
Family Case
Family Case
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Aws D8.1M 2013Document40 pagesAws D8.1M 2013vishesh dharaiya100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Name Programme SignatureDocument2 pagesName Programme SignatureJr. CesingNo ratings yet
- Report On Adm.&SupervisionDocument37 pagesReport On Adm.&SupervisionJr. Cesing100% (1)
- Honor & RespectDocument17 pagesHonor & RespectJr. CesingNo ratings yet
- Cardiac Leptospirosis: Iralphuaborque Md14thbatch Hds DocharlabardaDocument15 pagesCardiac Leptospirosis: Iralphuaborque Md14thbatch Hds DocharlabardaJr. CesingNo ratings yet
- Catechism of The Catholic Church: Chapter One: Man'S Capacity For GodDocument7 pagesCatechism of The Catholic Church: Chapter One: Man'S Capacity For GodJr. CesingNo ratings yet
- Catechism of The Catholic Church: Chapter One: Man'S Capacity For GodDocument7 pagesCatechism of The Catholic Church: Chapter One: Man'S Capacity For GodJr. CesingNo ratings yet
- SilenceDocument24 pagesSilenceJr. CesingNo ratings yet
- Bed 2nd Sem ResultDocument1 pageBed 2nd Sem ResultAnusree PranavamNo ratings yet
- Base Institute - Namakkal - PH: 900 37 111 66: - Mock - Ibpsguide.in - 1Document288 pagesBase Institute - Namakkal - PH: 900 37 111 66: - Mock - Ibpsguide.in - 1Kartik MaheshwariNo ratings yet
- Sop-10 Dose Rate MeasurementDocument3 pagesSop-10 Dose Rate MeasurementOSAMANo ratings yet
- Brisk Lumbini RWA Membership FormDocument1 pageBrisk Lumbini RWA Membership FormTelus InternationalNo ratings yet
- Electromagnetic Interference (EMI) in Power SuppliesDocument41 pagesElectromagnetic Interference (EMI) in Power SuppliesAmarnath M DamodaranNo ratings yet
- Accounting Chapter 5: Internal Control, Cash and Receivables 1. Accounts & Notes ReveivableDocument7 pagesAccounting Chapter 5: Internal Control, Cash and Receivables 1. Accounts & Notes ReveivableMarine De CocquéauNo ratings yet
- Andrew Mickunas - Teaching Resume PortfolioDocument3 pagesAndrew Mickunas - Teaching Resume PortfolioAndrewNo ratings yet
- Scania Annual and Sustainability Report 2017Document138 pagesScania Annual and Sustainability Report 2017Wahidin UmarNo ratings yet
- Almario, Rich L. - InvestmentDocument6 pagesAlmario, Rich L. - InvestmentRich Lopez AlmarioNo ratings yet
- Design Thinking WorksheetDocument5 pagesDesign Thinking Worksheetsujal patel100% (1)
- The Impact of Food Branding On Children's Eating Behaviour and ObesityDocument8 pagesThe Impact of Food Branding On Children's Eating Behaviour and ObesityAlessandraBattagliaNo ratings yet
- Epoxy Curing Agents and Modifiers: Ancamide® 260A Curing AgentDocument1 pageEpoxy Curing Agents and Modifiers: Ancamide® 260A Curing AgentNissim Hazar CasanovaNo ratings yet
- China and EnvironmentDocument2 pagesChina and EnvironmentAndrea CalcagniNo ratings yet
- Solute Inputs in The Salar de Atacama (N. Chile) : V. Carmona, J.J. Pueyo, C. Taberner, G. Chong, M. ThirlwallDocument4 pagesSolute Inputs in The Salar de Atacama (N. Chile) : V. Carmona, J.J. Pueyo, C. Taberner, G. Chong, M. ThirlwallJosue FerretNo ratings yet
- CsToCpp ASomewhatShortGuide PDFDocument56 pagesCsToCpp ASomewhatShortGuide PDFIldar SakhapovNo ratings yet
