagesLumbar PunctureWitneyGrace100% (1)
- Models of PreventionDocument21 pagesModels of Preventionprecillathoppil100% (6)
- Course PlANDocument7 pagesCourse PlANprecillathoppil50% (4)
- Building Resilience in Preschool ChildrenDocument65 pagesBuilding Resilience in Preschool ChildrenAnamari SlavicNo ratings yet
- Hydrocephalus PPT SSMC RewaDocument60 pagesHydrocephalus PPT SSMC RewaAbhishek Mishra100% (3)
- HydrocephalusDocument33 pagesHydrocephalusrajan kumar100% (2)
- Lumbar Puncture: First LP TechniqueDocument8 pagesLumbar Puncture: First LP TechniquenamithaNo ratings yet
- Modern Concept of Child CareDocument14 pagesModern Concept of Child CareKiranNo ratings yet
- Endotracheal Suctioning PDFDocument4 pagesEndotracheal Suctioning PDFDebipriya MistryNo ratings yet
- Administration of OxygenDocument52 pagesAdministration of OxygenSivabarathy50% (2)
- Case Study BronchiolitisDocument15 pagesCase Study Bronchiolitisanimesh panda0% (1)
- HydrocephalusDocument72 pagesHydrocephalusZharah RuzNo ratings yet
- Lesson Plan Section IDocument17 pagesLesson Plan Section IAshly NygilNo ratings yet
- Case 2 Hydrocephalus Group 4Document27 pagesCase 2 Hydrocephalus Group 4younggirldavidNo ratings yet
- Rheumatic Heart DiseaseDocument37 pagesRheumatic Heart Diseasesalman hNo ratings yet
- HydrocephalusDocument8 pagesHydrocephalusJean Albine CatipanNo ratings yet
- Neurological AssessmentDocument18 pagesNeurological AssessmentMackenzie GaranNo ratings yet
- Nephrotic SyndromeDocument17 pagesNephrotic Syndromevishnu0% (1)
- Nursing Management of Patient With Mechanical VentilationDocument77 pagesNursing Management of Patient With Mechanical Ventilationrojina poudel0% (1)
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDocument23 pagesAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaNo ratings yet
- HydrocephalusDocument25 pagesHydrocephalusعمارہ عمر100% (1)
- Group 11 Cleft Lip and Cleft Palate Case Study N2BDocument46 pagesGroup 11 Cleft Lip and Cleft Palate Case Study N2BLerma PagcaliwanganNo ratings yet
- Government College of Nursing, Jodhpur (Raj.) : Ballard ScoringDocument14 pagesGovernment College of Nursing, Jodhpur (Raj.) : Ballard ScoringASHISH KUMAR YADAV100% (1)
- Reffractive ErrorsDocument13 pagesReffractive ErrorsSagiraju SrinuNo ratings yet
- Case Presentation On ARMsDocument39 pagesCase Presentation On ARMsSomyee PachuauNo ratings yet
- Hirschsprung Disease (Aganglionic Megacolon)Document6 pagesHirschsprung Disease (Aganglionic Megacolon)Julliza Joy PandiNo ratings yet
- The Challenged ChildDocument17 pagesThe Challenged ChildAmy Lalringhluani Chhakchhuak50% (2)
- Choanal Atresia, Epistaxis & AspirationDocument12 pagesChoanal Atresia, Epistaxis & Aspirationsubinj_350% (2)
- Neonatal SepsisDocument63 pagesNeonatal SepsisDemewoz Fikir100% (2)
- Congenital AnomaliesDocument94 pagesCongenital AnomaliesDeepti Kukreti100% (1)
- Convulsions in ChildrenDocument12 pagesConvulsions in ChildrenShesly Philomina0% (1)
- EncephalitisDocument37 pagesEncephalitisPRADEEPNo ratings yet
- Presentation On Guillain Barre Syndrome: Submitted To: Submitted byDocument12 pagesPresentation On Guillain Barre Syndrome: Submitted To: Submitted bypandem soniyaNo ratings yet
- Accidentpreventioninchildren 160508054518Document28 pagesAccidentpreventioninchildren 160508054518maanka aliNo ratings yet
