Download as pdf or txt
You might also like
- MI40-X - Nutrition GuideDocument12 pagesMI40-X - Nutrition GuideJoe Merengues100% (2)
- Anesthetic Formulation of Tumescent SolutionsDocument9 pagesAnesthetic Formulation of Tumescent SolutionsJorgeNo ratings yet
- Drug Study (Lidocaine HCL) - TorresDocument6 pagesDrug Study (Lidocaine HCL) - TorresbabiNo ratings yet
- Hallucinogens As Medicine - R. GriffithsDocument4 pagesHallucinogens As Medicine - R. GriffithsHans OrangenbaumNo ratings yet
- Pantoprazole DrugDocument1 pagePantoprazole Drugman12No ratings yet
- Tic BookDocument19 pagesTic BookPersis NairNo ratings yet
- Guideline On Use of Local Anesthesia For Pediatric Dental PatientsDocument7 pagesGuideline On Use of Local Anesthesia For Pediatric Dental PatientsLisna K. RezkyNo ratings yet
- Local Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryDocument8 pagesLocal Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryFrancisco Javier Rodriguez MolinaNo ratings yet
- Local Anaesthetic AgentsDocument21 pagesLocal Anaesthetic AgentsSuresh KumarNo ratings yet
- Local AnaestheticsDocument26 pagesLocal Anaestheticsv_vijayakanth7656No ratings yet
- LidocaineDocument3 pagesLidocainebrittNo ratings yet
- Lidocaine and Pain Management in The Emergency Department: A Review ArticleDocument6 pagesLidocaine and Pain Management in The Emergency Department: A Review ArticlesarahnblaNo ratings yet
- Accepted Manuscript: 10.1016/j.amjoto.2018.03.023Document7 pagesAccepted Manuscript: 10.1016/j.amjoto.2018.03.023Mazi KamaliNo ratings yet
- Apexa No 7Document4 pagesApexa No 7Apexa YadavNo ratings yet
- Local Anesthesia in Large AnimalsDocument53 pagesLocal Anesthesia in Large AnimalsNot SayingNo ratings yet
- G Localanesthesia PDFDocument7 pagesG Localanesthesia PDFmanusiaNo ratings yet
- An Update On Local Anesthesia For Pediatric Dental PatientsDocument10 pagesAn Update On Local Anesthesia For Pediatric Dental Patientsdil aawazNo ratings yet
- LidocaineDocument4 pagesLidocaineFikrianisa SafrinaNo ratings yet
- Local Anesthetic AgentDocument21 pagesLocal Anesthetic AgentSiti Fatimah IsmailNo ratings yet
- Jurnal Kelompok AnestesiDocument44 pagesJurnal Kelompok AnestesiAndrean MartinNo ratings yet
- Administration of LidocaineDocument6 pagesAdministration of Lidocainecookie onganizaNo ratings yet
- AnesthesiaDocument18 pagesAnesthesiaZakria Al-HadadNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Lidocaine Plus Insert Correction Update 31-03-2022Document2 pagesLidocaine Plus Insert Correction Update 31-03-2022Kamrunnahar SwornaNo ratings yet
- Effect of "Lidocaine" Infusion On Sevoflurane Requirement During Bis Guided SurgeryDocument10 pagesEffect of "Lidocaine" Infusion On Sevoflurane Requirement During Bis Guided SurgeryTJPRC PublicationsNo ratings yet
- DIH LidocaineDocument21 pagesDIH LidocaineMuamar Abdillah14No ratings yet
- Analgesic Constant Rate InfusiónDocument7 pagesAnalgesic Constant Rate InfusiónOlga Lucia Duque QuijanoNo ratings yet
- Opiod Free For AnesthesiaDocument5 pagesOpiod Free For AnesthesiaburhangunawanNo ratings yet