- Influence of Humic Acid Application On Onion Growth Characteristics Under Water Deficit ConditionsDocument12 pagesInfluence of Humic Acid Application On Onion Growth Characteristics Under Water Deficit ConditionsMohammad Kazem souriNo ratings yet
- Task 1 - PCK8Document8 pagesTask 1 - PCK8Andrea SantosNo ratings yet
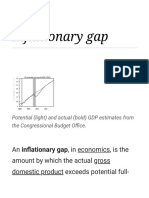
- Inflationary Gap - WikipediaDocument15 pagesInflationary Gap - WikipediaKush KumarNo ratings yet
- Manual Del Gemcom Surpac - Underground Ring DesignDocument43 pagesManual Del Gemcom Surpac - Underground Ring DesignDavid GarciaNo ratings yet
- Professional Diploma in Marketing: Reading List 2011 - 2012Document6 pagesProfessional Diploma in Marketing: Reading List 2011 - 2012yaqub19799141100% (1)
- Meter Reading Details: Assam Power Distribution Company LimitedDocument1 pageMeter Reading Details: Assam Power Distribution Company LimitedPadum PatowaryNo ratings yet
- Data Loss PreventionDocument6 pagesData Loss Preventionrajesh kesariNo ratings yet
- NoSleep Ebook - 2014, Issue 2 - NoSleep PDFDocument76 pagesNoSleep Ebook - 2014, Issue 2 - NoSleep PDFSofiiBaudeanNo ratings yet
- OpAudCh02 CBET 01 501E ToraldeMa - KristineE.Document4 pagesOpAudCh02 CBET 01 501E ToraldeMa - KristineE.Kristine Esplana ToraldeNo ratings yet
- D16 DipIFR Answers PDFDocument8 pagesD16 DipIFR Answers PDFAnonymous QtUcPzCANo ratings yet
- Solar Water Use Issues in SouthwestDocument20 pagesSolar Water Use Issues in Southwestpthakur234No ratings yet
- Switching Theory and Logic DesignDocument2 pagesSwitching Theory and Logic DesignManjunath BadigerNo ratings yet
- Daily Lesson Log: Monday Tuesday Wednesday Thursday FridayDocument5 pagesDaily Lesson Log: Monday Tuesday Wednesday Thursday FridayRienaly Bustamante100% (1)










































































Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Aws D8.1M 2013Document40 pagesAws D8.1M 2013vishesh dharaiya100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Name Programme SignatureDocument2 pagesName Programme SignatureJr. CesingNo ratings yet
- Report On Adm.&SupervisionDocument37 pagesReport On Adm.&SupervisionJr. Cesing100% (1)
- Honor & RespectDocument17 pagesHonor & RespectJr. CesingNo ratings yet
- Cardiac Leptospirosis: Iralphuaborque Md14thbatch Hds DocharlabardaDocument15 pagesCardiac Leptospirosis: Iralphuaborque Md14thbatch Hds DocharlabardaJr. CesingNo ratings yet
- Catechism of The Catholic Church: Chapter One: Man'S Capacity For GodDocument7 pagesCatechism of The Catholic Church: Chapter One: Man'S Capacity For GodJr. CesingNo ratings yet
- Catechism of The Catholic Church: Chapter One: Man'S Capacity For GodDocument7 pagesCatechism of The Catholic Church: Chapter One: Man'S Capacity For GodJr. CesingNo ratings yet
- SilenceDocument24 pagesSilenceJr. CesingNo ratings yet
- Bed 2nd Sem ResultDocument1 pageBed 2nd Sem ResultAnusree PranavamNo ratings yet
- Base Institute - Namakkal - PH: 900 37 111 66: - Mock - Ibpsguide.in - 1Document288 pagesBase Institute - Namakkal - PH: 900 37 111 66: - Mock - Ibpsguide.in - 1Kartik MaheshwariNo ratings yet
- Sop-10 Dose Rate MeasurementDocument3 pagesSop-10 Dose Rate MeasurementOSAMANo ratings yet
- Brisk Lumbini RWA Membership FormDocument1 pageBrisk Lumbini RWA Membership FormTelus InternationalNo ratings yet
- Electromagnetic Interference (EMI) in Power SuppliesDocument41 pagesElectromagnetic Interference (EMI) in Power SuppliesAmarnath M DamodaranNo ratings yet
