Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- General - GITDocument90 pagesGeneral - GITAbdallah Gamal100% (1)
- PolycythemiaDocument22 pagesPolycythemiaIrman DinejadNo ratings yet
- Banco Kap. - CK 2Document1,099 pagesBanco Kap. - CK 2Lucas OrtizNo ratings yet
- Nephrotic Syndrome in ChildrenDocument36 pagesNephrotic Syndrome in ChildrenMalueth AnguiNo ratings yet
- NCLEX QuestionsDocument5 pagesNCLEX QuestionsTindo Esa SariNo ratings yet
- Occurrence of Infection Among Children With Nephrotic Syndrome During HospitalizationsDocument8 pagesOccurrence of Infection Among Children With Nephrotic Syndrome During HospitalizationsViswas ChhapolaNo ratings yet
- Ginkgo BilobaDocument19 pagesGinkgo Bilobafarmasi_hm100% (1)
- Brochure Finecare Plus Fs-114Document2 pagesBrochure Finecare Plus Fs-114lumira Bogota100% (2)
- Step 2 - Notes On Questions From USMLE WorldDocument16 pagesStep 2 - Notes On Questions From USMLE Worldbhav17z100% (1)
- Deep Vein Thrombosis: P Resenter - Dr. SAMRAT SHRESTHADocument69 pagesDeep Vein Thrombosis: P Resenter - Dr. SAMRAT SHRESTHAUsmle GuyNo ratings yet
- Deep Vein ThrombosisDocument3 pagesDeep Vein ThrombosisAnonymous cwRgUKv2MQ100% (1)
- The Most CommonsDocument80 pagesThe Most CommonsJmee8No ratings yet
- Ajovy - Fremanezumab - Drug Information - UpToDateDocument6 pagesAjovy - Fremanezumab - Drug Information - UpToDateDiana PhamNo ratings yet
- Stroke - Etiology, Classification, and Epidemiology - UpToDateDocument34 pagesStroke - Etiology, Classification, and Epidemiology - UpToDateSamanta MedinillaNo ratings yet
- CVA JroozDocument5 pagesCVA JroozEdmonLagartoNo ratings yet
- Icd 10Document78 pagesIcd 10KumarNo ratings yet
- UCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Document5 pagesUCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Olguita Huaccha PastorNo ratings yet
- Spherocytosis & Increased Risk of Thrombosis. Kam Newman, Mojtaba Akhtari, Salim Shakour, Shahriar DadkhahDocument1 pageSpherocytosis & Increased Risk of Thrombosis. Kam Newman, Mojtaba Akhtari, Salim Shakour, Shahriar DadkhahjingerbrunoNo ratings yet
- Lab7 Circulatory DisturbancesDocument13 pagesLab7 Circulatory DisturbancesSoon SheedNo ratings yet
- GP Exam Compiled 1st BiDocument136 pagesGP Exam Compiled 1st BiCherry RahimaNo ratings yet
- Articles On Wheat ToxicityDocument96 pagesArticles On Wheat ToxicityDr. Heath MotleyNo ratings yet
- Lecture On Hemodynamic and Thromboembolic DisordersDocument77 pagesLecture On Hemodynamic and Thromboembolic DisordersCharmaine Torio PastorNo ratings yet
- General Pathology - Topical Past Papers-1Document21 pagesGeneral Pathology - Topical Past Papers-1RazaNo ratings yet
- Vet PathologyDocument128 pagesVet PathologyMegarsaNo ratings yet
- Ischemic Heart Disease NotesDocument8 pagesIschemic Heart Disease NotesDr. Tarush DhawanNo ratings yet
- Diagnosa PRBDocument12 pagesDiagnosa PRBSAEHANNo ratings yet
- Visceral RenalDocument120 pagesVisceral RenalShivik PatelNo ratings yet
- Acute Mesenteric IschemiaDocument46 pagesAcute Mesenteric Ischemiashita febrianaNo ratings yet
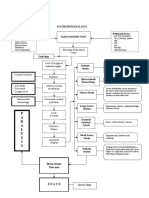
- Pathophysiology: P A R A L Y S I SDocument1 pagePathophysiology: P A R A L Y S I SJordan Garcia AguilarNo ratings yet
- Frequently Prescribed DrugsDocument47 pagesFrequently Prescribed DrugsMahogony ScottNo ratings yet