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Intestinal Obstruction FinalDocument10 pagesIntestinal Obstruction FinalAmlan jyoti thanapatiNo ratings yet
- Oxygen InsufficiencyDocument93 pagesOxygen InsufficiencyAnjali Rahul Ajmeri100% (2)
- Hydrocephalus N C P BY BHERU LALDocument1 pageHydrocephalus N C P BY BHERU LALBheru LalNo ratings yet
- HypothermiaDocument5 pagesHypothermiaMRS CHAKRAPANINo ratings yet
- Child Guidance ClinicDocument8 pagesChild Guidance Clinicpurnasha_mitra12100% (6)
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Drugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterDocument42 pagesDrugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterPrernaSharma100% (1)
- NCP HydrocephalusDocument10 pagesNCP HydrocephalusHardeep Akku100% (1)
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- Seminar On Bronchial Asthma NewDocument42 pagesSeminar On Bronchial Asthma NewShabna SameerNo ratings yet
- Case Presentation: HydrocephalusDocument22 pagesCase Presentation: HydrocephalusNina100% (2)
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDocument10 pagesSister Nivedita Govt. Nursing College Igmc, ShimlashivaniNo ratings yet
- Assisting in Ventilator Care ProcedureDocument13 pagesAssisting in Ventilator Care ProcedureSAYMABANU100% (1)
- Tetralogy of FallotDocument10 pagesTetralogy of FallotanggiehardiyantiNo ratings yet
- Otitis MediaDocument39 pagesOtitis MediaGilian Dacanay100% (4)
- Assignment On Unconciousness: Subject:-Advanced Nursing PracticeDocument15 pagesAssignment On Unconciousness: Subject:-Advanced Nursing PracticeShaells JoshiNo ratings yet
- Meningitis PPT 2.0Document15 pagesMeningitis PPT 2.0Francis Adrian100% (1)
- Leukaemia PDFDocument21 pagesLeukaemia PDFbrijsingNo ratings yet
- Pulse OximetryDocument3 pagesPulse OximetryJanna Favila100% (3)
- Lesson Plan Wilms TumorDocument29 pagesLesson Plan Wilms TumorAnusha Verghese100% (2)
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Hydrocephalus PDFDocument17 pagesHydrocephalus PDFEdna López100% (1)
- Ventricles of BrainDocument16 pagesVentricles of BrainAzeemNo ratings yet
- Hydrocephalus .WPS OfficeDocument87 pagesHydrocephalus .WPS Officepiyushk999.60No ratings yet
- Bahan Hidrosefalus2Document17 pagesBahan Hidrosefalus2Arry Wijaya LieNo ratings yet
- Cerebrospinal Fluid: Dr. Usman Farooq (PT) Lecturer NWIHS DPT, MS-NMPTDocument14 pagesCerebrospinal Fluid: Dr. Usman Farooq (PT) Lecturer NWIHS DPT, MS-NMPTtwity 1No ratings yet
- Pathway, Show The Major Pathway of CSF Flow. Beginning in The Lateral Ventricles, CSF FlowsDocument2 pagesPathway, Show The Major Pathway of CSF Flow. Beginning in The Lateral Ventricles, CSF FlowsMary Scarlette CenaNo ratings yet
- PHPQ 6 X 8 SSDocument6 pagesPHPQ 6 X 8 SSprecillathoppilNo ratings yet
- Injections: Subcutaneous Intramuscular MedicationsDocument9 pagesInjections: Subcutaneous Intramuscular MedicationsprecillathoppilNo ratings yet
- Visit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7Document7 pagesVisit To Nariniketan Jabalpur: 1. To Encourages Adoption of Orphans and Destitute Children. 2. 3. 4. 5. 6. 7precillathoppilNo ratings yet
- Current Trends in Nursing Educaion..MadhuDocument13 pagesCurrent Trends in Nursing Educaion..Madhuprecillathoppil100% (3)