- Accounting Chapter 5: Internal Control, Cash and Receivables 1. Accounts & Notes ReveivableDocument7 pagesAccounting Chapter 5: Internal Control, Cash and Receivables 1. Accounts & Notes ReveivableMarine De CocquéauNo ratings yet
- Andrew Mickunas - Teaching Resume PortfolioDocument3 pagesAndrew Mickunas - Teaching Resume PortfolioAndrewNo ratings yet
- Scania Annual and Sustainability Report 2017Document138 pagesScania Annual and Sustainability Report 2017Wahidin UmarNo ratings yet
- Almario, Rich L. - InvestmentDocument6 pagesAlmario, Rich L. - InvestmentRich Lopez AlmarioNo ratings yet
- Design Thinking WorksheetDocument5 pagesDesign Thinking Worksheetsujal patel100% (1)
- The Impact of Food Branding On Children's Eating Behaviour and ObesityDocument8 pagesThe Impact of Food Branding On Children's Eating Behaviour and ObesityAlessandraBattagliaNo ratings yet
- Epoxy Curing Agents and Modifiers: Ancamide® 260A Curing AgentDocument1 pageEpoxy Curing Agents and Modifiers: Ancamide® 260A Curing AgentNissim Hazar CasanovaNo ratings yet
- China and EnvironmentDocument2 pagesChina and EnvironmentAndrea CalcagniNo ratings yet
- Solute Inputs in The Salar de Atacama (N. Chile) : V. Carmona, J.J. Pueyo, C. Taberner, G. Chong, M. ThirlwallDocument4 pagesSolute Inputs in The Salar de Atacama (N. Chile) : V. Carmona, J.J. Pueyo, C. Taberner, G. Chong, M. ThirlwallJosue FerretNo ratings yet
- CsToCpp ASomewhatShortGuide PDFDocument56 pagesCsToCpp ASomewhatShortGuide PDFIldar SakhapovNo ratings yet
- Influence of Humic Acid Application On Onion Growth Characteristics Under Water Deficit ConditionsDocument12 pagesInfluence of Humic Acid Application On Onion Growth Characteristics Under Water Deficit ConditionsMohammad Kazem souriNo ratings yet
- Task 1 - PCK8Document8 pagesTask 1 - PCK8Andrea SantosNo ratings yet
- Inflationary Gap - WikipediaDocument15 pagesInflationary Gap - WikipediaKush KumarNo ratings yet
- Manual Del Gemcom Surpac - Underground Ring DesignDocument43 pagesManual Del Gemcom Surpac - Underground Ring DesignDavid GarciaNo ratings yet
- Professional Diploma in Marketing: Reading List 2011 - 2012Document6 pagesProfessional Diploma in Marketing: Reading List 2011 - 2012yaqub19799141100% (1)
- Meter Reading Details: Assam Power Distribution Company LimitedDocument1 pageMeter Reading Details: Assam Power Distribution Company LimitedPadum PatowaryNo ratings yet
- Data Loss PreventionDocument6 pagesData Loss Preventionrajesh kesariNo ratings yet
- NoSleep Ebook - 2014, Issue 2 - NoSleep PDFDocument76 pagesNoSleep Ebook - 2014, Issue 2 - NoSleep PDFSofiiBaudeanNo ratings yet
- OpAudCh02 CBET 01 501E ToraldeMa - KristineE.Document4 pagesOpAudCh02 CBET 01 501E ToraldeMa - KristineE.Kristine Esplana ToraldeNo ratings yet
- D16 DipIFR Answers PDFDocument8 pagesD16 DipIFR Answers PDFAnonymous QtUcPzCANo ratings yet
- Solar Water Use Issues in SouthwestDocument20 pagesSolar Water Use Issues in Southwestpthakur234No ratings yet
- Switching Theory and Logic DesignDocument2 pagesSwitching Theory and Logic DesignManjunath BadigerNo ratings yet
- Daily Lesson Log: Monday Tuesday Wednesday Thursday FridayDocument5 pagesDaily Lesson Log: Monday Tuesday Wednesday Thursday FridayRienaly Bustamante100% (1)