
Satria Adi
Satria Adi
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- POEA Contract For SeafarersDocument40 pagesPOEA Contract For SeafarersSto Cu100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ArdsDocument53 pagesArdsSophy Sony100% (3)
- SBLII Prop Bet SheetDocument32 pagesSBLII Prop Bet SheetMárk György KisNo ratings yet
- Satria AdiDocument14 pagesSatria AdiSatria Adi PutraNo ratings yet
- DXA in Adults: The Challenge of DiagnosisDocument4 pagesDXA in Adults: The Challenge of DiagnosisSatria Adi PutraNo ratings yet
- Basic Principles and Technical Considerations: Radiographic AbsorptiometryDocument10 pagesBasic Principles and Technical Considerations: Radiographic AbsorptiometrySatria Adi PutraNo ratings yet
- Bed Positioning For Stroke Patients: A. Lying On Your Back or SittingDocument1 pageBed Positioning For Stroke Patients: A. Lying On Your Back or SittingSatria Adi PutraNo ratings yet
- Satria AdiDocument13 pagesSatria AdiSatria Adi PutraNo ratings yet
- Paper Template For 2nd ASEAN Academic Society International ConferenceDocument3 pagesPaper Template For 2nd ASEAN Academic Society International ConferenceSatria Adi PutraNo ratings yet
- Satria Adi PutraDocument83 pagesSatria Adi PutraSatria Adi PutraNo ratings yet
- Article DHEA and AntiagingDocument2 pagesArticle DHEA and AntiagingSatria Adi PutraNo ratings yet
- Basic College Mathematics 6th Edition Martin Gay Solutions ManualDocument35 pagesBasic College Mathematics 6th Edition Martin Gay Solutions Manualbiggenabodement2jb8100% (26)
- Rengoera Lave Vaisselle Encastrable Ikea 300 - AA 2192023 3 1Document64 pagesRengoera Lave Vaisselle Encastrable Ikea 300 - AA 2192023 3 1adamNo ratings yet
- P & I Club InsuranceDocument20 pagesP & I Club Insurancesxy_sadiNo ratings yet
- Nuisance 161030205655 PDFDocument26 pagesNuisance 161030205655 PDFSimranNo ratings yet
- Nursing Case Study of Electric Burn Injury (Edit Nisa) Sdah Di Edit New 2Document38 pagesNursing Case Study of Electric Burn Injury (Edit Nisa) Sdah Di Edit New 2Rizal AhmadNo ratings yet
- Gingivaltissuemanagement 090723132044 Phpapp02Document17 pagesGingivaltissuemanagement 090723132044 Phpapp02Priya IngaleNo ratings yet
- Anatomi BahuDocument4 pagesAnatomi BahuSheila Setiawati TanzilNo ratings yet
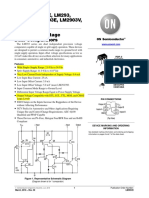
- LM393, LM393E, LM293, LM2903, LM2903E, LM2903V, NCV2903 Low Offset Voltage Dual ComparatorsDocument10 pagesLM393, LM393E, LM293, LM2903, LM2903E, LM2903V, NCV2903 Low Offset Voltage Dual Comparatorssam2No ratings yet
- Department of Orthopaedics KMC, Mangalore: Ankle ArthrodesisDocument8 pagesDepartment of Orthopaedics KMC, Mangalore: Ankle ArthrodesiscmonmanNo ratings yet
- Manual de Usuario ESpace 7910 IP PhoneDocument115 pagesManual de Usuario ESpace 7910 IP PhoneChris ThianNo ratings yet
- Spinal StenosisDocument14 pagesSpinal StenosisHONGJYNo ratings yet
- Baseball Fundamentals: Sasi KarupartiDocument12 pagesBaseball Fundamentals: Sasi Karupartisrk1221No ratings yet
- 10 1016@j Surg 2019 04 034Document7 pages10 1016@j Surg 2019 04 034amelia henitasariNo ratings yet