- Complications of Local AnesthesiaDocument80 pagesComplications of Local AnesthesiaRiya JainNo ratings yet
- 6 Regional AnaesthesiaDocument12 pages6 Regional AnaesthesiasaniaaNo ratings yet
- Guideline On Use of Local Anesthesia For Pediatric Dental PatientsDocument7 pagesGuideline On Use of Local Anesthesia For Pediatric Dental PatientsJacoboGonzález100% (1)
- S 025 LBLDocument11 pagesS 025 LBLPradeep Mathew VargheseNo ratings yet
- Lidocaine HydrochlorideDocument12 pagesLidocaine HydrochlorideShivam VinothNo ratings yet
- Systemic Lidocaine For Perioperative Analgesia A LDocument9 pagesSystemic Lidocaine For Perioperative Analgesia A LWahyu Syahrul RamadhanNo ratings yet
- Diclofenac Sodium Ophthalmic Solution, 0.1%: CL NaocchDocument2 pagesDiclofenac Sodium Ophthalmic Solution, 0.1%: CL NaocchBechchar HichamNo ratings yet
- Bupivacaine (Marcaine)Document2 pagesBupivacaine (Marcaine)Michalis SpyridakisNo ratings yet
- Zorcaine MonographDocument18 pagesZorcaine Monographwakeupinday1ayNo ratings yet
- Airwayanesthesia: Theory and PracticeDocument14 pagesAirwayanesthesia: Theory and PracticeJEFFERSON MUÑOZNo ratings yet
- Local Anesthesia - Definition of Local Anesthesia in The Medical Dictionary - by The Free Online Medical Dictionary, Thesaurus and EncyclopediaDocument10 pagesLocal Anesthesia - Definition of Local Anesthesia in The Medical Dictionary - by The Free Online Medical Dictionary, Thesaurus and EncyclopediaAkhilesh PipadaNo ratings yet
- Local Anesthesia in Pediatric DentistryDocument70 pagesLocal Anesthesia in Pediatric DentistryNicky Romeo100% (1)
- Local AnesthesiaDocument63 pagesLocal AnesthesiaReda IsmaeelNo ratings yet
- Pharmoclogy Lit Review 1Document5 pagesPharmoclogy Lit Review 1api-663993558No ratings yet
- Basics: Constant-Rate Infusions: Each Class of Drug Works On A Different Aspect of The Pain PathwayDocument7 pagesBasics: Constant-Rate Infusions: Each Class of Drug Works On A Different Aspect of The Pain PathwayBibek SutradharNo ratings yet
- Use of Local Anesthesia For Pediatric Dental PatientsDocument11 pagesUse of Local Anesthesia For Pediatric Dental PatientsMuhammad Fahry AladjaiNo ratings yet
- Safari - 21 Agt 2018 18.00 PDFDocument1 pageSafari - 21 Agt 2018 18.00 PDFCeriaindriasariNo ratings yet
- TDM of LidocaineDocument19 pagesTDM of LidocaineNikkiiNo ratings yet
- Anestesi Lokal Pada Lesi Superfisial: Huntal NapoleonDocument12 pagesAnestesi Lokal Pada Lesi Superfisial: Huntal NapoleonshevinesaNo ratings yet
- Drugs Study ER LEAD Drug (Yntig)Document5 pagesDrugs Study ER LEAD Drug (Yntig)Herbert Almendras HuyoNo ratings yet
- Complications Associated With Local Anesthesia inDocument25 pagesComplications Associated With Local Anesthesia inAli YehyaNo ratings yet
- Xylocaine Dentaland AdrenalineDocument7 pagesXylocaine Dentaland Adrenalinefawwaz FofoNo ratings yet
- 5 Drug StudyDocument14 pages5 Drug StudyJennyLapitan100% (2)
- DIPROSPAN Sterile Aqueous Suspension: DescriptionDocument6 pagesDIPROSPAN Sterile Aqueous Suspension: DescriptionAbet AtienzaNo ratings yet