- AbgDocument8 pagesAbgprecillathoppilNo ratings yet
- Master Rotatoin Plan M.SC Nursing 1st YearDocument2 pagesMaster Rotatoin Plan M.SC Nursing 1st YearprecillathoppilNo ratings yet
- Principles of PreventionDocument14 pagesPrinciples of PreventionprecillathoppilNo ratings yet
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocument6 pagesCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (25)
- Av Aids FinalDocument17 pagesAv Aids Finalprecillathoppil0% (1)
- Guidance & CounsellingDocument16 pagesGuidance & Counsellingprecillathoppil67% (9)
- Jsa Removal Fixing InsulationDocument2 pagesJsa Removal Fixing InsulationAprilia Rizki Ardila63% (8)
- The Experiences of Pregnant Teenagers About Their Pregnancy: Julie RangiahDocument93 pagesThe Experiences of Pregnant Teenagers About Their Pregnancy: Julie RangiahRonald Pacquiao MacaseroNo ratings yet
- Stemetil DCS SlideDocument31 pagesStemetil DCS SlideSanchit GargNo ratings yet
- RRLDocument7 pagesRRLFaye Dianne Damian-BuenafeNo ratings yet
- 1392149762keystone Reliance Reference Guide Feb 2014Document9 pages1392149762keystone Reliance Reference Guide Feb 2014Thiago BerthaudNo ratings yet
- Metabolism of XenobioticsDocument5 pagesMetabolism of XenobioticsJanelle Bondad100% (2)
- Bài Thi nói Tiếng Anh lớp 10 HKIDocument2 pagesBài Thi nói Tiếng Anh lớp 10 HKIMonochrome Neko ChanNo ratings yet
- Randomized Clinical TrialsDocument35 pagesRandomized Clinical TrialsFatt ZakiNo ratings yet
- Dka CalculatorDocument1 pageDka CalculatordelfiaNo ratings yet
- Tilt Table Testing For Assesing SyncopeDocument13 pagesTilt Table Testing For Assesing SyncopeNino SatriaNo ratings yet
- Table of Specifications in Bachelor of Physical Education/Grade 9 (Multiple Choice Test)Document1 pageTable of Specifications in Bachelor of Physical Education/Grade 9 (Multiple Choice Test)Gilbert Bulado0% (1)
- Jaha 120 017275Document150 pagesJaha 120 017275Leonardo LiswojoNo ratings yet
- Dental Fear ThesisDocument6 pagesDental Fear Thesismaritzapetersonpaterson100% (2)
- BW Muscle Gift PDFDocument22 pagesBW Muscle Gift PDFRohit Yadav100% (4)
- Respiratory Mechanics and Introduction To Respiratory PhysiologyDocument55 pagesRespiratory Mechanics and Introduction To Respiratory PhysiologyhariNo ratings yet
- Knowledge Attitudes and Practices Toward COVID-19Document9 pagesKnowledge Attitudes and Practices Toward COVID-19Nurin AdlinNo ratings yet
- MAPEH 10 4th Periodical TestDocument4 pagesMAPEH 10 4th Periodical TestJohn Alter LaraNo ratings yet
- Sample StoryboardDocument20 pagesSample StoryboardJFS100% (1)
- Acute PancreatitisDocument9 pagesAcute PancreatitisestefygomezsNo ratings yet
- Vims-Vas Final SeptDocument115 pagesVims-Vas Final SeptR Lamb D LeonNo ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Horm S 23 00313 1Document32 pagesHorm S 23 00313 1andreopNo ratings yet
- Green Building Green Building Codes CodesDocument94 pagesGreen Building Green Building Codes CodesSharvani MedaNo ratings yet
- Application For Iec NriasDocument15 pagesApplication For Iec NriasPavan Kumar TripuraneniNo ratings yet
- Daftar Pustaka Makalah ObatDocument2 pagesDaftar Pustaka Makalah Obatnur adiniNo ratings yet
- Risk Assessment Removal of Walers & StrutsDocument6 pagesRisk Assessment Removal of Walers & StrutsBhargav BbvsNo ratings yet