Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pharmaceutical Unit Operation (Solid Dosage)Document8 pagesPharmaceutical Unit Operation (Solid Dosage)Sangram KendreNo ratings yet
- Data Source Book P-7475HDocument51 pagesData Source Book P-7475HJoão13@No ratings yet
- Unit 3 Pressure GaugeDocument11 pagesUnit 3 Pressure GaugeUv sai likithNo ratings yet
- Polyacrylamide Based Breathable Coating For Cotton Fabric: N S. S, M J A K. ADocument20 pagesPolyacrylamide Based Breathable Coating For Cotton Fabric: N S. S, M J A K. AVinnawati SetiadiNo ratings yet
- Is.15656.2006 - Hazard Identification and Risk AssessmentDocument31 pagesIs.15656.2006 - Hazard Identification and Risk Assessmentjitesh26100% (3)
- CasiñoJeanne Pearl 2H1 Experiment 1 Laboratory ReportDocument9 pagesCasiñoJeanne Pearl 2H1 Experiment 1 Laboratory ReportJeanne Pearl CasiñoNo ratings yet
- Basics of Paste Backfill SystemsDocument5 pagesBasics of Paste Backfill Systemsalvaroaac4100% (1)
- Chemistry Form-Four (Chapters Summery of Questions With Answers)Document13 pagesChemistry Form-Four (Chapters Summery of Questions With Answers)Mohamed Abuukar AbdukadirNo ratings yet
- Criteria For Chemical Equilibrium With Application To Methane Steam ReformingDocument7 pagesCriteria For Chemical Equilibrium With Application To Methane Steam ReformingteeeeeeeeeeeeeeeeeeeeeeeeeeeeettNo ratings yet
- 2018al BassamAZMHPhDDocument224 pages2018al BassamAZMHPhDFloren Ardila AlvaradoNo ratings yet
- Adoc - Pub - Ewf10932 Ewf10932s Ewf12732 Ewf12732s in VI MesinDocument104 pagesAdoc - Pub - Ewf10932 Ewf10932s Ewf12732 Ewf12732s in VI MesinSơn PhạmNo ratings yet
- Power and WiringDocument82 pagesPower and WiringABELWALIDNo ratings yet
- Drug Discovery by DesignDocument143 pagesDrug Discovery by DesignRieke Azhar0% (1)
- PROBES-75 Guidelines For Developing GreenbeltsDocument210 pagesPROBES-75 Guidelines For Developing Greenbeltsgreymatter2012No ratings yet
- 2.3 Steam SDocument58 pages2.3 Steam Saravind grandhiNo ratings yet
- Soil Science 1 - Soil Genesis Ronel RobertoDocument21 pagesSoil Science 1 - Soil Genesis Ronel RobertoMalikah AliNo ratings yet
- M15021 Leucidal Liquid PT Technical Data Sheet v6Document3 pagesM15021 Leucidal Liquid PT Technical Data Sheet v6Molly0630No ratings yet
- File-Sensus Model 243 RegulatorDocument12 pagesFile-Sensus Model 243 RegulatorNaNo RegentNo ratings yet
- Rotary Lobe Pump Mechanical Seal SelectionDocument2 pagesRotary Lobe Pump Mechanical Seal SelectionSachin HolkarNo ratings yet
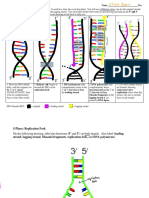
- Elijah James - 35-DNA Replication Worksheet - CompleteDocument4 pagesElijah James - 35-DNA Replication Worksheet - CompleteElijah JamesNo ratings yet
- Zinc-5 % Aluminum-Mischmetal Alloy-Coated Steel Overhead Ground Wire StrandDocument3 pagesZinc-5 % Aluminum-Mischmetal Alloy-Coated Steel Overhead Ground Wire StrandJosé Ramón GutierrezNo ratings yet
- Lesson 11 Activity 1 Thermal ExpansionDocument18 pagesLesson 11 Activity 1 Thermal ExpansionEthel WenceslaoNo ratings yet
- Banned DrugsDocument28 pagesBanned DrugsSanjeev Singh100% (1)
- Analytical Chemistry PDFDocument253 pagesAnalytical Chemistry PDFJerome MamauagNo ratings yet
- Mark Scheme (Results) Summer 2019Document17 pagesMark Scheme (Results) Summer 2019Alaska DavisNo ratings yet
- Fire DiamondDocument33 pagesFire DiamondArun HarpalaniNo ratings yet
- CSP10 Blueprint ReferencesDocument5 pagesCSP10 Blueprint ReferencesFuzail AyazNo ratings yet
- Sludge Drying PDFDocument10 pagesSludge Drying PDFdanndiamondNo ratings yet
- WPS (1) 1Document5 pagesWPS (1) 1Pedro José PadillaNo ratings yet
- Pioneer ScopeDocument85 pagesPioneer ScopeArchana ShuklaNo ratings yet