- The Use of Intravenous Lidocaine For Postoperative Pain and Recovery: International Consensus Statement On Ef Ficacy and SafetyDocument13 pagesThe Use of Intravenous Lidocaine For Postoperative Pain and Recovery: International Consensus Statement On Ef Ficacy and SafetyReynaldo Canelles RodriguezNo ratings yet
- Intralesional CorticosteroidsDocument8 pagesIntralesional Corticosteroidssidrahbaloch94No ratings yet
- WWW - Fda.gov/medwatch: Reference ID: 3924387Document8 pagesWWW - Fda.gov/medwatch: Reference ID: 3924387Attaufiq IrawanNo ratings yet
- Injeksi IntravitrealDocument16 pagesInjeksi IntravitrealindahNo ratings yet
- Injeksi IntravitrealDocument16 pagesInjeksi IntravitrealindahNo ratings yet
- Emergency Kit Module 2Document27 pagesEmergency Kit Module 2Amit GaurNo ratings yet
- What Are Current Recommendations For Treatment of Drug ExtravasationDocument13 pagesWhat Are Current Recommendations For Treatment of Drug ExtravasationThắng NguyễnNo ratings yet
- Local Anesthesia AdvancesDocument61 pagesLocal Anesthesia AdvancesMugdha FrancisNo ratings yet
- 20197.LocalAnestheticsinPediatricDental PpracticeDocument6 pages20197.LocalAnestheticsinPediatricDental PpracticeLaxmi VermaNo ratings yet
- M S B U P T K L P K: Social Cultural Problems in Tuberculosis Respective Effort in Lima Puluh Kota RegencyDocument7 pagesM S B U P T K L P K: Social Cultural Problems in Tuberculosis Respective Effort in Lima Puluh Kota Regency<_>No ratings yet
- Difference Between Rheumatic Heart Disease and Infective EndocarditisDocument7 pagesDifference Between Rheumatic Heart Disease and Infective Endocarditis<_>No ratings yet
- ANFISDocument3 pagesANFIS<_>No ratings yet
- AnorexiaDocument1 pageAnorexia<_>No ratings yet
- Urological InfectionsDocument21 pagesUrological Infections<_>No ratings yet
- Sumber: Urinalysis and Body Fluid 6 EditionDocument1 pageSumber: Urinalysis and Body Fluid 6 Edition<_>No ratings yet
- ChocolateDocument1 pageChocolate<_>No ratings yet
- Am HCW Safety enDocument2 pagesAm HCW Safety en<_>No ratings yet
- Guideline Resucitation DrowningDocument4 pagesGuideline Resucitation Drowning<_>No ratings yet
- Figure A-23: Isolation of LymphocytesDocument15 pagesFigure A-23: Isolation of Lymphocytes<_>No ratings yet
- Art:10.1186/1471 2393 14 337 PDFDocument10 pagesArt:10.1186/1471 2393 14 337 PDF<_>No ratings yet
- Ask The Kamen Rider Characters: HumorDocument46 pagesAsk The Kamen Rider Characters: Humor<_>No ratings yet
- Pathobiology/Agents Incubation Period Vomiting Abdominal Pain Fever DiarrheaDocument4 pagesPathobiology/Agents Incubation Period Vomiting Abdominal Pain Fever Diarrhea<_>No ratings yet
- Postgraduate Programs Summary Table: Australian School of BusinessDocument5 pagesPostgraduate Programs Summary Table: Australian School of Business<_>No ratings yet
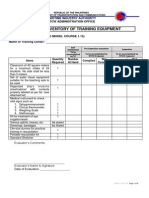
- Form 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDocument9 pagesForm 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDemp AlmiranezNo ratings yet
- A Comparison of Human Dental Pulp Response To CalcDocument5 pagesA Comparison of Human Dental Pulp Response To CalcrespikNo ratings yet
- Usmle MSKDocument12 pagesUsmle MSKstruzzNo ratings yet