- Nervous System PresentationDocument22 pagesNervous System PresentationEnero Ombina PorlaresNo ratings yet
- G600 Inverter ManuelDocument225 pagesG600 Inverter ManuelBambang Wisnu100% (2)
- Categories of RestraintsDocument7 pagesCategories of RestraintsgireeshsachinNo ratings yet
- Paradigms of Oxygen Therapy in Critically Ill PatientsDocument6 pagesParadigms of Oxygen Therapy in Critically Ill Patientsdella psNo ratings yet
- Symptoms and Causes CataractsDocument5 pagesSymptoms and Causes CataractsEmma KalmanNo ratings yet
- CNS Mcqs PDFDocument12 pagesCNS Mcqs PDFSindhi Waseem BalochNo ratings yet
- Passive Movements: BY: Dr. Sonali DesaiDocument21 pagesPassive Movements: BY: Dr. Sonali DesaiBhargavNo ratings yet
- Gait Training (MIH Presentation)Document44 pagesGait Training (MIH Presentation)Jean Pascal AppadooNo ratings yet
- Flexural Strength Tests of Ceramics (SubsTech)Document3 pagesFlexural Strength Tests of Ceramics (SubsTech)mypenta2008No ratings yet
- Installation Manual: SYSTEM Inverter Air ConditionersDocument52 pagesInstallation Manual: SYSTEM Inverter Air ConditionersOscar DiazNo ratings yet
- Hemothorax - Background, Anatomy, Pathophysiology PDFDocument6 pagesHemothorax - Background, Anatomy, Pathophysiology PDFHendriawan PutraNo ratings yet
- 25 Western Guaranty v. CADocument1 page25 Western Guaranty v. CAMark Anthony Javellana SicadNo ratings yet
- Fire PreventionDocument45 pagesFire PreventionSyed IrfanNo ratings yet
- Ricoh DX2430Document124 pagesRicoh DX2430Amer Rafique89% (9)













































































Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- POEA Contract For SeafarersDocument40 pagesPOEA Contract For SeafarersSto Cu100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ArdsDocument53 pagesArdsSophy Sony100% (3)
- SBLII Prop Bet SheetDocument32 pagesSBLII Prop Bet SheetMárk György KisNo ratings yet
- Satria AdiDocument14 pagesSatria AdiSatria Adi PutraNo ratings yet
- DXA in Adults: The Challenge of DiagnosisDocument4 pagesDXA in Adults: The Challenge of DiagnosisSatria Adi PutraNo ratings yet
- Basic Principles and Technical Considerations: Radiographic AbsorptiometryDocument10 pagesBasic Principles and Technical Considerations: Radiographic AbsorptiometrySatria Adi PutraNo ratings yet
- Bed Positioning For Stroke Patients: A. Lying On Your Back or SittingDocument1 pageBed Positioning For Stroke Patients: A. Lying On Your Back or SittingSatria Adi PutraNo ratings yet
- Satria AdiDocument13 pagesSatria AdiSatria Adi PutraNo ratings yet
- Paper Template For 2nd ASEAN Academic Society International ConferenceDocument3 pagesPaper Template For 2nd ASEAN Academic Society International ConferenceSatria Adi PutraNo ratings yet
- Satria Adi PutraDocument83 pagesSatria Adi PutraSatria Adi PutraNo ratings yet
- Article DHEA and AntiagingDocument2 pagesArticle DHEA and AntiagingSatria Adi PutraNo ratings yet
- Basic College Mathematics 6th Edition Martin Gay Solutions ManualDocument35 pagesBasic College Mathematics 6th Edition Martin Gay Solutions Manualbiggenabodement2jb8100% (26)