- Common ENT ComplaintsDocument9 pagesCommon ENT ComplaintsHo Yong WaiNo ratings yet
- Physical and Physiological Effects of UltrasoundDocument2 pagesPhysical and Physiological Effects of UltrasoundKrissy WilhelmsenNo ratings yet
- Jebah Hospital: The Crimson Press Curriculum Center The Crimson Group, IncDocument8 pagesJebah Hospital: The Crimson Press Curriculum Center The Crimson Group, IncLian EspinoNo ratings yet
- Concept of MiasmDocument4 pagesConcept of MiasmCristinaNo ratings yet
- S1 2016 316037 BibliographyDocument6 pagesS1 2016 316037 BibliographyfikriNo ratings yet
- WC Guideline ProcedureDocument9 pagesWC Guideline ProcedureVarlam CristaviNo ratings yet
- Fulltext Schizophrenia v4 Id1033Document4 pagesFulltext Schizophrenia v4 Id1033Awaluddin MisrangNo ratings yet
- Determinants of Leptospirosis in Bayambang, Pangasinan: An Input To A Community-Based Epidemiological ProgramDocument6 pagesDeterminants of Leptospirosis in Bayambang, Pangasinan: An Input To A Community-Based Epidemiological ProgramJamesBatholomewNo ratings yet
- Mark Scheme (Results) June 2011: GCE Biology (6BI01) Paper 01Document20 pagesMark Scheme (Results) June 2011: GCE Biology (6BI01) Paper 01BooksNo ratings yet
- Biochemical Oxygen Demand or Biological Oxygen DemandDocument3 pagesBiochemical Oxygen Demand or Biological Oxygen DemandEllieNo ratings yet
- RESEARCH 2 - Project Research ProposalDocument11 pagesRESEARCH 2 - Project Research ProposalFranchesca LouiseNo ratings yet
- Sikagard - 701W: Alkylalkoxy Siloxane Micro-Emulsion Water Repellent ImpregnationDocument2 pagesSikagard - 701W: Alkylalkoxy Siloxane Micro-Emulsion Water Repellent Impregnationthe pilotNo ratings yet
- Vitamin K: Wallflower Sister of The FamousDocument3 pagesVitamin K: Wallflower Sister of The FamousbisanpaNo ratings yet
- CHN - TBDocument58 pagesCHN - TBStudentnurseMjNo ratings yet
- Diagnosis and Management of Pearly Penile PapulesDocument5 pagesDiagnosis and Management of Pearly Penile Papulesmamal malikaNo ratings yet
- The Origin of The Solution-Focused Approach PDFDocument8 pagesThe Origin of The Solution-Focused Approach PDFMirela Cojocaru StetcoNo ratings yet
- CSTDA Service Application Form 20200615Document5 pagesCSTDA Service Application Form 20200615Autumn DrueNo ratings yet
- ErythromycinDocument2 pagesErythromycinEurielle MioleNo ratings yet
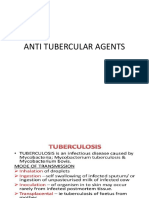
- Anti TBDocument68 pagesAnti TBGunjan YadavNo ratings yet
- Wrap (Wellness Recovery Action Plan) Western AustraliaDocument4 pagesWrap (Wellness Recovery Action Plan) Western AustraliagavinbuzzNo ratings yet
- Clin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyDocument7 pagesClin Psychology and Psychoth - 2017 - Durá Ferrandis - Confirming The Mechanisms Behind Cognitive Behavioural TherapyNatalie JaraNo ratings yet
- 2010 TNM Staging Colorectal CADocument2 pages2010 TNM Staging Colorectal CAbubbrubb20063998No ratings yet
- History of Surgery: Esperanza R. Lahoz, MD, FPCS, FpsgsDocument52 pagesHistory of Surgery: Esperanza R. Lahoz, MD, FPCS, Fpsgs2BCASTILLO FITZ GERALDPNo ratings yet