- Rengoera Lave Vaisselle Encastrable Ikea 300 - AA 2192023 3 1Document64 pagesRengoera Lave Vaisselle Encastrable Ikea 300 - AA 2192023 3 1adamNo ratings yet
- P & I Club InsuranceDocument20 pagesP & I Club Insurancesxy_sadiNo ratings yet
- Nuisance 161030205655 PDFDocument26 pagesNuisance 161030205655 PDFSimranNo ratings yet
- Nursing Case Study of Electric Burn Injury (Edit Nisa) Sdah Di Edit New 2Document38 pagesNursing Case Study of Electric Burn Injury (Edit Nisa) Sdah Di Edit New 2Rizal AhmadNo ratings yet
- Gingivaltissuemanagement 090723132044 Phpapp02Document17 pagesGingivaltissuemanagement 090723132044 Phpapp02Priya IngaleNo ratings yet
- Anatomi BahuDocument4 pagesAnatomi BahuSheila Setiawati TanzilNo ratings yet
- LM393, LM393E, LM293, LM2903, LM2903E, LM2903V, NCV2903 Low Offset Voltage Dual ComparatorsDocument10 pagesLM393, LM393E, LM293, LM2903, LM2903E, LM2903V, NCV2903 Low Offset Voltage Dual Comparatorssam2No ratings yet
- Department of Orthopaedics KMC, Mangalore: Ankle ArthrodesisDocument8 pagesDepartment of Orthopaedics KMC, Mangalore: Ankle ArthrodesiscmonmanNo ratings yet
- Manual de Usuario ESpace 7910 IP PhoneDocument115 pagesManual de Usuario ESpace 7910 IP PhoneChris ThianNo ratings yet
- Spinal StenosisDocument14 pagesSpinal StenosisHONGJYNo ratings yet
- Baseball Fundamentals: Sasi KarupartiDocument12 pagesBaseball Fundamentals: Sasi Karupartisrk1221No ratings yet
- 10 1016@j Surg 2019 04 034Document7 pages10 1016@j Surg 2019 04 034amelia henitasariNo ratings yet
- Nervous System PresentationDocument22 pagesNervous System PresentationEnero Ombina PorlaresNo ratings yet
- G600 Inverter ManuelDocument225 pagesG600 Inverter ManuelBambang Wisnu100% (2)
- Categories of RestraintsDocument7 pagesCategories of RestraintsgireeshsachinNo ratings yet
- Paradigms of Oxygen Therapy in Critically Ill PatientsDocument6 pagesParadigms of Oxygen Therapy in Critically Ill Patientsdella psNo ratings yet
- Symptoms and Causes CataractsDocument5 pagesSymptoms and Causes CataractsEmma KalmanNo ratings yet
- CNS Mcqs PDFDocument12 pagesCNS Mcqs PDFSindhi Waseem BalochNo ratings yet
- Passive Movements: BY: Dr. Sonali DesaiDocument21 pagesPassive Movements: BY: Dr. Sonali DesaiBhargavNo ratings yet
- Gait Training (MIH Presentation)Document44 pagesGait Training (MIH Presentation)Jean Pascal AppadooNo ratings yet
- Flexural Strength Tests of Ceramics (SubsTech)Document3 pagesFlexural Strength Tests of Ceramics (SubsTech)mypenta2008No ratings yet
- Installation Manual: SYSTEM Inverter Air ConditionersDocument52 pagesInstallation Manual: SYSTEM Inverter Air ConditionersOscar DiazNo ratings yet
- Hemothorax - Background, Anatomy, Pathophysiology PDFDocument6 pagesHemothorax - Background, Anatomy, Pathophysiology PDFHendriawan PutraNo ratings yet
- 25 Western Guaranty v. CADocument1 page25 Western Guaranty v. CAMark Anthony Javellana SicadNo ratings yet
- Fire PreventionDocument45 pagesFire PreventionSyed IrfanNo ratings yet
- Ricoh DX2430Document124 pagesRicoh DX2430Amer Rafique89% (9)